Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
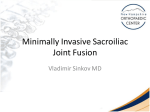
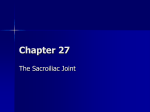
Percutaneous fusion of the sacroiliac joint with hollow modular anchorage screws CLINICAL AND RADIOLOGICAL OUTCOME A. Khurana, A. R. Guha, K. Mohanty, S. Ahuja From University Hospital of Wales, Cardiff, Wales A. Khurana, MRCS, MS, MSc, Specialist Registrar, Trauma & Orthopaedics A. R. Guha, FRCS, MS, Specialist Registrar, Trauma & Orthopaedics K. Mohanty, FRCS, FRCS(Orth), MSc, Consultant Orthopaedic Surgeon S. Ahuja, FRCS, FRCS(Orth), MSc, Consultant Orthopaedic Surgeon Department of Orthopaedics University Hospital of Wales, Heath Park, Cardiff & Vale NHS Trust, Cardiff CF14 4XW, UK. Correspondence should be sent to Mr A. Khurana at; e-mail: [email protected] ©2009 British Editorial Society of Bone and Joint Surgery doi:10.1302/0301-620X.91B5. 21519 $2.00 J Bone Joint Surg [Br] 2009;91-B:627-31. Received 8 July 2008; Accepted after revision 15 January 2009 VOL. 91-B, No. 5, MAY 2009 We reviewed 15 consecutive patients, 11 women and four men, with a mean age of 48.7 years (37.3 to 62.6), who between July 2004 and August 2007 had undergone percutaneous sacroiliac fusion using hollow modular anchorage screws filled with demineralised bone matrix. Each patient was carefully assessed to exclude other conditions and underwent preoperative CT and MR scans. The diagnosis of symptomatic sacroiliac disease was confirmed by an injection of local anaesthetic and steroid under image intensifier control. The short form-36 questionnaire and Majeed’s scoring system were used for pre- and post-operative functional evaluation. Post-operative radiological evaluation was performed using plain radiographs. Intra-operative blood loss was minimal and there were no post-operative clinical or radiological complications. The mean follow-up was for 17 months (9 to 39). The mean short form-36 scores improved from 37 (23 to 51) to 80 (67 to 92) for physical function and from 53 (34 to 73) to 86 (70 to 98) for general health (p = 0.037). The mean Majeed’s score improved from 37 (18 to 54) pre-operatively to 79 (63 to 96) post-operatively (p = 0.014). There were 13 good to excellent results. The remaining two patients improved in short form-36 from a mean of 29 (26 to 35) to 48 (44 to 52). Their persistent pain was probably due to concurrent lumbar pathology. We conclude that percutaneous hollow modular anchorage screws are a satisfactory method of achieving sacroiliac fusion. The sacroiliac joint may be the source of pain in 10% to 32% of patients presenting with low back pain.1,2 There is no consensus about the management of sacroiliac joint pain. Several methods of treatment have been described, with varying degrees of success.1,3,4 Operative treatment usually takes the form of sacroiliac fusion.5,6 Open arthrodesis has been described using the Smith-Petersen5 or a midline fascial-splitting approach,7 which can cause wound problems. In this study, we describe a technique of percutaneous sacroiliac fusion and present its clinical and radiological outcome. Patients and Methods We reviewed 15 consecutive patients who had undergone a sacroiliac fusion at our hospital for a chronic non-traumatic condition between July 2004 and August 2007. These who had additional pelvic pathology or required further surgery were excluded from the study, as were others operated on for injuries of the sacroiliac joint. We recorded the patient’s demographics, diagnosis and post-operative complications. There were 11 women and four men, with a mean age of 48.7 years (37.3 to 62.6). Each patient had a sacroiliac fusion by a percutaneous technique using hollow modular anchorage screws (Aescalup Ltd, Tuttlingen, Germany) packed with a bone substitute. Diagnosis. The diagnosis of sacroiliac joint disease was based on the clinical presentation, radiological investigations and diagnostic injections. The aetiology in these patients is shown in Table I. Clinical evaluation consisted of Patrick’s test,8 Gaenslen’s test,9 and tenderness over the posterior sacroiliac joint. A full clinical and neurological examination, including sacroiliac joint injections, was performed to exclude any other cause of low back pain. Plain radiographs focused on the sacroiliac joint were used to identify signs of arthritis or sclerosis. Further radiological examination included a CT scan of the sacroiliac joint and an MR scan of both the lumbosacral spine and the sacroiliac joint to demarcate the joint pathology in detail. An MR scan is a more 627 628 A. KHURANA, A. R. GUHA, K. MOHANTY, S. AHUJA Table I. Aetiology Diagnosis Number Osteoarthritis Sacroiliac joint Dysfunction Instability Inflammatory arthritis 7 4 3 1 accurate method of identifying coexisting neurological pathology or compression in the lumbosacral spine, whereas a CT scan will confirm the extent of arthritis of the sacroiliac joint. Confirmatory diagnostic injections into the sacroiliac joint were performed by a consultant radiologist under fluoroscopic guidance with the patient lying prone and with a caudal tilt of approximately 20° of the C-arm. Non-ionic contrast was used to confirm that the needle was in the joint and local anaesthetic and corticosteroid were introduced. Surgery was offered to patients only when the clinical symptoms and signs were confirmed by the radiological findings, the injection relieved the patient’s pain, and no other pathological process could be identified. Of the 15 patients, six had undergone spinal surgery previously. Each patient had low back pain or pain in the buttock as their principal symptom. Unilateral fusion was carried out in 11 cases and bilateral procedures in four. Surgical technique. Adequate bowel preparation is of paramount importance to ensure a clear fluoroscopic view of the sacrum and screws. Patients are given a liquid diet for 24 hours pre-operatively and laxatives on the night before surgery. Patients are positioned supine on a radiolucent operating table and a lateral view is taken to identify the starting point for the guide wire. An incision of approximately 1.5 cm is used and a guide wire is introduced into the centre of the triangular portion of the sacroiliac joint, just under the iliac overhang. Inlet and outlet views are used to advance the guide wire. The inlet view is used to guide the wire in the anteroposterior (AP) plane (Fig. 1) and the outlet view gives a true AP view of the sacrum. The aim is to place the guide wire between the superior and inferior end-plates of the first sacral vertebra (Fig. 2). Once the guide wire is in a satisfactory position, a 10 mm hollow modular anchorage screw is inserted over it. The cannulated screw is packed with a bone substitute (DBX, Demineralised Bone Matrix, Synthes Inc, West Chester, Pennsylvania). Post-operatively, patients were mobilised partially weight-bearing for six weeks, after which they gradually increased the weight taken until they were fully weight-bearing at 12 weeks. Outcome measures. The outcome was assessed independently by two authors (AK and ARG). Pre- and postoperative functional evaluation was performed using the short form (SF)-36 questionnaire10 and Majeed’s scoring system.11 The SF-36 is a reliable, validated scoring system which gives a measure of quality of life. Majeed’s scoring system was originally developed to assess functional outcome after pelvic injuries. It is based on five criteria: pain, standing, sitting, sexual function and performance at work. Each patient had AP, inlet and outlet views of the pelvis taken at three and six months post-operatively, and at final follow-up. These are not a very accurate method of confirming fusion, but we took the absence of clinical symptoms and signs and the absence of any radiological signs of metal failure or lucency to indicate fusion of the sacroiliac joint. Further radiological evaluation was performed only if patients reported continuing symptoms. In these cases we obtained a CT scan to determine whether or not fusion had occurred, and an MR scan to identify any alternative source of pain. Two patients reported continuing symptoms after 12 months’ follow-up and underwent CT and MR scanning. Statistics. Wilcoxon’s signed-ranks test was used as a nonparametric alternative to the t-test to compare the pre- and post-operative results. Statistical calculations were performed using SPSS software version 14 (SPSS Inc., Chicago, Illinois). A p-value < 0.05 was considered significant. Results The mean follow-up was for 17 months (9 to 39). The mean SF-36 scores improved from 37 (23 to 51) to 80 (67 to 92) for physical function and from 53 (34 to 73) to 86 (70 to 98) for general health (Table II). These differences were statistically significant (p = 0.037). The mean Majeed score improved from 37 (18 to 54) pre-operatively to 79 (62 to 96) post-operatively (p = 0.014). Based on Majeed’s score, 13 patients had good or excellent results. The remaining two improved from 21 and 33 to 57 and 64, respectively. Their SF-36 scores improved from a mean of 29 (23 to 35) to 48 (44 to 52). Intra-operative blood loss was minimal (< 50 ml) in all cases. No patient required autologous bone grafting. There were no post-operative neurological or wound complications. There were no obvious problems with screw placement, such as breach of the anterior cortex or the nerve root foramen. There were no cases of implant failure. The mean post-operative hospital stay was 2.7 days (1 to 7). Fusion was obtained in all patients and none required further surgery. In the two patients with a fair result, fusion was confirmed with a CT scan. Discussion The sacroiliac joint may be the source of pain in a significant number of patients with low back pain1,2 and may be a source of persistent pain after lumbar fusion.2 It allows approximately 2° to 4° of movement in the sagittal plane. As it is a synovial joint, it can develop degenerative changes.5,12 Sacroiliac dysfunction is a term used to describe pain from the joint with no demonstrable lesion, but with a presumed underlying biomechanical disorder.13,14 It is diagnosed by Patrick’s8 and Gaenslen’s9 THE JOURNAL OF BONE AND JOINT SURGERY PERCUTANEOUS FUSION OF THE SACROILIAC JOINT WITH HOLLOW MODULAR ANCHORAGE SCREWS Fig. 1a 629 Fig. 1b Diagrams of the inlet view showing a) placement of the guide wire and b) the screw in the coronal plane. Fig. 2a Fig. 2b Diagrams of the outlet view showing, a) placement of the guide wire and b) the screw in the transverse plane between the superior endplate of the first sacral vertebra and the sacral foramina. tests, in the absence of any other obvious pathology.13,14 Post-partum sacroiliac instability15 and inflammatory arthritis,6 crystal arthropathy and infection12 are other known causes. Our study group had a preponderance of patients with sacroliliac arthritis or dysfunction (Table I). Non-operative treatment for sacroiliac pain includes physiotherapy, radiofrequency neurotomy and intraarticular injections.1,4 The efficacy of these measures has not been proven.1 Operative intervention has been described in the form of sacroiliac joint debridement3 or fusion.5,7,16 A thorough clinical assessment and accurate diagnosis and good patient selection are of paramount importance if surgery is to succeed. An accurate diagnosis can be difficult to make, as patients may present with a variety of symptoms and there is no single reliable diagnostic test.5 However, injection of corticosteroid and local anaesthetic under image intensifier control may assist in making the diagnosis.2,5 VOL. 91-B, No. 5, MAY 2009 Haufe and Mork3 reported that 53% of their patients improved by more than 75% two years after having had a sacroiliac joint debridement without instrumentation. Buchowski et al5 evaluated the functional and radiological outcome in 20 patients after an open sacroiliac fusion using the Smith-Petersen approach. They reported improvement in both pain and function. However, the mean blood loss in their series was 290 ml (SD 186) and the mean duration of post-operative stay was 5.2 days (SD 3.8). In their series, two patients developed a deep infection and three a nonunion requiring further surgery. The incidence of significant complications after open sacroiliac fusion has been reported to be between 6% and 25%.5,16 The percutaneous technique avoids wound-related complications and achieved union in all cases in this series. A similar percutaneous procedure has been reported for patients with disruption of the posterior pelvic ring and those with sacral insufficiency fractures.17-19 Percutaneous fixation in these 630 A. KHURANA, A. R. GUHA, K. MOHANTY, S. AHUJA Fig. 3 Fig. 4 Post-operative inlet view showing placement of the screws in the coronal plane. Post-operative outlet view showing placement of the screws in the anteroposterior plane. Table II. Mean pre- and post-operative short form (SF)-36 scores SF-36 component Pre-operative (SD) Post-operative (SD) p-value Physical functioning Role physical Bodily pain General health Vitality Social functioning Role emotional Mental health Physical summary Mental summary 37.15 27.20 21.26 53.67 39.92 44.37 59.64 57.68 28.49 46.82 79.33 36.27 46.87 85.77 58.26 54.84 66.46 68.19 51.38 57.48 0.026 0.045 0.031 0.018 0.027 0.041 > 0.05 > 0.05 0.033 0.045 (14.28) (10.70) (16.71) (19.44) (10.51) (11.28) (14.74) (17.26) (11.24) (17.88) patients provides early stabilisation with minimal operative time, minimal blood loss, and little wound-related morbidity. We have not, however, been able to find any report of percutaneous sacroiliac joint fusion for non-traumatic sacroiliac joint pathology in the literature. In this study 13patients (87%) had good or excellent results. The remaining two showed some improvement in their Majeed and SF-36 scores. Follow-up CT scans in both these patients showed that fusion of the sacroiliac joint had been obtained. Their MR scans suggested an arthropathy of the lower lumbar facet joints as well, which may explain the persistent pain. This was also present in their preoperative scans. They were offered sacroiliac fusion because of tenderness and arthropathy and a satisfactory response to the diagnostic injections. Post-operatively, these patients reported remission of localised sacroiliac symptoms. It does, however, highlight the need for accurate diagnosis with confirmation by diagnostic injections. Patients with possible alternative sources of pain should be warned of the risk of failure. Xu et al20 and Tonetti et al21 concluded in separate studies that pelvic CT should be carried out pre-operatively to (12.52) (11.65) (7.91) (13.82) (13.16) (12.27) (13.80) (19.42) (9.87) (17.32) demonstrate the precise anatomy of the patient. This enhances the safety of iliosacral screw placement. The inlet view (Fig. 3) shows the orientation of screws relative to the coronal plane and will show any screw tip perforating the ala anteriorly, and the outlet view (Fig. 4) will show those extending into the sacral foramina or superior to the ala.20 We conclude that the insertion of percutaneous hollow modular anchorage screws fused with demineralised bone matrix is a satisfactory method of achieving sacroiliac stabilisation in the appropriate patient. The authors would like to thank J. Sharp, Senior Medical Artist, Medical Illustrations Department, University Hospital of Wales, Cardiff, for creating the line diagrams. No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article. References 1. Hansen HC, McKenzie-Brown AM, Cohen SP, et al. Sacroiliac joint interventions: a systematic review. Pain Physician 2007;10:165-84. 2. Katz V, Schofferman J, Reynolds J. The sacroiliac joint: a potential cause of pain after lumbar fusion to the sacrum. J Spinal Disord Tech 2003;16:96-9. 3. Haufe SM, Mork AR. Sacroiliac joint debridement: a novel technique for the treatment of sacroiliac joint pain. Photomed Laser Surg 2005;23:596-8. THE JOURNAL OF BONE AND JOINT SURGERY PERCUTANEOUS FUSION OF THE SACROILIAC JOINT WITH HOLLOW MODULAR ANCHORAGE SCREWS 4. Vallejo R, Benyamin RM, Kramer J, Stanton G, Joseph NJ. Pulsed radiofrequency denervation for the treatment of sacroiliac joint syndrome. Pain Med 2006;7:429-34. 5. Buchowski JM, Kebaish KM, Sinkov V, et al. Functional and radiographic outcome of sacroiliac arthrodesis for the disorders of the sacroiliac joint. Spine J 2005;5:520-8. 6. Berthelot JM, Gouin F, Glemarec J, Maugars Y, Prost A. Possible use of arthrodesis for intractable sacroiliitis in spondylarthropathy: report of two cases. Spine 2001;26:2297-9. 7. Belanger TA, Dall BE. Sacroiliac arthrodesis using a posterior midline fascial splitting approach and pedicle screw instrumentation: a new technique. J Spinal Disord 2001;14:118-24. 8. Barenstein DG, Weisel SW, Boden SD. Low back and neck pain. In: Comprehensive diagnosis and management. Third edition. Philadelphia: Saunders;2004:128. 9. Gaenslen FJ. Sacro-iliac arthrodesis: indications, author’s technic and end-results. JAMA 1927;89:2031-5. 10. Ware JE Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). 1. conceptual framework and item selection. Med Care 1992;30:473-83. 11. Majeed SA. Grading the outcome of pelvic fractures. J Bone Joint Surg [Br] 1989;71B:304-6. 12. Bernard TN Jr, Cassidy JD. The sacroiliac joint syndrome: pathophysiology, diagnosis, and management. In: The adult spine: princioples and practice. New York: Raven Press, 1991:2107-30. VOL. 91-B, No. 5, MAY 2009 631 13. Dreyfuss P, Michaelsen M, Pauza K, McLarty J, Bogduk N. The value of medical history and physical examination in diagnosing sacroiliac joint pain. Spine 1996;21:2594-602. 14. Elgafy H, Semaan HB, Ebraheim NA, Coombs RJ. Computed tomography findings in patients with sacroiliac pain. Clin Orthop 2001;382:112-18. 15. Lynch FW. The pelvic articulations during pregnancy, labor, and the puerperium: an xray study. Surg Gynecol Obstet 1920;30:575-80. 16. Schütz U, Grob D. Poor outcome following bilateral sacroiliac joint fusion for degenerative sacroiliac joint syndrome. Acta Orthop Belg 2006;72:296-308. 17. Shuler TE, Boone DC, Gruen GS, Peitzman AB. Percutaneous iliosacral screw fixation: early treatment for unstable posterior pelvic ring disruptions. J Trauma 1995;38:453-8. 18. Nork SE, Jones CB, Harding SP, Mirza SK, Routt ML Jr. Percutaneous stabilization of U-shaped sacral fractures using iliosacral screws: technique and early results. J Orthop Trauma 2001;15:238-46. 19. Tsiridis E, Upadhyay N, Gamie Z, Giannoudis P. Percutaneous screw fixation for sacral insufficiency fractures: a review of three cases. J Bone Joint Surg [Br] 2007;89B:1650-3. 20. Xu R, Ebraheim NA, Robke J, Yeasting RA. Radiologic evaluation of iliosacral screw placement. Spine 1996;21:582-8. 21. Tonetti J, Cloppet O, Clerc M, et al. Implantation of iliosacral screws: simulation of optimal placement by 3-dimensional x-ray computed tomography. Rev Chir Orthop Reparatrice Appar Mot 2000;86:360-9 in French).