Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
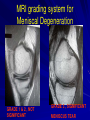
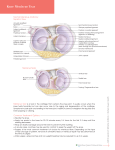
MRI KNEE WHAT TO SEE Dr. SHEKHAR SRIVASTAV Sr.Consultant – KNEE & SHOULDER ARTHROSCOPY MRI KNEE - WHAT TO SEE MRI is the most accurate and frequently used diagnostic tool for evaluation of internal derangement of knee. MRI examination of knee consists of spin echo sequences obtained in sagittal, coronal and usually axial plane. Sagittal cuts most important SAGITTAL CUTS Cruciates Meniscus Cartilage Extensor mechanism CORONAL CUTS Collaterals Meniscus Cartilage AXIAL CUTS PATELLO-FEMORAL PROBLEMS MRI Knee Meniscus ACL PCL Collateral ligaments Patello femoral Chondral defects Misc. Meniscus Normal anatomy The normal meniscus shows uniform, low signal intensity (Black) Peripherally the meniscus have a bow- tie configuration Centrally, the normal meniscus is composed of 2 separate triangular structures, the anterior horn and the posterior horn. The apices (free edges or inner margins) appear as sharp points of the triangle facing each other. MRI grading system for Meniscal Degeneration GRADE 1 & 2 , NOT SIGNIFICANT GRADE 3 , SIGNIFICANT MENISCUS TEAR Types of Meniscal Tear Three basic meniscal tear Longitudinal Radial Horizontal Longitudinal Tears Longitudinal tears separate the meniscus into inner and outer fragments and occur parallel to the outer margin of the meniscus are perpendicular to the tibial plateau and propagate parallel to the circumferential axis of the meniscus Radial tears ( Transverse Tears) These are vertical tear and propagate perpendicular to the main axis of the meniscus Horizontal tear These tears are also called cleavage or fish- mouth tears They divide the meniscal tear into a top ( superior) portion and a bottom ( inferior) portion Most are degenerative, occurring in older patients with osteoarthritis. Bucket- Handle Tears These tears are displaced vertical longitudinal tears and usually involve the MM . The separated central ( inner) fragment, when viewed axially, resembles the handle of a bucket The remaining larger peripheral portion of the meniscus resembles the bucket. Typical locations of the displaced fragment include the intercondylar notch anterior and parallel to the PCL ( double PCL sign) MRI criteria for meniscal tears Two MRI criteria established for meniscal tears. have been diagnosing Criteria 1 Criteria 1 is increased internal signal intensity in the meniscus The abnormal signal intensity must be in contact with one articular surface, either the superior or interior surface or at the tip ( free edge) of the meniscus Criteria 2 Criterion 2 is an abnormal meniscal shape ACL The normal ACL appears on sagittal images as a solid band or as a striated band diverging slightly, ruler straight although mild sagging convex inferiorly can be present, especially with mild knee flexion. The ACL shows low- to intermediate signal intensity , higher than that of the PCL. ACL Tear – Primary Signs – Secondary Signs Primary signs of the ACL tear Disruption, increased signal intensity in the substance of the ACL on T2 weighted images, abrupt angulation or wavy appearance and abnormal ACL axis. Nonvisualization or near nonvisualization with replacement be a cloud of focal edema and hemorrahage. Secondary Signs of ACL Tear Pivot - shift bone bruises and osteochondral fracture Anterior translocation of the tibia Segond fracture Anterior tibial spine fractures Buckling of PCL Secondary Signs of ACL Tear Pivot- Shift Bone Bruises Anterior Translocation of the Tibia and Fractures Secondary Signs of ACL Tear Avulsion fracture of the tibia at ACL insertion Buckling PCL Segond Fracture PCL Major stabilizer of knee Restrain against post. displacement Isolated –3% Combined –97% – – – – ACL injury - 65% MCL – 50% Medial Meniscus – 30% Posterior capsule and fibular collateral ligament MRI Finding Intrasubstantial tear Partial tear Complete tear Avulsions Collateral Ligaments Coronal images with anatomy defining and fluid-sensitive sequences demonstrate the medial and lateral supporting structures optimally. Additional useful information can be gleaned from sagittal and axial images of these structures Chondral Defects Degenerative cartilage defects Osteochondritis dissecans Chondromalacia patellae Osteochondritis Dissecans Chondromalacia Patellae Miscellaneous Meniscal cysts Ganglion cyst Discoid meniscus Infections PVNS Extensor mechanism tear – Quadriceps tendon tear – Patellar tendon tear – Tibial tuberosity avulsion Meniscal Cysts Ganglion Cysts Discoid Meniscus INFECTION Tubercular Hypointense Synovial proliferation Marrow Edema Osteomyelitis Abcess Cortical erosion Sinuses PVNS Low signal changes Synovial proliferation Hemosiderin deposition Extensor Mechanism Tear Quadriceps Tendon Tear Patellar Tendon Tear Tibial Tuberosity Avulsion MRI – Very useful tool in hands of Radiologists & Orthopedicians Orthopedicians probably in a better position than Radiolologist to read MRI Visit www.delhiarthroscopy.com Thank You MCL Tear Grade I Microscopic tear Grade II Partial tear Grade III Complete tear LCL LCL tear is seen as a serpiginous or lax ligament with discontinuous fibers (or avulsed fibular head), often without significant thickening of the ligament. LCL tears rarely are isolated, and an LCL tear becomes more likely as associated PLC and cruciate ligament injuries increase in severity Studies reported in diagnostic arthroscopy 51% (With use of MRI) MRI accuracy in Meniscus & ACL Pathology > 90% Difference in radiologist & arthroscopist opinion in meniscal injury because Different radiologist are at different level of the learning curve and different arthroscopist have different level of experience Partial ACL Tear Partial tears of the ACL are common, accounting for 10-43% of all ACL tears Direct signs may include focal angulation of the ACL or partial – thickness focal high signal intensity. T2- weighted images allow more confident identification of abnormal focal high signal intensity in the ACL substance ( stoller, 1997). MRI grading system for Meniscal Degeneration Grade I Grade I is a nonarticular , focal or diffuse region of increased signal intensity within the substance of the meniscus . Grade 2 Grade 2 is a horizontal , linear area of increased signal intensity within the substance of the meniscus that extends to but does not involve the articular surface. . Patients are usually asymptomatic Meniscal Degeneration Grade 3 Is a region of abnormal signal intensity within the meniscus extending to and communicating with at least 1 articular surface of the meniscus Clinically Significant