Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
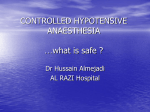
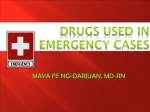
PAROXYSMAL SYMPATHETIC WITHDRAWAL/Williams and Bashore 901 22. Caldwell PD, Ricketts HJ, Dillard DH, Guntheroth WG: Ventricular tachycardia in a child: an indication for angiography? Am Heart J 88: 777, 1974 23. Engle MA, Ebert PA, Redo SF: Recurrent ventricular tachycardia due to resectable cardiac tumor. Circulation 50: 1052, 1974 tachycardia and ventricular fibrillation in a young population. Circulation 60: 988, 1979 21. Ferrer PL: Arrhythmias in the neonate. In Cardiac Arrhythmias in the Neonate, Infant and Child, edited by Roberts, NI, Gelband H. New York, Appleton-CenturyCrofts, 1977, p 291 Paroxysmal Hypotension Associated with Sympathetic Withdrawal A New Disorder of Autonomic Vasomotor Regulation R. SANDERS WILLIAMS, M.D., AND THOMAS M. BASHORE, M.D. Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 SUMMARY We evaluated a patient who had transient episodes of hypotension with clinical and laboratory features apparently distinct from previously recognized disorders of vasomotor regulation. In between his abrupt attacks of hypotension, the patient is asymptomatic and demonstrates normal autonomic modulation of heart rate and blood pressure in response to changes in body position, Valsalva maneuver, cold, and exercise. During periods of hypotension, his plasma norepinephrine falls markedly and he has blunted or absent responses to stimuli that normally have a pressor effect due to sympathetic efferent discharge. Mechanical or known hormonal disorders that produce episodic hypotension have been excluded by extensive testing. We suggest two possible causes for our patient's paroxysmal sympathetic withdrawal: first, a centrally mediated inhibition of sympathetic discharge to peripheral resistance and capacitance vessels, but with no afferent stimulus reflexly producing sympathetic withdrawal readily evident; or second, an episodic release of an unknown endogenous compound with inhibitory effects upon central or preganglionic sympathetic neurons or upon postganglionic sympathetic neurons by a presynaptic inhibition of norepinephrine release. HYPOTENSION associated with abnormal autonomic modulation of vasomotor function is a prominent feature of several neurologic disorders-117 (table lA). Other disorders may also lead to paroxysmal hypotension by one of three major mechanisms: episodic or variable vascular obstruction,18 22 abnormal activation of vasodepressor reflexes,23 26 or abnormal episodic release of endogenous vasoactive substances27-32 (table 1B). We recently evaluated a patient with paroxysmal hypotension in whom extensive laboratory investigation revealed features that appear to be distinct from any recognized disorders of vasomotor regulation. Case Report A 50-year-old Caucasian man was referred to our Cardiovascular Laboratory for the evaluation of frequent episodes of presyncope associated with hypotension. His spells of lightheadedness occurred one to three times daily and lasted 1 minute to 4 hours. He From the Division of Cardiology, Duke University Medical Center, and the Veterans Administration Medical Center, Durham, North Carolina. Address for correspondence: R. Sanders Williams, M.D., P.O. Box 3945, Duke University Medical Center, Durham, North Carolina 27710. Received November 21, 1979; revision accepted March 5, 1980. Circulation 62, No. 4, 1980. had to remain supine to avoid syncope. The onset of the spells was not related to body position. There were no premonitory symptoms, no apparent periodicity, and no evident precipitating events (such as exertion, meals or emotional stress) associated with the episodes. He occasionally had bitemporal headaches during or after a period of hypotension, but had no other associated symptoms. He had no flushing of the skin. In between the episodes he was asymptomatic, with no orthostatic lightheadedness or abnormalities of sweating or micturition. He first noted similar spells in 1971, though from that time until late 1978 they had been less frequent (one or two per month) and were shorter (5-60 minutes) than the more recent spells. Previous therapeutic trials of ephedrine, atropine and fludrocortisone acetate had been ineffective in preventing or moderating his symptoms. His medical history included numerous episodes of superficial and deep thrombophlebitis of the lower extremities, dating from a deep-vein thrombosis during hospitalization for an appendiceal abscess at age 12 years, and including several vein-stripping procedures. In 1971 he suffered an angiographically documented pulmonary embolus despite systemic anticoagulation, and underwent percutaneous insertion of an umbrella filter device33 into his inferior vena cava. He also had a history of abuse of alcohol and minor tranquilizers and reported several hospital admissions for psy- CIRCULATION 902 Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 TABLE 1. Disorders of Vasomotor Control Leading to Hypotension A. Neurologic disorders associated with autoiiomic dysfunction Peripheral neuropathies: diabetes mellitus;2 alcoholism;3 acute intermittenit porphyria; 4 tabes dorsalis5 Wernicke's disease6 Parkinson's disease7 Holmes-Adie syndrome8 Familial dysautonomia (Riley-Day)9 Lesch-Nyan syndrome'0 Guillain-Barre syndrome"1 Shy-D)rager syndrome12 aiid idiopathic orthostatic hypotensionl3 Acute pandysautonomia14 Autonomic epilepsy1" Old age"6 Postprandial glucose loading17 Numerous drugs with hypotensive effects B. Disorders producing episodic hypotension (excluding cardiac dysrhythmias) IJtermittent vascular obstruction Atrial myxomals Defective cardiac valve prosthesisl9 Pregnancy or large iiitra-abdomiiial tumor2' Aortic stenosis21 Idiopathic hypertrophic subaortic steniosis (IHSS)22 Abnormal activation of autoniomic reflexes Centrally mediated vasodepressor syncope23 Hypersensitive carotid sinus syndrome24 Micturition syncope2' Cough syncope26 ? Aortic stenosis2l and ? IHSS22 Abnormal release of vasoactive substances Pheochromocytoma (epinephrine, dopamine, other amines)27 Carcinoid syndrome (serotonin)28 Systemic mastocytosis (histamine)29 Anaphylactic shock (histamine, kiniins, SR1S-A);° Septicemic shock (endotoxins)31 Hereditary angioedema (complement activation)12 chiatric evaluation and care. Although he denied alcohol or drug abuse in the 3 months before admission, he did note prominent symptoms of depression. He also gave a history of hypertension that had intermittently been treated with diuretics. On physical examination he weighed 235 lbs and was 5'10" tall. His supine vital signs were pulse rate 72 beats/min and blood pressure 150/90 mm Hg, changing normally with standing to a pulse rate of 76 beats/min and blood pressure of 142/90 mm Hg. During a typical hypotensive spell (fig. 1) his blood pressure fell precipitously, to a range of 50/30 mm Hg to 80/50 mm Hg, usually with no change in heart rate or a slowing to a range of 48-68 beats/min. His periods of hypotension during hemodynamic monitoring ranged from 3 minutes to 21/2 hours. During hypotension he remained oriented and conversant, VOL 62, No 4, OCTOBER 1980 though at times he appeared drowsy; his extremities remained warm; he did not become diaphoretic; his pupils were midposition and his pupillary responses to light were preserved; and his respiratory rate generally increased slightly, although he had no striking hyperventilation. His skin showed stasis hyperpigmentation of the lower extremities. His head, eyes, ears, nose and throat were normal. His jugular venous pulsations were normal, as was his thyroid gland. He had bilateral carotid bruits, which were more prominent on the left. His left ventricular impulse was in the fifth left intercostal space, 12 cm from the midsternal line, and was normal. S, and S, were normal, and an S4 gallop was present. No cardiac murmurs or other abnormal sounds were present. His lungs, abdomen, rectum, and genitalia were normal. The lower extremities showed superficial varicosities and 1 + peripheral edema. The peripheral arterial pulsations were normal. His neurologic examination was within normal limits. Baseline laboratory data included a chest radiograph that was normal except for some calcification in the aortic knob and an ECG that showed nonspecific ST-T-wave changes only. His ECG was unchanged during hypotension. A complete blood count, urinalysis, serum electrolytes, urea nitrogen, blood sugar, and SMA-12 were within normal limits, except for a uric acid of 8.7 mg%. His prothrombin time was 12.3 seconds (control 11.8 seconds). Partial thromboplastin time was 32.3 seconds (control 39.8 seconds). Other laboratory data included erythrocyte sedimentation rate (Westergren) 38 mm/hour fluorescent antinuclear antibody titer 1:160 with weakly speckled pattern, VDRL negative, hepatitisassociated (surface) antigen negative, rheumatoid factor negative, LE prep negative, thyroxine 9.8 mg/100 ml, RT3U 27%. Radioisotope quantification of plasma volume by 1251-albumin was within normal limits. Plasma cortisol was normal. A toxic screen of plasma at the time of admission revealed only trace levels of benzodiazepine metabolites. Urinary excretion per 24 hours of 5HIAA was undetectable, and of VMA was normal at 3.4 mg. Computerized axial tomography of the abdomen was normal. Laboratory Evaluation of Hypotensive Episodes The hemodynamic characteristics of our patient's hypotensive episodes were studied in the cardiac catheterization laboratory and by continuous hemodynamic monitoring on the coronary care unit. Recordings of intra-arterial blood pressure during normotension and during typical hypotensive episodes are shown in figure 1. Hemodynamic measurements obtained in the catheterization laboratory before and during a hypotensive spell are listed in table 2. The initial pulmonary capillary wedge pressure of 18 mm Hg, observed in the catheterization laboratory, followed the injection of radiographic contrast media; more typical measurements during continuous hemo- PAROXYSMAL SYMPATHETIC WITHDRAWAL/ Williamis and Bashore AE CONTROL 903 DECREASED BP Spontaneous BP Fall ECG 200r ARTERIAL PRESSURE 100 (mm Hg) N... HR 65 ,W 0t 1 Sec. B 200lDownloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 ARTERIAL PRESSURE (mm Hg) 100 0- 1 Min. Frc RF. 1. Intra-arterial pressure recordings during hypotenivive epis odes. (A ) Hrpoten.is ive episode iin the catheterization laboratory. Tracings are not continuous. (B) Continuous miioni.toring of radial arteriy pressvre. This tracing illustrates the typical abrupt swings in blood pressure. front normotension at left to profound hripotension,followed bir a rapid return to normotension again. BP blood pressuare; IR - heart rate. dynamic monitoring on the coronary care unit during normotension ranged from 8-14 mm Hg, and during hypotension ranged from 5-8 mm Hg. Injections of contrast media into the right atrium revealed no evidence of right atrial myxoma, and no left atrial filling defects were noted during levophase. An echocardiogram was normal. Because we suspected intermittent venous obstruction of the inferior vena cava at the level of his umbrella device, pressure measurements above and below the umbrella TA\BLE 2. Heniodlynamstl ic illeasurcuents Bcforc andIl)ring Hypotensive Spell Ilxoteinsion Noinotenlsionilly Arterial pressure (mrin Jig) 158 /4 78/46 a hleart rate (bhets/naini) Arterioveniouis oxygeni differenlce (vol (() 58 158 5.4 6.6 5.8 2.5 100 4.0 t.7 Cardiac outpult, (Fick) (/rnilln) Cardiac inidex (1/ralilln lln2) Stroke volume (nil) Systemiic resistance (Wood ullits) Mean pulm-nonatry capillary wedge pressuire (mm lig) 16.4 18 69 11.5 8 made and contrast injections were performed during normotension and during hypotension. There was no pressure gradient, and dye flowed freely across the umbrella during hypotension. We tested our patient's responses to a number of stimuli known to activate intrinsic autonomic responses in normal subjects.1 Unlike his normal circulatory responses to changes in body position while normotensive, during a hypotensive episode his blood pressure fell still further with changes from the supine to sitting position, evoking symptoms of presyncope, and he failed to elevate his heart rate with sitting. Valsalva maneuvers during normotension elicited the expected fall in arterial pressure and tachycardia during the late strain phase, followed by the normal "overshoot" of blood pressure with slowing of the heart rate upon release (fig. 2A). During hypotension, these responses were markedly blunted (fig. 2B). The adequacy of the Valsalva maneuver in each instance was documented by a rise in intrathoracic pressure of at least 40 mm Hg for at least 10 seconds as recorded by a central venous catheter. Similarly, placing his hand in ice water during normotension evoked the were normal pressor response (fig. 3A), while little effect was noted during a hypotensive episode (fig. 3B). Massage of either the left or right carotid sinus produced bradycardia during normotension, but did not produce hypotension; during hypotension, it produced slight sinus slowing or had no effect. (IOTBER 1980 Voi- 62, No 4, CIlRCULATION 904 A E 1- E VALSALVA ) LL D B. U,) Lli W 100 r Lr LU cj-: Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 lOL ----- c --- VALSALVA >1 4 Sec. FIU REi 2. Intra-arterial pressure recordings during Valsuala maneuvers. (A J Valsalva m?anelul er dlurinig normotension. A`Wte the prominent -overshoot of arterial pressure after the release of intrathoraci . (B) Valsalva maneuver during hvpotension. Note the absetnce ofthe -overshoot- phenomenon. pressure Plasma catecholanmines were measured by radioenzymatic assay34 on blood obtained from an indwelling venous needle left in place at least 15 minutes before sampling. On 2 days, after blood samples were obtained while the patient was supine and his blood pressure was greater than 120/80 mm Hg, a hypotensive episode began. Repeat blood sampling was done 5-15 minutes after the onset of a fall in arterial pressure to levels less than 80/50 mm Hg. Each time hypotension was associated with a fall in plasma A. 200 .. , 5S 5~~ C) ~C EC S~~ WATER IMMERSION -------------- POST - T- E FE B. LUJ D 1i LU HR 55 a- HR 45 HR 52 100k-1 4i 1 SEC 0- PRE ICE WATER IMMERSION POST [Iwt,'Ri, 3. Intra-arterial pressure recordings during immersion of the right hanid inz ice water. (A) Ice water immersion during normotens ion. Note the rapid and sustained rise in arterial pressu4re. fllob wed hi a retuirni to baseline after the cold stimiiulus was withdrawn. (Two nminutes elapse at the break ini the tracing. o (B) Ice water immersi.on during hipotension. Note the absence of a significatt pressor effect. HR heart = rate. PAROXYSMAL SYMPATHETIC WITHDRAWAL/ Williams and Bashore 300D E 0 -c ,-z' lep(*.05 200.11 - 0 c .a .1 0 ,' .11 BP Syst 120 100 (mm Hg) Diast 1.1 ,,1l~ C1 , 0 z 0 E 1.' , , c HR (bpm) 0^ 100l 905 80 60 40 20)l 80 60 40 ICE OFF zu- ^L---i U -- 40 80 120 160 Systolic Blood Pressure (Supine) (mm Hg) Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 FIGURE 4. Plasma norepinephrine levels plotted against the systolic blood pressure at the time of blood sampling. Values during normotension are expressed as open squares and values during hypotension as open circles. The dotted lines connect determinations that were made serially within 1 hour of each other. The mean plasma norepinephrine during normotension (closed square) differed significantly from the mean value during hypotension (closed circle) at the p < 0.05 level by one-way analysis of variance. Vertical lines represent the SEM. norepinephrine to roughly one-half the resting value (fig. 4). An electroencephalogram with nasopharyngeal leads was within normal limits during normotension and was unchanged during a hypotensive episode. Forearm venous plethysmography was monitored by standard techniques35 before and during a hypotensive episode, with results roughly paralleling the central hemodynamics during cardiac catheterization. Hypotension was associated with an abrupt fall in forearm vascular resistance (fig. 5). When this occurred, ice placed on the forehead, perhaps a more potent sympathetic stimulus than placing the hand in ice water, was associated with a slight, although blunted, pressor response. During normotension, a bicycle ergometer exercise test was unassociated with abnormalities in his ECG, and his heart rate and blood pressure responses to exercise were normal. His ventricular function as assessed by gated blood pool radionuclide angiography was normal both at rest and with bicycle exercise. Response to Cardiac Pacing, Pharmacologic Agents and Biofeedback Right atrial or right ventricular pacing (fig. 6) during a hypotensive episode did not correct the hypotensive state. Two types of drug studies were performed: acute i.v. or intranasal drug administration during a hypotensive episode aimed at correcting the hypotension and oral drug administration over a 72-hour 0 3 6 9 12 15 18 21 24 27 33 36 39 TIME (mins) FIGURE 5. Heart rate (HR), bloodpressure (BP), forearm blood flow (FBF) and forearm vascular resistance (FVR) before and during a hypotensive episode. Note the rapid decline in forearm vascular resistance occurring simultaneously with the fall in systemic arterial pressure. The application of ice to the forehead (arrow) produced a rise in vascular resistance and a slight increase in arterial pressure, though without returning arterial pressure to the normal range. period aimed at the prevention or modification of the hypotensive spells. Because of the marked spontaneous variation in the duration of his hypotensive spells, all acute interventions were performed several times. Neither i.v. atropine (2 mg), propranolol (5 mg), or isoproterenol (4 ,g/min) produced a pressor response during hypotensive episodes (fig. 6B and 6C), although a cardioacceleratory effect of both atropine and isoproterenol did occur. With i.v. phenylephrine at an infusion rate of 75 ,ug/min, blood pressure returned to or above the normal range each of the three times it was tested (fig. 6D). A dose-response effect was observed for phenylephrine in that lower doses evoked smaller pressor effects. The doses of i.v. phenylephrine necessary to produce a pressor response were similar to those required for pressor effects in normal subjects.`e Thus, we did not observe the hypersensitivity to infused catecholamines that may be present in patients with idiopathic orthostatic hypotension.37 Intranasal phenylephrine (1%) solution in doses CIRCULATION 906 B= EGG E E PRE~ATROPINE Lii U) U) Li Er Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 Ir Li FIGURE 6. Effects of cardiac pacing and drugs upon blood during hypotension. ECG monitoring and radial artery pressure (RA P) during hypotension before and during right ventricular pacing (A), before and 5-10 minutes after 2 mg of i. v. atropine (B), before and during i. v. infusion of 4 g/mmin ofisoproterenol (C), and before and during i. v. infusion of 75 ,g/min of phenylephrine (D). The correction of hypotension by phenylephrine was confirmed twice during pressure separate hypotensive episodes. as high as 5 mg was ineffective in correcting the hypotension. We attempted to prevent or modify our patient's hypotensive episodes with a variety of pharmacologic agents, with each drug administered orally in the stated dosages for at least 72 hours. Neither carbamazepine 200 mg for 1 day, 400 mg for 1 day, then 600 mg every day for 3 days, indomethacin 25 mg three times daily, ephedrine 25 mg four times daily, the combination of diphenhydramine 50 mg three times daily plus cimetidine 300 mg four times daily, nor transylcypromine (monoamine oxidase inhibitor) VOL 62, No 4, OCTOBER 1980 10 mg twice daily, induced any observable change in the frequency, severity or duration of the hypotensive episodes. Biofeedback techniques and hypnosis were used to find clues to possible centrally mediated factors leading to his hypotensive episodes. Although a hypotensive spell occurred once during hypnosis, it could not be reversed during or in the hour after hypnosis, and voluntary induction or reversal of hypotension could not be reproducibly accomplished on other occasions. The patient denied any voluntary control over the episodes or any insight into psychological trigger mechanisms. Surreptitious drug administration was excluded by intra-arterial pressure recordings documenting numerous typical hypotensive episodes during sleep, during direct observation of the patient in the catheterization laboratory, and during direct visual monitoring of the patient by closed-circuit television in the coronary care unit. Discussion Our patient's hypotensive episodes appear to be different from previously reported disorders causing hypotension. During periods of normotension, he demonstrated normal autonomic vasomotor and cardiac chronotropic responses to standing, Valsalva maneuver, cold and exercise. His periods of hypotension were associated with signs of dramatic withdrawal of peripheral sympathetic efferent tone in both resistance and capacitance vessels. During hypotension his total peripheral vascular resistance and forearm vascular resistance fell markedly, his pulmonary capillary wedge pressure fell, he demonstrated blunted or absent responses to maneuvers that normally activate sympathetic neural reflexes, and he had an inappropriate bradycardia and an inappropriate absence of cutaneous signs, such as pallor or sweating, given the profound level of hypotension present. In addition, his plasma norepinephrine fell markedly with the onset of hypotension, and the hypotension could be readily corrected by i.v. phenylephrine, presumably through its effect upon postsynaptic vascular aadrenergic receptors, but not by cholinergic antagonists, ,3-adrenergic agonists or antagonists, cardiac pacing, prostaglandin synthesis inhibitors, histamine antagonists, monoamine oxidase inhibitors, or antiepileptic medication. We considered several possible causes for our patient's hypotensive spells. Anatomic loss of sympathetic neurons, inflammatory neuritis, or metabolic abnormalities, such as diabetes mellitus leading to autonomic insufficiency, were excluded by the highly transient nature of the hypotensive episodes, the absence of other neurologic dysfunction, and the absence of discernible metabolic abnormalities. In addition, he had no other clinical evidence for the neurologic disorders listed in table IA that have been associated with hypotension. Centrencephalic epilepsy causing stimulation of pathways inhibitory to the peripheral release of norepinephrine was probably ex- PAROXYSMAL SYMPATHETIC WITHDRAWAL/ Williams and Bashore Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 cluded by the normal electroencephalogram during hypotension and the lack of a therapeutic response to carbamazepine. Intermittent vascular obstruction at the site of his inferior vena cava umbrella filter was excluded by angiographic studies. There was no evidence for right or left atrial myxoma, valvular heart disease, or hypertrophic subaortic stenosis. In addition, intermittent vascular obstruction alone could not explain the failure of the expected signs of reflex sympathetic stimulation to appear with the onset of hypotension. Abnormal release of vasoactive substances producing vasodilatation and episodic hypotension has been observed in the situations cited in table 1 B, but plasma or urine analyses, the failure of antagonist drug trials, or the lack of other expected concomitant clinical features excluded these known disorders. The clinical and laboratory data suggesting episodic withdrawal of peripheral sympathetic tone in association with our patient's hypotensive spells are strong. However, the stimuli leading to sympathetic withdrawal were not identifiable, unlike the common form of vasodepressor syncope or the hypotensive syndromes of hypersensitive carotid sinus, micturition syncope, or cough syncope. Also, the duration of his hypotensive periods was often much longer than that observed in these syndromes. There was no evidence of a relationship between our patient's episodic hypotension and the other clinical abnormalities we observed - the history of psychiatric disturbances, the history of venous thromboembolic disease, the carotid bruits, the elevated uric acid, and the moderate antinuclear antibody titer. We propose that one of two hypothetical mechanisms leads to the apparent withdrawal of sympathetic tone that accompanies the episodic hypotension noted in our patient. First, the withdrawal of peripheral sympathetic vasomotor tone may be mediated centrally by reduced firing of afferent neurons from the medullary vasomotor centers. The primary stimulus that produces this centrally mediated sympathetic withdrawal could be from higher central nervous system pathways impinging upon the vasomotor centers of the brainstem, or from the activation of the afferent limb of an undescribed vasodepressor reflex, perhaps a sympathetically mediated analogy of the vagally mediated Bezold-Jarish reflex38 in laboratory animals. The opportunity to test this hypothesis must await either identification of a stimulus that produces hypotension in our patient or a method that allows us to record the rate of afferent sympathetic neuronal firing in our patient. Second, an apparent sympathetic withdrawal could be produced by the episodic release of some unknown endogenous compound, perhaps a tumor product, with inhibitory effects either upon activation of central, pre- or postganglionic sympathetic neurons, or upon the release of norepinephrine from postganglionic nerve terminals, perhaps by stimulation of inhibitory presynaptic a-adrenergic receptors. 907 Acknowledgment The authors gratefully acknowledge the assistance and advice of Dr. John Baker and Dr. Jeffrey Medoff in the clinical evaluation of the patient; Dr. Redford Williams for the forearm venous plethysmography analysis and biofeedback efforts; Dr. Steven Grossman, Dr. J. Caulie Gunnells and Robin Sykes for the plasma catecholamine assays; and especially Dr. Joseph Greenfield and Dr. Eugene Stead for their advice during the laboratory evaluation of this patient and their review of the manuscript. We also thank Linda Ashley and Janice James for their assistance in the preparation of the manuscript. References 1. Johnson RH, Spalding JMK: Disorders of the Autonomic Nervous System. Philadelphia, FA Davis, 1974 2. Cryer PE, Siterberg AB, Santiago JV, Shah SD: Plasma catecholamines in diabetes: the syndromes of hypoadrenergic and hyperadrenergic postural hypotension. Am J Med 64: 407, 1978 3. Novak DJ, Victor M: The vagus and sympathetic nerves in alcoholic polyneuropathy. Arch Neurol 30: 273, 1974 4. Schirger A, Martin WJ, Goldstein NP, Huizenga KA: Orthostatic hypotension in association with acute exacerbations of porphyria. Mayo Clin Proc 37: 7, 1962 5. Sharpey-Schafer EP: Circulatory reflexes in chronic disease of the afferent nervous system. J Physiol 134: 1, 1956 6. Birchfield RI: Postural hypotension in Wernicke's disease: a manifestation of autonomic nervous system involvement. Am J Med 36: 404, 1964 7. Bannister R, Oppenheimer DR: Degenerative diseases of the nervous system associated with autonomic failure. Brain 95: 457, 1972 8. Johnson RH, McLellan DL, Love DR: Orthostatic hypotension and the Holmes-Adie syndrome: a study of two patients with afferent baroreceptor block. J Neurol Neurosurg Psychiat 34: 562, 1971 9. Riley CM, Moore RH: Familial dysautonomia differentiated from related disorders. Pediatrics 37: 435, 1966 10. Rockson S, Stone R, VanderWeyden M, Kelley WN: Lesch- 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. Nyhan syndrome: evidence for abnormal adrenergic function. Science 186: 934, 1974 Matsuyama H, Haymaker W: Distribution of lesions in the Landry-Guillain-Barre syndrome, with emphasis on involvement of the sympathetic system. Acta Neuropath 8: 230, 1967 Shy GM, Drager GA: A neurologic syndrome associated with orthostatic hypotension. Arch Neurol 2: 511, 1960 Ziegler MG, Lake CR, Kopin IJ: The sympathetic-nervous system defect in primary orthostatic hypotension. N Engl J Med 296: 293, 1977 Hopkins A, Neville B, Bannister R: Autonomic neuropathy of acute onset. Lancet 1: 769, 1974 Penfield W, Erickson TC: Epilepsy and Cerebral Localization. Springfield, Charles C Thomas, 1941 Johnson RH, Smith AC, Spalding JMK, Wollner L: Effect of posture on blood-pressure in elderly patients. Lancet 1: 731, 1965 Appenzeller 0, Goss JE: Glucose and baroreceptor function: effects of oral administration of glucose on baroreceptor function in cerebrovascular disease and in other disorders with baroreceptor reflex block. Arch Neurol 23: 137, 1970 Peters MN, Hall RJ, Cooley DA, Leachman RD, Garcia E: The clinical syndrome of atrial myxoma. JAMA 230: 695, 1974 Kloster FE: Diagnosis and management of complications of prosthetic heart valves. Am J Cardiol 35: 872, 1975 Courtney L: Supine hypotension syndrome during Caesarean section. Br Med J 1: 797, 1970 Johnson AM: Aortic stenosis, sudden death, and the left ventricular baroreceptors. Br Heart J 33: 1, 1971 Braunwald E, Morrow AG, Cornell WP, Aygen MM, Hilbish TF: Idiopathic hypertrophic subaortic stenosis: clinical, hemodynamic and angiographic manifestations. Am J Med 29: 924, 1960 CIRCULATION 908 23. Engel GL: Psychologic stress, vasodepressor (vasovagal) syncope, and sudden death. Ann Intern Med 89: 403, 1978 24. Walter PF, Crawley IS, Dorney ER: Carotid sinus hypersensitivity and syncope. Am J Cardiol 42: 396, 1978 25. Lyle CB, Monroe JT, Flinn DE, Lamb LE: Micturition syncope: report of 24 cases. N Engl J Med 265: 982, 1961 26. Sharpey-Schafer EP: The mechanism of syncope after coughing. Br Med J 2: 860, 1953 27. Gifford RW, Kvale WF, Maher FT, Roth GM, Priestley JT: Clinical features, diagnosis, and treatment of pheochromocytoma: a review of 76 cases. Mayo Clin Proc 39: 281, 1964 28. Kahil ME, Brown H, Fred HL: The carcinoid crises. Arch Intern Med 114: 26, 1964 29. Parker C, Garza R: Systemic mastocytosis. Am J Med 61: 671, 1976 30. Austen KF: Systemic anaphylaxis in the human being. N Engl J Med 291: 661, 1974 31. Robinson JA, Klodnycky ML, Loeb HS, Racic MR, Gunnar RM: Endotoxin, prekallikrein, complement and systemic vascular resistance: sequential measurements in man. Am J Med 59: 61, 1975 VOL 62, No 4, OCTOBER 1980 32. Frank MM, Gelfand JA, Atkinson JP: Hereditary angioedema: the clinical syndrome and its management. Ann Intern Med 84: 580, 1976 33. Mobin-Uddin K, Callard GM, Bolooki H, Rubinson R, Michie D, Jude JR: Transvenous caval interruption with umbrella filter. N Engi J Med 286: 55, 1972 34. Peuler JD, Johnson GA: Simultaneous single isotope radioenzymatic assay of plasma norepinephrine, epinephrine, and dopamine. Life Sci 21: 625, 1977 35. Greenfield ADM: Venous occlusion plethysmography. Methods Med Res 8: 293, 1960 36. Theilen EO, Wilson WR: Hemodynamic effects of peripheral vasoconstriction in normal and thyrotoxic subjects. J Appl Physiol 22: 207, 1967 37. Davies BD, Bannister R, Sever P: Pressor amines and monoamineoxidase inhibitors for treatment of postural hypotension in autonomic failure: limitations and hazards. Lancet 1: 172, 1978 38. Dawes GS, Mott JC, Widdicombe JG: Respiratory and cardiovascular reflexes from the heart and lungs. J Physiol 115: 258, 1951 Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 Paroxysmal hypotension associated with sympathetic withdrawal. A new disorder of autonomic vasomotor regulation. R S Williams and T M Bashore Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 Circulation. 1980;62:901-908 doi: 10.1161/01.CIR.62.4.901 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1980 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/62/4/901 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/