Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
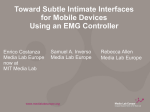
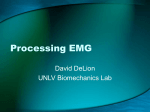
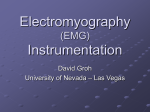
©1999 ARTVILLE, LLC Estimation and Application of EMG Amplitude During Dynamic Contractions Processing Nonstationary EMG for Applications in Prosthesis Control, Biofeedback, and Joint Torque Estimation Wthey conduct electrical activity (ac- hen skeletal muscle fibers contract, Edward A. Clancy1, Stéphane Bouchard2, Denis Rancourt2 1 Department of Electrical and Computer Engineering and Department of Biomedical Engineering, Worcester Polytechnic Institute 2 Department of Mechanical Engineering, Laval University November/December 2001 tion potentials, APs) that can be measured by electrodes affixed to the surface of the skin above the muscle. As the APs pass by the electrodes, spikes of electrical activity are observed and pulses of muscle fiber contractions are produced. Small functional groups of muscle fibers, termed motor units (MUs), contract synchronously, resulting in a motor unit action potential (MUAP). To sustain force, an MU is repeatedly activated by the central nervous system several times per second. The repetition, or average, firing rate is often between 5 and 30 times per second (or faster) [1]. During most voluntary muscle contraction, however, a sufficiently large number of MUs contract (generally asynchronously) and a random electrical interference pattern is observed by surface electrodes. In the absence of muscle fatigue (a condition that will not be discussed in this report), increased firing rate and/or increases in the number of active MUs result in both increased muscle tension and an interference pattern with higher power. Studied as a whole (i.e., without decomposing the individual action potentialsa separate and important study topic) the overall magnitude of the electrical activity found at the skin surface provides insight into muscle effort. The magnitude of the electrical activity is commonly referred to as the amplitude of the electromyogram (EMG). This amplitude has been used, for example, as the control input to upper-limb prostheses (myoelectrically controlled elbows [19], wrists, and hands), in biofeedback applications, in ergonomic assessment, and to estimate the torque produced about a joint [2, 9, 15, 23]. IEEE ENGINEERING IN MEDICINE AND BIOLOGY Although an MU is activated repeatedly, the interval between successive activations is not fixed. Rather, the physiology “fires” an MU at nonperiodic time intervals (with some average firing rate). The interval lengths can be well modeled as a random process with a mean value equal to the average time between firings. In addition, the number and identity of MUs active at any time is controlled. Thus, stochastic process models have been used to model the recorded EMG. Some of these models superimpose the random firing of individual MUs to form a composite recorded EMG (e.g., [1, 25]). Alternatively, “functional” models are based on the observed interference signal without specific regard to the underlying physiologic processes of individual MU firings. In this case, the observed interference pattern is modeled directly as a Gaussian (e.g., [10, 17, 18]) or Laplacian [10] random process. The functional modeling style will be developed exclusively herein. Further, because the strength of muscle contraction is varied in many of these applications, EMG amplitude is generally a time-varying parameter. As will be discussed below, timevarying EMG amplitudes cause the stochastic models to be nonstationary. If the EMG signal is modeled mathematically as a random process, then EMG amplitude can more formally be defined as the time-varying standard deviation of the random process. Then, optimal estimation techniques can be used to best estimate EMG amplitude from a sample of the EMG. This style of formal EMG modeling has led to progressive iterative improvement in EMG amplitude estimates over the past 25 or more years, with a concomitant increase in the number of signal details in0739-5175/01/$10.00©2001IEEE 47 There are at least two fundamental difficulties in relating surface EMG amplitude directly to the tension produced by individual muscles. cluded in the random process model. The majority of this article will describe the present “state of the art” in EMG modeling and amplitude estimation. Emphasis will be placed on the impact of the nonstationary nature of the signal on the details of the estimation technique. Estimates of EMG amplitude can be used directly in such applications as the control input to upper-limb prostheses, biofeedback, and ergonomic assessment. Once a dynamic EMG amplitude estimate is available, a common application is to relate the EMG amplitude to the dynamic mechanical activity of the muscle. It would be ideal to relate surface EMG amplitude directly to the tension produced by wi Htime(ejω) individual muscles. However, there are at least two fundamental difficulties in doing so. First, classical EMG recorded at the surface of the skin can contain “cross talk.” That is, EMG from muscles other than that which the experimenter intends to record may be included in the signal. Cross talk is a difficult problem with no immediate, simple solution. Second, relating EMG to individual muscle tension requires independent verification via direct mechanical measurement of individual muscle tension. At present, there is no practical (and perhaps not any) method for reliably making such measurements in situ. Because of these fundamental limitations, several efforts have focused on relating surface EMG amplitude to joint torque. First, cross talk, if it exists, may not be as problematic. Certain cross-talk contributions are automatically removed from the estimated torque, even if they cannot be removed from the individual muscle tension contributions (c.f., [3, pp. 343-345]). Second, net torque about a joint can, in many cases, be reasonably (or even easily) verified via direct mechanical measurement. The second portion of this article will present preliminary results of a recent study of relating EMG amplitude to joint torque during force-varying contractions. Model of the Surface EMG Functional models of the EMG seek to capture the observed stochastic behavior of the EMG signal without including the complexity that would be involved in modeling the activity of each individual MU. A complete model in this style for a single channel of EMG is shown in Fig. 1. ri ni si Zero Mean, WSS, Shaping Filter CE, White Process of Unit Intensity Σ mi vi EMG Amplitude Zero Mean, WSS, CE, Additive Noise Process Measured Surface EMG 1. Mathematical model of a single channel of the surface EMG. A zero-mean, wide-sense stationary (WSS), correlation-ergodic (CE), white process of unit intensity wi (i is the sample index) passes through the stable, causal, inversely stable, linear, time-invariant shaping filter H ( e jω ). It is then multiplied by the EMG amplitude s i and added to the zero-mean, WSS, CE, Gaussian noise process v i to form the measured surface EMG m i . The processes wi and v i are assumed to be uncorrelated with each other and the EMG amplitude. Muscle contraction is nonfatiguing. 48 IEEE ENGINEERING IN MEDICINE AND BIOLOGY This model produces a measured surface EMG (m i ) with statistical properties similar to real EMG. The model develops surface EMG from a zero-mean, wide-sense stationary (WSS), correlation-ergodic (CE), white process of unit intensity. The white process is passed through a time-invariant shaping filter, which accounts for the spectral shaping in the measured EMG. The output of the shaping filter is multiplied by the time-varying EMG amplitude (s i ). All changes in the signal variance of the noise-free EMG (ri ) are attributed to changes in the EMG amplitude. Because EMG is invariably observed in the presence of measurement noise, an additive Gaussian noise source (v i ) is included in the model. This noise source is much broader-band than the noise-free EMG (represented by ri ). The white process (wi) is frequently assumed to be Gaussian distributed, although other distribution assumptions are possible [10]. As can be seen by this mathematical model, EMG amplitude is defined as the standard deviation of the EMG (observed in the presence of additive noise). This standard deviation is time varying (hence, the process is nonstationary) because EMG amplitude is a function of time. Note that multiple-channel EMG models also exist for the purpose of estimating EMG amplitude. In these models, it is assumed that several electrodes can be placed over different regions of the same muscle to simultaneously monitor the electrical activity of different muscle fibers. In this case, all electrodes contribute to the one amplitude estimate. EMG Amplitude Estimation During Dynamic Conditions Given the above EMG model, EMG amplitude estimation becomes the problem of estimating the time-varying standard deviation of a colored random process in the presence of additive noise. An optimal closed-form analytic solution for achieving this goal has yet to be derived. (See [4, 11] for a brief historical perspective of research work in this area.) However, piece-wise solutions (i.e., those in which individual processing steps are optimal) exist. The most common of these solutions is shown in block diagram form in Fig. 2. The figure shows the cascade of six sequential processing stages to form a general processor for EMG amplitude estimation. The six stages are 1) noise and interference attenuation/filtering, 2) whitening, 3) mulNovember/December 2001 tiple-channel combination (including gain scaling), 4) demodulation, 5) smoothing, and 6) relinearization. Noise and interference attenuation/filtering is used to reject motion artifacts, power line interference, etc.—common noise sources that have been omitted from the EMG model shown in Fig. 1. Because successive EMG samples are necessarily acquired at or above the Nyquist rate, neighboring EMG samples are correlated. [Physiologically, the correlation between neighboring EMG samples is a consequence of the limited signal bandwidth (modeled by the shaping filter in Fig. 1). The limited signal bandwidth reflects the actual biological generation of EMG and the lowpass filtering effects of the tissues as the signal propagates from its source to the measurement apparatus.] Unfortunately, correlated samples confound optimal statistical estimation problems, such as estimation of a standard deviation (i.e., the EMG amplitude estimation problem). Decorrelation (that is, whitening) makes the samples statistically uncorrelated and increases the “statistical bandwidth.” Thereafter, the detection algorithm treats each sample as independent. Multiple-channel combination is used to combine the information from several electrode recordings made over the same muscle. Demodulation rectifies the whitened EMG and then raises the result to a power [either one for mean-absolute-value (MAV) processing or two for root-mean-square (RMS) processing]. Smoothing filters the signal, increasing the signal-to-noise ratio, albeit at the expense of adding bias error to the estimate. Finally, relinearization inverts the power law applied during the demodulation stage, returning the signal to units of EMG amplitude. Two issues are important to point out when using this processing scheme. First, five of the six steps are relatively independent of each other. (The demodulation and relinearization steps must be inverses of each other, thus they are completely dependent.) Therefore, the processing steps can generally be considered separately. Second, it turns out that dynamics in the EMG only have a significant influence on processing decisions in the smoothing step. This article will review these six processing steps with an emphasis on the smoothing step. Additional details of these steps can be found elsewhere [5-8, 10-11]. November/December 2001 EMG Amplitude Estimation Processing Steps The goal of the first processing stage is to eliminate noise and interference (e.g., motion artifact, power-line interference) that are acquired along with the “true” EMG. Of course, it should be mentioned that the most successful treatment of these unwanted signal sources is to minimize their contribution to the measured signal samples via, for example, proper skin preparation prior to electrode placement and the use of active electrodes. The frequency content of motion artifact is typically below 10-20 Hz. The general approach to motion artifact reduction is to high-pass filter the EMG with a cutoff frequency of approximately 20 Hz. Little “true” signal power is lost, however most motion artifact is rejected. For attenuating power-line interference, the most straightforward technique is to apply a narrow fixed-notch filter to EMG at the power-line fundamental frequency and its first few harmonics. Notch filtering, however, removes “true” signal as well as power-line components. Most remaining techniques fall under the category of adaptive filters, the most well known being that of Widrow et al. [24]. They describe an adaptive interference cancellation method in which a reference input (a signal correlated with the power-line interference) is adaptively filtered and subtracted from the corrupted signal, giving an estimate of the true signal. This method can be applied for interference reduction wherever a ref- The goal of the first processing stage is to eliminate noise and interference (e.g., motion artifact, power-line interference) that are acquired along with the “true” EMG. erence “noise” signal (in this case, the power line) can be obtained simultaneously with the corrupted signal. Additional discussion of motion artifact and power-line interference attenuation can be found in [11]. After attenuation of motion artifact and power-line interference, the signal is treated as though it were free of these arti- m1(t) Noise Reject/ Filter Whiten Detect •d m2(t) Noise Reject/ Filter Whiten Detect •d m3(t) Noise Reject/ Filter Whiten m4(t) Noise Reject/ Filter Whiten .. . Spatial Uncorrelate and Gain Normalize .. . Detect •d Smooth ∧ Relinearize s(t) (•)1/d .. . Detect •d 2. Cascade of processing stages used to form an EMG amplitude estimate. The acquired EMG m1 , i through m L , i are all assumed to be from bipolar electrodes placed over the same muscle. The EMG amplitude estimate is s i . In the “Detect” and “Relinearize” stages, d = 1 for MAV processing and d = 2 for RMS processing. IEEE ENGINEERING IN MEDICINE AND BIOLOGY 49 facts (although an additive background noise remains). Next, in stage two, the signal is whitened, typically via software signal processing algorithms. A whitening filter is formed by first estimating the power spectral density (PSD) of the “true” (i.e., noise-free) EMG and, in one case discussed below, the accompanying additive noise. Then, the inverse of the square root of the “true” PSD is the shape of the whitening filter. At least three general methods to achieve whitening have been described in the literature. First, for constant-force, constant-posture, nonfatiguing contractions, it is common to whiten using a moving average filter (determined by the “true” PSD). (See [7, 16] for details.) Second, contrary to the functional Table 1. Degrees of freedom constant “g” for several different EMG processors. This constant is determined by the statistical bandwidth of the EMG, the number of EMG channels, and the detector type (see [5] for details). EMG Processor Degrees of Freedom Constant “g” (Hz) Detector Whitened vs. Unwhitened Number of EMG Channels Mean-Absolute-Value (MAV) Unwhitened 1 263 Mean-Absolute-Value (MAV) Unwhitened 4 546.5 Mean-Absolute-Value (MAV) Whitened 1 639 Mean-Absolute-Value (MAV) Whitened 4 1427 Root-Mean-Square (RMS) Unwhitened 1 234.5 Root-Mean-Square (RMS) Unwhitened 4 463.5 Root-Mean-Square (RMS) Whitened 1 617.5 800 Optimal Window Length (ms) 700 Noncausal, Quadratic Model 600 500 400 300 200 100 Causal, Linear Model 0 0 0.5 1 1.5 2 2.5 3 EMG Amplitude / [EMG Amplitude Derivative] 3. Theoretical optimal smoothing window lengths. Dotted graph is for noncausal processing. For this plot, the X-axis is the ratio of EMG amplitude to EMG amplitude second derivative magnitude (in units of seconds squared). The solid graph is for causal processing. For this plot, the X-axis is the ratio of EMG amplitude to EMG amplitude first derivative magnitude (in units of seconds). For both graphs, the constant g is set to 500/s. 50 IEEE ENGINEERING IN MEDICINE AND BIOLOGY EMG model given above, some research has assumed that the PSD of the EMG can v a ry (i. e . , th e s h a p in g f i l t e r i s time-varying), and thus the whitening filter must vary as well. In this case, the PSD model is continuously updated, and thus the whitening filter is time adaptive [13-14]. Historically, both of these methods have ignored that fact that EMG is invariably observed in the presence of additive broadband noise, as modeled in Fig. 1. Hence, when EMG amplitude is small relative to the noise (at lower contraction levels), the above techniques may fail. Thus, a third technique was recently developed that adapts the whitening scheme based on the PSD of both the “true” EMG and the additive noise [6]. This technique incorporates a noise attenuation stage that adaptively filters the signal based on the relative strength of the signal versus the noise. EMG is effectively whitened over all contraction levels. Formally, the adaptive noise attenuation is a nonstationary filter. But, because the filter has a short time constant, EMG amplitude is relatively constant over the duration of time during which data are passing through the filter. Hence, the processing is considered stationary for the filter duration, even though the filter shape is continuously updated (quasi-stationary). After the whitening stage, the signal is assumed to be noise-free and temporally uncorrelated. When multiple channels have been recorded from the same muscle, they are next combined in the third processing step. Formally, the spatial correlation between channels must be accounted for when combining channels [7, 17]. However, in practice, simple gain normalizing of the channels (to account for the fact that the signal strength can vary from one recording site to the other) is sufficient (at least for up to four electrodes [7]). Thus, channel combination is accomplished by gain normalizing the multiple signals. The standard deviation of the “true” EMG is now the common standard deviation of these signals. In order to estimate this standard deviation from the EMG samples, some form of nonlinearity must be applied to the signals. In general, the nonlinearity consists of taking the absolute value of each sample, then raising each sample to a power. This operation is the fourth processing stage—demodulation. Whatever power is selected in this stage also specifies the relinearization opNovember/December 2001 eration in the sixth processing stage. The two most common powers are one (MAV processing) and two (RMS processing). Theoretically, Hogan and Mann [17] have shown that RMS processing is optimal if EMG is Gaussian distributed, and Clancy and Hogan [10] have shown that MAV processing is optimal if EMG is Laplacian distributed. Using EMG from biceps and triceps muscles, Clancy and Hogan found that the observed densities fell in between the theoretic Gaussian and Laplacian densities. On average, the Gaussian density was the better fit. For amplitude estimation, MAV processing had a higher SNR than RMS processing, but only by 2.0-6.5%. These results suggest that forming EMG amplitude estimates via either RMS or MAV processing is nearly indistinguishable. The Smoothing Step s2 ⋅ 2Ave (s ) Ave 1/ 5 where N is the window length (samples), 2 is f is the sampling frequency (Hz), s Ave the average value of the square of EMG amplitude, and (s 2 ) Ave is the average value of the square of the second derivative of EMG amplitude. The quantities November/December 2001 2 s Ave ⋅ 1/ 3 2 g ( s ) Ave 1 1/ 3 where ( s 2 ) Ave is the average value of the square of the first derivative of EMG amplitude. Figure 3 shows an example plot used to select the optimal window length. Note that several studies have attempted to improve the amplitude estimate by dynamically adapting the window length to the local characteristics of the EMG (e.g., [5, 12, 21]). In direct comparison to the best fixed-length smoother, these adaptive smoothers have found little or no advantage for generic applications, with a few exceptions. The six steps described above produce a state-of-the-art estimate of EMG amplitude. Note that in all of the above, selection of the window length was discussed in view of optimizing the amplitude estimate only. For applications such as EMG-torque estimation (discussed below), the amplitude estimate is the input to an ensuing procedure (e.g., EMG amplitude to torque modeling). In these cases, smoothing may be skipped en- mE1,i mE2,i mE L Extensor EMG Amplitude Estimator ∧ sE E,i tirely (leaving all of the smoothing to the ensuing application), or the smoothing parameters may be dictated by the requirements of the application. Preliminary Results of Relating EMG Amplitude to Joint Torque During Dynamic Conditions As mentioned above, a common application of EMG amplitude is to estimate torque about a joint. Preliminary results of a first investigation to do so with advanced EMG amplitude estimators and dynamic contractions will now be described. To adequately estimate joint torque, both agonist and antagonist muscles must be monitored [9]. If multiple-channel EMG recordings are made from both the agonist and antagonist muscle groups, then EMG-torque estimation can be organized as shown in Fig. 4. In the figure, all flexion torque is attributed to one “composite” agonist muscle, and all extension torque is attributed to one “composite” antagonist muscle. Although individual muscle group tensions (TE and TF ) are internal states of the model, only the net joint torque contributes to model error. Note that more general model representations exist; e.g., the more generic two-input ( s F , s E ), one-output (TExt ) system is also common. For this investigation, linear models of the EMG amplitude to torque relationship were studied during constant-posture contraction about the elbow. Linear models would likely capture much of the system dynamics (c.f. the EMG-torque investigations of Gottlieb and Agarwal [15] and Extensor EMG Amplitude to Torque Estimator TE − TExt Σ mF1,i mF2,i mFL … 72 N Noncausal = f g 1/ 5 N Causal = f … What remains to be described is the fifth processing step—smoothing. Initially, the demodulated samples from each sample index are averaged across L channels. A single demodulated signal results. Then, several demodulated samples are averaged in time to form one amplitude estimate. A sliding time window selects the demodulated samples for each successive amplitude estimate, thereby forming an averaging filter. Because EMG amplitude is changing during contraction, an appropriate smoothing window length over which the signal is quasi-stationary must be selected [5, 12, 20-21]. In doing so, it is found that variance (random) errors in the EMG amplitude estimate are diminished with a long smoothing window; however, bias (deterministic) errors in tracking the signal of interest are diminished with a short smoothing window. Clancy [5, see Appendix] derived a method for optimal selection of a fixed window length. Different results were derived for causal and noncausal (midpoint moving average) processing. For noncausal processing, the optimal window length was found to be: 2 and (s 2 ) Ave take different values for s Ave different tasks. The constant g is related to the number of statistical degrees of freedom in the data, determined by the statistical bandwidth of the EMG, the number of EMG channels, and the detector type (see [5] for details). Table 1 shows the value of g det e rm in e d e x p e r im e n ta lly b y St-Amant et al. [22] for eight different processors. For causal processing, the optimal window length was found to be: Flexor EMG Amplitude Estimator F,i ∧ sF Flexor EMG Amplitude to Torque Estimator TF + 4. Net torque about the joint (TExt ) equals the flexor muscles torque contribution (TF ) minus the extensor muscles torque contribution (TE ). The flexor muscles torque contribution is a function of the flexor EMG amplitude (s F ), which is estimated from the flexion electrode EMG samples (m F1 , i through m FL , i , where L F is F the number of flexion channels). The extensor muscles torque contribution is similarly estimated. IEEE ENGINEERING IN MEDICINE AND BIOLOGY 51 Thelen et al. [23]). Appropriate nonlinear models can be incorporated in the future, as necessary. Methods The EMG and torque data used in this study are a portion of the data obtained during an experiment examining constant-posture exertions about the elbow, described in detail in [6]. Briefly, subjects (16) were firmly seated in the chair of an exercise machine (Biodex Medical Systems, Shirley, NY, U.S.A.) and their right wrist rigidly secured to the chair arm. They were asked to exert dynamically varying elbow torque (motion bandwidth of 1 Hz) indicated by a visual feedback signal shown to them on a computer screen, for periods of 30 s at a maximum of 50% of their maximum voluntary contraction (MVC). The contraction patterns were random in nature, requiring equal durations of flexion and extension contraction on average. Eight EMG surface electrodes (Liberty Technology model MYO115, Hopkinton, MA, U.S.A.) were placed on the subject’s right arm (four over the biceps and four over the triceps muscles) for acquisition of two four-channel EMG signal sets. The location of the four biceps electrodes is depicted in Fig. 5. EMG-torque processing was performed offline, with a portion of the acquired data from each subject serving as a training set for the model, and the remaining data serving as the test set. Only test set results are reported. To investigate the influence of advanced EMG algorithms—in particular, multiplechannel processing and the adaptive whitening technique of [6]—four different EMG processors were used (each processor was used to produce a flexion and an extension EMG amplitude estimate for each trial). Processor 1 was the single-channel technique, without whitening. Processor 2 was the four-channel technique, without whitening. Processor 3 was the single-channel technique, with whitening. Processor 4 was the four-channel technique, with whitening. The smoothing stage was effectively omitted from amplitude estimate processing since the optimal smoothing for torque estimation is inherently solved for in the system-identification process. Two different system-identification models were examined. Model 1 was an output error (OE) model that incorporated the operating point (mean values of the inputs and the outputs) into the identification process. This model estimated the complete joint torque. Model 2 was an OE model that operated on the data after all mean values were removed (“AC model”). This model only estimated the dynamic portion of joint torque. In all, a total of eight processor-model combinations were reported. For each combination, a range of model orders was also investigated. Results were expressed as the percent variance accounted for (%VAF), a time-domain error measure equal to 100 ⋅ PError , %VAF = 100 − PTrue where PError is the total power in the torque estimate error and PTrue is the total power in the true torque. Additional details of the system identification are available in [2]. EMG 3 Subject 21, File 69, %VAF = 89.5 EMG 2 EMG 1 Anterior EMG 0 Torque (Percent of Maximum Contraction) 100 50 0 −50 −100 5. Drawing showing the location of the four biceps electrode-amplifiers on the right arm of a subject. The two contacts of each electrode-amplifier were oriented along the muscle’s long axis, the presumed direction of action potential conduction. Each electrode-amplifier had a pair of 4-mm-diameter, stainless steel, hemispherical contacts separated by 15 mm (center to center). The distance between adjacent electrode-amplifiers was approximately 1.75 cm (center to center). 52 0 5 10 15 20 25 30 Time (Seconds) 6. The measured torque (solid line) and the corresponding EMG-torque estimate (dotted line) are plotted versus time into the trial. EMG were processed using the four-channel technique, with whitening. The EMG-torque modeling technique was the OE model that incorporated the operating point into the identification process. The model numerator order was five and denominator order was six. A positive-valued torque denotes extension, a negative-valued torque denotes flexion. IEEE ENGINEERING IN MEDICINE AND BIOLOGY November/December 2001 Experimental Results and Discussion Only preliminary results are presently available, with accompanying statistical analysis yet to be completed. Figure 6 is a time-series plot representative of the results for the four-channel, whitened EMG amplitude estimation technique using the OE modeling method that incorporated the operating point into the identification process. The model numerator order was five and the denominator order was six. Table 2 lists summary results from the eight processor-model combinations. The %VAF listed is that corresponding to the maximum average value of all the model orders tested. This model order is also listed in each cell. Average torque estimation performance using whitened EMG processors was better than unwhitened processors, and using four-channel processors it was better than single-channel processors. These results are consistent with results from a previous experiment using nondynamic contractions [9]. In addition, the combination of whitening and multiple channels provided the best performance. This result is expected since both whitening and multiple-channel EMG amplitude estimation reduce the noise variance of EMG amplitude. Their combination provides a cumulative benefit [8]. Hence, the input to the system identification process has less noise. The “AC Model” was investigated since it is common in system identification studies to separately model the ac and dc characteristics of a system. Doing so removes the influence of the system’s operating point (the dc component of the signals) on the system’s dynamics (the ac components of the signal). Of course, after estimating the ac response, a complete response is found by combining the estimated ac and dc responses. Only the ac portion of the response was studied here. For OE processing, the ac models all had a higher average %VAF than the full model. Since the dc component can more accurately be modeled with a nonlinear model [9], it may be worthwhile in the future to consider nonlinear dynamical system models. One such system would be to combine a dc model (e.g., [9]) with the ac models reported above. Many other options are available. Table 2 also lists the number of nonconvergent trials for each of the reported %VAFs. There were a total of 80 trials available per cell (16 subjects times five November/December 2001 training set trials per subject). For these trials, the system identification algorithms were unable to find a global minimum solution for the model parameters. In these cases, no test result is reported for that trial-processor-model combination. As can be seen from the table, nonconvergence was less of a problem with the ac model. There are several issues related to nonconvergence that warrant further investigation in this EMG-torque application, including: selecting a contraction bandwidth that sufficiently excites the system to be identified, appropriate model order selection, appropriate selection of an initial solution in the OE model, duration of the training contraction, and the extent of co-contraction exhibited by the subjects. Summary The sections above have described an EMG amplitude estimator and an initial application of this estimator to the EMG-torque problem. The amplitude estimator consists of six stages. In the first stage, motion artifact and power-line interference are attenuated. Motion artifact is typically removed with a highpass filter. Elimination of power-line noise is more difficult. Commercial systems tend to use notch filters, accepting the concomitant loss of “true” signal power in exchange for simplicity and robustness. Adaptive methods may be preferable, however, to preserve more “true” signal power. In stage two, the signal is whitened. One fixed whitening technique and two adaptive whitening methods were described. For low-amplitude levels, the adaptive whitening technique that includes adaptive noise cancellation may be necessary. In stage three, multiple EMG channels (all overlying the same muscle) are combined. For most applications, simple gain normalization is all that is required. Stage four rectifies the signal and then applies the power law required to demodulate the signal. In stage six, the inverse of the power law is applied to relinearize the signal. Direct comparison of MAV (first power) to RMS (second power) processing demonstrates little difference between the two. Therefore, unless there is reason to believe that the EMG density departs strongly from that found in the existing studies, RMS and MAV processing are essentially identical. In stage five, the demodulated samples are averaged across all channels and then smoothed (time averaged) to reduce the variance of the amplitude estimate, but at the expense of increasing the bias. For best performance, the window length that best trades off variance and bias error is selected. The advanced EMG processing was next applied to dynamic EMG-torque estimation about the elbow joint. Results showed that improved EMG amplitude estimates led to improved EMG-torque estimates. An initial comparison of different system-identification techniques and model orders was reported. It is expected that these advanced processing and identification algorithms will also improve performance in other EMG applications, including myoelectrically controlled prostheses, biofeedback, and ergonomic assessment. Table 2. EMG-torque estimation results for the 1-Hz bandwidth trials for the four EMG processors and the two modeling techniques, in %VAF. Each result cell lists 1) %VAF: the mean ± standard deviation percent variance accounted for (%VAF), 2) the model order, and 3) nonconvergent trials: the number of contraction trials (out of 80 total) omitted from the %VAF result because the training model did not converge. Symbol nb is the numerator model order and symbol nf is the denominator model order. Model EMG Processor Single Channel Multiple Channel Single Channel Whitened Multiple Channel Whitened OE %VAF n b / nf Nonconvergent Trials 75.7 ± 20.2 6/4 20 82.0 ± 14.2 4/4 16 81.7 ± 12.7 5/3 19 85.4 ± 11.1 5/6 20 OE (AC Model) %VAF n b / nf Nonconvergent Trials 81.5 ± 15.6 ½ 6 84.8 ± 13.6 2/2 8 84.7 ± 13.4 4/2 7 87.2 ± 12.4 6/2 6 IEEE ENGINEERING IN MEDICINE AND BIOLOGY 53 Edward (Ted) A. Clancy received the B.S. degree from Worcester Polytechnic Institute (WPI) and the S.M. and Ph.D. degrees from the Massachusetts Institute of Technology, all in electrical engineering. He spent 12 years in industry as an engineer and research scientist for medical instrumentation and analysis companies interested in EMG, EEG, ECG, blood pressure, and ergonomics, and as a radar engineer at Raytheon Company. He is an associate professor in the Department of Electrical and Computer Engineering and the Department of Biomedical Engineering at WPI. He is interested in signal processing, stochastic estimation, and system identification, particularly as applied to problems in medical engineering and human rehabilitation. (www.wpi.edu/~ted, www.ece.wpi.edu/Research/csp2) Stéphane Bouchard received the B.Sc. degree in mechanical engineering in 1998 from Laval University, PQ, Canada. He received the M.Sc.A. in mechanical engineering (with a concentration in bioengineering) at the same university in 2001. His thesis subject was the dynamic relationship between biceps-triceps EMG and the torque produced during constant-angle contraction of the elbow. His principal interests include system identification, control, signal processing, modeling, real-time programming, and data acquisition. Currently, he is working in the aerospace industry for MDS Aero Support Corp., ON, Canada. Denis Rancourt received the B.Sc degree in mechanical engineering in 1986 from Laval University, PQ, Canada. He received the M.Sc.A. in mechanical engineering at École Polytechnique de Montréal in 1989, and the Ph.D. degree in mechanical engineering at the Massachusetts Institute of Technology in 1995. He holds an associate professor appointment in mechanical engineering at 54 Laval University and is director of the bioengineering laboratory in the same department. He is currently on sabbatical leave at the Euros R&D department, a French orthopaedic designer and manufacturer. His interests cover tissue engineering, human factors, design, modeling, and control of physical systems, with an emphasis on the musculo-skeletal system and orthopaedic implants. (www.gmc.ulaval.ca/labos/bioing/) Address for Correspondence: Edward (Ted) A. Clancy, Department of Electrical and Computer Engineering, Worcester Polytechnic Institute, 100 Institute Road, Worcester, MA 01609. Tel: +1 508 831 5778. Fax: +1 508 831 5491. E-mail: [email protected]. References [1] J.V. Basmajian and C.J. DeLuca, Muscles Al i v e : T he i r F unc t i ons R e v e al e d by Electromyography. Baltimore, MD: Williams & Wilkins, 1985. [2] S. Bouchard, “Relation dynamique entre les signaux électromyographiques et le couple au coude lors de contractions à angles constants,” M.S. thesis, Dept. Mech. Eng., Laval Univ, Québec, Canada, 2001. [3] E.A. Clancy, “Stochastic modeling of the relationship between the surface electromyogram and muscle torque,” Ph.D. dissertation, Dept. Elect. Eng. Comp. Sci., MIT, Cambridge, MA, Jan. 11, 1991. [4] E.A. Clancy, “EMG amplitude estimation: A review of the past and a look towards the future,” in Proc. 1997 MyoElectric Controls Conf., Fredericton, NB, Canada, 1997, pp. 71-74. [5] E.A. Clancy, “Electromyogram amplitude estimation with adaptive smoothing window length,” IEEE Trans. Biomed. Eng., vol. 46, pp. 717-729, 1999. [6] E.A. Clancy and K.A. Farry, “Adaptive whitening of the electromyogram to improve amplitude estimation,” IEEE Trans. Biomed. Eng., vol. 47, pp. 709-719, 2000. [7] E.A. Clancy and N. Hogan, “Single site electromyograph amplitude estimation,” IEEE Trans. Biomed. Eng., vol. 41, pp. 159-167, 1994. [8] E.A. Clancy and N. Hogan, “Multiple site electromyograph amplitude estimation,” IEEE Trans. Biomed. Eng., vol. 42, pp. 203-211, 1995. [9] E.A. Clancy and N. Hogan, “Relating agonist-antagonist electromyograms to joint torque during isometric, quasi-isotonic, non-fatiguing contractions,” IEEE Trans. Biomed. Eng., vol. 44, pp. 1024-1028, 1997. [10] E.A. Clancy and N. Hogan, “Probability density of the surface electromyogram and its relation to amplitude detectors,” IEEE Trans. Biomed. Eng., vol. 46, pp. 730-739, 1999. [11] E.A. Clancy, E.L. Morin, and R. Merletti, “Sampling, noise-reduction and amplitude esti- IEEE ENGINEERING IN MEDICINE AND BIOLOGY mation issues in surface electromyography,” J. Electromyo. Kinesol., to be published. [12] T. D’Alessio, “Analysis of a digital EMG signal processor in dynamic conditions,” IEEE Trans. Biomed. Eng., vol. 32, pp. 78-82, 1985. [13] T. D’Alessio, N. Accornero, and A. Berardelli, “Toward a real time adaptive processor for surface EMG signals,” Ann. Int. Conf. IEEE Eng. Med. Biol. Soc., vol. 9, pp. 323-324, 1987. [14] T. D’Alessio, M. Laurenti, and B. Turco, “On some algorithms for the tracking of spectral structure in non-stationary EMG signals,” in Proc. MIE ‘87, Rome, Italy, 1987. [15] G.L. Gottlieb and G.C. Agarwal, “Dynamic relationship between isometric muscle tension and the electromyogram in man,” J. Appl. Physiol., vol. 30, pp. 345-351, 1971. [16] M.I.A. Harba and P.A. Lynn, “Optimizing the acquisition and processing of surface electromyographic signals,” J. Biomed. Eng., vol. 3, pp. 100-106, 1981. [17] N. Hogan and R.W. Mann, “Myoelectric signal processing: Optimal estimation applied to electromyography—Part I: Derivation of the optimal myoprocessor,” IEEE Trans. Biomed. Eng., vol. 27, pp. 382-395, 1980. [18] N. Hogan and R.W. Mann, “Myoelectric signal processing: Optimal estimation applied to electromyography—Part II: Experimental demonstration of optimal myoprocessor performance,” IEEE Trans. Biomed. Eng., vol. 27, pp. 396-410, 1980. [19] S. Jacobsen, D.F. Knutti, R.T. Johnson, and H.H. Sears, “Development of the Utah artificial arm,” IEEE Trans. Biomed. Eng., vol. 29, pp. 249-269, 1982. [20] H. Miyano, T. Masuda, and T. Sadoyama, “A note on the time constant in low-pass filtering of rectified surface EMG,” IEEE Trans. Biomed. Eng., vol. 27, pp. 274-278, 1980. [21] E. Park and S.G. Meek, “Adaptive filter of the electromyographic signal for prosthetic control and force estimation,” IEEE Trans. Biomed. Eng., vol. 42, pp. 1048-1052, 1995. [22] Y. St-Amant, D. Rancourt, and E.A. Clancy, “Influence of smoothing window length on electromyogram amplitude estimates,” IEEE Trans. Biomed. Eng., vol. 45, pp. 795-799, 1998. [23] D.G. Thelen, A.B. Schultz, S.D. Fassois, and J.A. Ashton-Miller, “Identification of dynamic myoelectric signal-to-force models during isometric lumbar muscle contractions,” J. Biomech., vol. 27, pp. 907-919, 1994. [24] B. Widrow, J.R. Glover, J.M. McCool, J. Kaunitz, C.S. Williams, R.H. Hearn, J.R. Zeidler, E. Dong, and R.C. Goodlin, “Adaptive noise cancelling: Principles and applications,” Proc. IEEE, vol. 63, pp. 1692-1716, 1975. [25] Y.T. Zhang, P.A. Parker, and R.N. Scott, “Study of the effects of motor unit recruitment and firing statistics on the signal-to-noise ratio of a myoelectric control channel,” Med. Biol. Eng. Comput., vol. 28, pp. 225-231, 1990. November/December 2001