Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Sexual dysfunction wikipedia , lookup
Sexological testing wikipedia , lookup
Sexual stimulation wikipedia , lookup
Ego-dystonic sexual orientation wikipedia , lookup
Sexual racism wikipedia , lookup
Human male sexuality wikipedia , lookup
Human female sexuality wikipedia , lookup
Penile plethysmograph wikipedia , lookup
Sexual ethics wikipedia , lookup
Lesbian sexual practices wikipedia , lookup
Homosexualities: A Study of Diversity Among Men and Women wikipedia , lookup
Human sexual response cycle wikipedia , lookup
History of human sexuality wikipedia , lookup
Rotherham child sexual exploitation scandal wikipedia , lookup
Human mating strategies wikipedia , lookup
Sexual attraction wikipedia , lookup
Female promiscuity wikipedia , lookup
Increased exposure to an HIV risk reduction protocol associated
with a reduction in drug abuse severity
1
Haynes ;
1
Carter ;
1
Herrin ;
2
Calsyn
Louise F.
Rickey E.
Amy E.
Donald A.
1Medical University of South Carolina, Southern Consortium Node;
2University of Washington, Washington Node,
NIDA Clinical Trials Network
Results
Introduction and Hypotheses
Previously, we reported that men in substance abuse (SA)
treatment randomized to a five-session HIV prevention
intervention reduced their sexual risk more than men
randomized to a single-session intervention. For the purpose
of this research, the association of the number of HIV
prevention sessions attended with reductions in risky sexual
behavior (RSB) and ASI composite scores was examined for
those participants randomized to the five-session intervention.
Specifically, the following hypothesis was tested:
Table 1 presents the sample description of the N=89
participants included in this analysis. The majority
(80%) reported engaging in risky sexual behavior at
baseline. A total of 20 (22%) of the included subjects
failed to attend any REMAS sessions, 35% attended
all five sessions, and the remaining 43% attended one
to four sessions. Table 2 presents the baseline drug
and alcohol use profiles of the sample at baseline.
Variable
Age (years)
Hypothesis: Participants who reduce their drug use will be
more likely to reduce risky sexual behavior and that the
number of HIV prevention sessions attended would enhance
the effect.
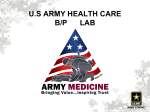
Figure 1 illustrates the baseline and three-month
mean number of RSB events and ASI-Lite composite
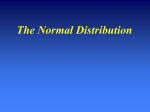
scores. Figure 2 dichotomizes each of these variables
to represent the percentage of subjects that improved
over the course of follow-up by the number of
sessions attended.
Risky Sexual Behavior (any in past 30
days reported at baseline) {a}
Measures
SA measures were the alcohol (ALC) and drug (DRG)
composite scores from the ASI-Lite. Risky sexual behavior
(RSB) was defined as the number of vaginal and anal
intercourse acts without a condom, and the outcome for this
analysis was the change in RSB at three month follow-up
relative to baseline. A participant was considered to have
improved if there was a reduction in RSB at the three month
follow-up.
Mean (SD)
Methadone Treatment
Ethnicity
Hispanic
American Indian or Alaskan
Asian
Black
White
10
2
1
25
51
71
11.24
2.25
1.12
28.09
57.3
79.78
Table 1: Sample description (n=89)
{a} Risky Sexual Behavior is defined as the number of vaginal and anal
intercourse acts without a condom
The odds for an improvement in RSB (i.e.,
40
0.40
reduction in RSB events) at follow-up
30
0.30
significantly increased as the number of
sessions attended increased (p=0.032). In
0.20
20
addition, the odds for a reduction in the
DRG composite score similarly increased
10
0.1
with session attendance (p=0.049), yet this
association did not mediate the effect of
0.0
0
Baseline
3 month follow-up
the number of sessions on RSB. The
RSB
ASI-DRG
ASI-ALC
number of REMAS sessions was not found
to be associated with a reduction in ALC
Figure 1: Mean (SD) number of RSB events and
composite scores (p=0.66).
ASI-Lite composite scores (n=89).
The SD for RSB is 60.94 at baseline and 39.4 at three-month
follow-up.
100%
90%
Baseline Use
D1 Alcohol
D2 Alcohol (to intoxication)
D3 Heroin
D4 Methadone (presribed)
D4a Methadone (illicit)
D5 Other Opiates/Analgesics
D6 Barbiturates
D7 Sedatives/Hypnotics/Tranquilizers
D8 Cocaine
D9 Amphetamines
D10 Cannabis
D11 Hallucinogens
D12 Inhalants
D13 More than 1 substance per day
Lifetime (years)
Mean
SD
4.28
1.84
0.74
16.38
0.07
1.60
0.00
3.57
2.81
0.32
3.55
0.06
0.01
10.63
11.07
7.33
6.96
1.91
0.11
2.42
0.54
1.58
6.10
2.66
9.45
0.82
0.38
12.53
Composite Scores, mean (SD)
ALC
DRG
8.27
4.51
2.29
14.91
0.33
5.80
0.00
8.71
6.42
1.09
7.73
0.38
0.11
12.69
11.17
9.35
9.08
3.26
0.53
5.26
2.11
3.96
7.48
4.65
9.65
2.07
1.93
10.62
0.13 (0.20)
0.19 (0.14)
Table 2: ASI-Lite Drug and Alcohol Use at Baseline
Conclusions
0.50
50
These data suggest that an overall reduction in RSB and DRG was
associated with increased exposure to the REMAS intervention.
A limitation of this analysis is that it only examines correlations among
patients who self-selected the amounts of their REMAS exposure, so any
suggestion of causality would be speculative. Another limitation is the
possible confounding. Men who attended more sessions would have been
exposed to additional substance abuse treatment. This could cause the ASI
improvements.
Further research is needed to examine if reductions in RSB are linked to
reductions in incident cases of HIV and other STDs and to better
understand the potential confounding effects of a participants willingness to
remain in treatment since those who attended more sessions may have
been more highly motivated to change than those who did not attend as
many sessions.
80%
% Improved
70%
Statistical Considerations
Binary indicator variables were created to indicate
improvement in RSB, ALC and DRG. Improvement was
defined as a decrease in scores at three-month follow-up
compared to baseline. Logistic regression was used to model
the log odds of improvement in each measure as a function of
the number of sessions attended. To assess if reductions in
DRG mediated the effect of the number of sessions attended
on RSB improvement, a multiple logistic model was
considered.
%
38.1 (10.3)
ASI Composite Scores
Participants
Of the 291 men randomized into the Real Men Are Safe
(REMAS) intervention, this analysis focuses on the n=89 who
had both baseline and three-month follow-up assessments
and who reported having more than one sexual partner during
the period six months prior to and throughout the study.
n
# of RSB events
Methods
Level
Past 30 days
Mean
SD
References
60%
50%
40%
30%
20%
10%
0%
0 (n=20)
1 (n=10)
2 (n=6)
3 (n=5)
4 (n=17)
5 (n=31)
1. Calsyn, Donald A.; Hatch-Maillette, Mary; Doyle, Suzanne R; Berns, Sara; Crits-Cristoph, Paul; Song,
Yong S; Harrer, Judith M; Lalos, Genise. “Efficacy of a Gender Specific HIV Prevention of Men in
Substance Abuse Treatment.” Poster presented at the XVI International AIDS Society (IAS) Conference,
Toronto, Canada, August 13-18, 2006.
2. Calsyn Donald A et al. “Primary Results from CTN Safer Sex Skills Groups for Men”. Symposium XVII at
The College of Problems of Drug Dependence (CPDD) Conference, Quebec City, Quebec, Canada, June
15-21, 2007.
# Sessions Attended
RSB
ASI-DRG
ASI-ALC
Acknowledgements
Figure 2: Percent of subjects that improved by number of sessions attended (n=89)
*Note: Improvement is defined as a decrease in the number of RSB events or a decrease in the ASI-DRG and
ASI-ALC scores at three-month follow-up compared to baseline
This study is funded by the following grants from the National Institutes of Health: DA013727, DA013714. The
consortium performing this study was a part of the Clinical Trials Network (CTN) established by the National Institute on
Drug Abuse (NIDA).