Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
MODELING CARDIOVASCULAR AND RESPIRATORY DYNAMICS IN
CONGESTIVE HEART FAILURE
LAURA M. ELLWEIN1 , SCOTT R. POPE2 , ALIANG XIE3 , JERRY J. BATZEL4 , C.T. KELLEY5 , METTE
S. OLUFSEN5
1) Olin Engineering Center, Marquette University, 1515 West Wisconsin Av, Milwaukee, WI
2) SAS, 100 SAS Campus Drive, Cary, NC
3) Pulmonary Physiology Laboratory, William S. Middleton Veterans Hospital,
2500 Overlook Tarace, Madison, WI
4) Inst. for Math. and Scientific Computing, Univ. of Graz, Heinrichstrasse 36, Graz, Austria
5) Dept. of Mathematics, North Carolina State University, Campus Box 8205, Raleigh, NC
Abstract. This study develops a coupled cardiovascular-respiratory model that predicts cerebral
blood flow velocity (CBFV), arterial blood pressure, end-tidal CO2 , and ejection fraction for a
patient with congestive heart failure. The model is a lumped parameter model giving rise to
a system of ordinary differential equations. We use sensitivity analysis and subset selection to
identify a set of model parameters that can be estimated given the patient data. Gradient based
nonlinear optimization is used to estimate the subset of parameters. Optimization was caried out
first for the cardiovascular submodel and subsequently for the respiratory model. Once a set of
optimal parameters were found, the coupled model was computed to confirm that the model is still
able to predict the observed data. Results showed that with the approach and methods presented
in this paper it is possible to examine and quantify identifiability of model parameters. Using
this approach we identified 5 key cardiovascular parameters and 4 key respiratory parameters.
Nonlinear optimization techniques was used to estimate these parameters and we tested that values
for all parameters were physiologically reasonable for a patient with congestive heart failure.
1. Introduction. The strong pathophysiological links between sleep-related breathing disorders
and cardiovascular diseases have recently received raised attention among clinicians and researchers.
On one hand, sleep-related respiratory disorders, especially obstructive apneas, have been identified
as an independent risk factor for hypertension, myocardial infarction and stroke due to the associated recurrent upper airway vibration, intermittent hypoxia, surges of sympathetic neural activities,
and repetitive arousals and resulting sleep fragmention a (see for example [23, 16]). Central sleep
apnea has been considered a marker for congestive heart failure (CHF) and also been associated with
the deterioration of heart function in CHF [21]. On other hand, epidemiological data reveal that
about one-half of patients with CHF develop periodic breathing [17, 53]. CHF is characterized by a
reduction in cardiac output, elevation of left atrial pressure and pulmonary capillary wedge pressure,
accumulation of fluid in the lung, reduced functional residual capacity (FRC), and prolongation of
circulation time. All of these factors may destabilize breathing. In fact, a greater central and peripheral chemosensitivity to CO2 (i.e., controller gain) has been observed in CHF patients [54, 9] and
CHF animal models [57]. Respiratory changes duiring sleep combined with these cardiovascular and
control sensitivity changes can contribute to the occurrence of sleep apnea ([12, 37, 4]. Furthermore,
the low cardiac output also reduces brain perfusion [9, 36] and attenuates cerebrovascular chemosensitivity [22, 63]. The combination of hypoperfusion and low cerebrovascular reactivity impairs the
CBF protective mechanism for breathing stability [64]. Finally, CHF and its concomitant cardiovascular insufficiency and potential for reduced cerebral perfusion has been associated with impaired
cognitive function [5], while syncope is an issue in patients with CHF [26]. In general, although the
Key words and phrases. Cardiovascular modeling, Respiratory modeling, Parameter estimation, Model validation,
Sensitivity analysis, Subset selection.
1
2
L.M. ELLWEIN, S.R. POPE, A. XIE, J. J. BATZEL, C.T. KELLEY, M.S. OLUFSEN
underlying mechanisms for the interaction between the respiratory disorders and cardiaovascular
disorders have not fully understood, the two disorders eventually exacerbate each other, creating a
vicious cycle.
Modeling and especially models that can be applied in the clinical setting can contribute to the
development of methods for assessment of respiratory function such as estimating central and peripheral control gain and CO2 reactivity. Models can also provide insight into the control mechanisms
that govern respiratory function, respiratory interaction with cardiovascular control, and mutual
regulation between ventilation and cerebral blood flow (CBF) through partial pressure of arterial
CO2 .
Recent models that address aspects of the above topics include work by Dong and Langford [13],
which developed a model to study factors affecting stable behavior of the cardiovascular-respiratory
system in heart failure and Bidini et al. [38, 39] who applied a combined cardiovascular-respiratory
model to study the Valsalva maneuver and factors affecting cerebral blood flow. Recent experimental
studies include work investigating the differential role of partial pressures of CO2 and sympathetic
response on vasoconstriction [1], and the role of cerebral vascular function in setting ventilatory
response via influence on CO2 [63].
Thus, mathematical models that integrate ventilatory and cardiovascular system dynamics and
control functions have the potential to be used as a diagnostic tool as well as to obtain more
detailed knowledge of the dynamics of the underlying complex systems including aspects related to
cardiovascular diseases. Furthermore, models that can be used to investigate the cardiovascularrespiratory coupling both in health and disease has potential to help understanding and diagnosing
clinical conditions. To understand this complex dynamics models should be applicable for analyzing
dynamics during typical orthostatic and ventilatory tests such postural change, step changes in
inspiratory CO2 concentrations, or rhythmic breathing at various rates. These requirements indicate
that models should include a fair degree of complexity. On the other hand, for a given model
to have an impact in clinical settings, it is essential that the model can predict patient specific
outcomes such as systemic and cerebrovascular resistances. The latter is often studied by solving
an inverse problem, using a model combined with experimental data to predict patient specific
parameters that minimize the difference between observed and computed quantities such as arterial
blood pressure, cerebral blood flow velocity, or end-tidal CO2 . However, estimating parameters
from complex nonlinear models is difficult, in particular since parameters may be correlated or not
sensitive to given observations. Developing better techniques for analyzing such complex data is the
main focus in this manuscript.
To achieve an effective compromise between model complexity and clinical application requires
a modular approach to model analysis. This entails several considerations. First, model reduction
should be applied to reflect only the key functional elements under investigation. This simplifies
the parameter estimation problem but care needs to be taken to avoid loss of the models’ predictive
power. Second, a given model must be analyzed with regard to available data so that key model parameters sensitive to the observed data can be effectively and reliably estimated within a reasonable
time frame. Other less sensitive parameters should be estimated using information from literature,
statistics, or allometric scaling. Conversely, sensitivity analysis can provide suggestions for experimental design. However, sensitivity analysis alone does not fully enable estimation of all model
parameters. Therefore, this analysis must be coupled with a more advanced analysis investigating
correlations between model parameters, e.g., two correlated sensitive parameters should not both be
estimated.
This study develops a coupled pulsatile cardiovascular-respiratory model applicable to clinical
problems related to CHF. We use sensitivity analysis to rank model parameters from the most to
the least sensitive with respect to the available data. Furthermore, we study correlation of model
parameters using subset selection.
CARDIOVASCULAR & RESPIRATORY DYNAMICS IN CONGESTIVE HEART FAILURE
Vcv Ccv
3
Cca Vca
Rc
qc
Cerebral Tissue
cB,g
pcv
pca
MB,g
Head
Rcv
Vpa Cpa
Cpv Vpv
ppa
Lungs
qpa
qcv
Rpv
Vsv Csv
qsv
psv
Rtv
pa,g
qpv
VD
ca,g
pD2,g
pD1,g
prv
Erv Vrv
Right
Ventricle
qsa
plv
pI,g
Vlv Elv
pexp,CO2
Rs
qca
Rmv
pD3,g
csv,g
Rca
ppv
qp
Rp
Left
Ventricle
Csa Vsa
psa
Rav
Thorax
qs
Systemic Tissue cS,g
Body
MS,g
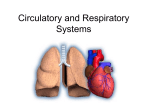
Figure 1. Compartmental model of systemic and pulmonary circulations. Systemic (subscript s),
cerebral (subscript c), and pulmonary (subscript p) arteries (subscript a) and veins (subscript v);
Vessels carrying oxygenated blood (systemic arteries and pulmonary veins) are red, while vessels
carrying deoxygenated blood (systemic veins and pulmonary arteries) are blue. All vascular compartments represent a group of vessels with similar pressure p [mmHg]. Each vascular compartment
is characterized by its volume V [ml] and compliance C [ml/mmHg]. The left (dark red, subscript lv)
and right (dark blue, subscript rv) ventricles generate pulsatile pressure plv , prv [mmHg]. These two
compartments are defined using time-varying elastance E [mmHg/ml]. Flow q [ml/sec] between compartments are opposed by constant resistances R [mmHg sec/ml]. Tissue compartments (magenta)
account for exchange of gases (O2 and CO2 ). Each vascular bed is characterized by a metabolic
rate M [mlST P D /sec], and the gas concentrations in the tissues are denoted by c [mlST P D /ml]. The
lungs are represented by three dead-space compartments each predicting the partial pressure of the
gases pDi,g [mmHg]. The partial pressure of the gases in the inspired air pI,g , and the end tidal
partial pressure of expiratory CO2 pexp,CO2 are marked separately.
2. Methods. The cardiorespiratory model depicted in Figure 1 is a lumped parameter compartmental model designed to predict systemic arterial blood pressure psa , cerebral blood flow velocity
vc , and end tidal partial pressure of expiratory CO2 pexp,CO2 for a CHF patient resting in supine
position.
For the purposes of this paper, we are considering dynamic oscillatory variations in cardiovascular
and respiratory system quantities around a resting steady state. Hence, control mechanisms are not
responding to system stress and control responses are not directly invoked. For this reason we do
not consider control submodels in this study. Note also that H and V̇IE are inputs to the model so
that variations in the controls of these quantities are implicitly included in the model.
4
L.M. ELLWEIN, S.R. POPE, A. XIE, J. J. BATZEL, C.T. KELLEY, M.S. OLUFSEN
2.1. Cardiovascular system. The cardiovascular system (see Figure 1) is represented by a closed
circuit with 3 arterial compartments, 3 venous compartments, and 2 ventricular compartments.
Vascular compartments represent systemic arteries and veins in the body and the brain, as well as
pulmonary arteries and veins. Each compartment lumps vessels with similar transmural pressure
p(t) [mmHg], volume V (t) [ml], and compliance C [ml/mmHg] (constant). For each compartment i,
the stressed volume Vi,str (t) is given by
Vi,str (t) = Vi (t) − Vi,unstr = Ci pi (t),
(1)
where Vi (t) [ml] is the time-dependent total volume and Vi,unstr [ml] (constant) is the unstressed
volume, at zero transmural pressure.
Flow between adjacent compartments are characterized by a constant resistance R [mmHg sec/ml]
and volumetric flow rate q(t) [ml/sec]. Incorporating Ohm’s law, the net change in volume for each
compartment is given by
dVi (t)
= qin (t) − qout (t),
dt
qin (t) =
pi−1 (t) − pi (t)
,
Rin
qout (t) =
pi (t) − pi+1 (t)
.
Rout
(2)
The subscripts i − 1 and i + 1 refer to upstream and downstream compartments in relation to
compartment i, respectively. A system of differential equations is obtained by differentiating (1)
and equating with (2),
dpi (t)
qin (t) − qout (t)
.
(3)
=
dt
Ci
An equation of this form is associated with each vascular compartment.
The heart is represented by the left and right ventricles, modeled to generate the driving pressures
for the systemic and pulmonary systems. This is realized by imposing a time-varying pressure
predicted as a function of ventricular volume. Thus, for the ventricular compartments we obtain a
differential equation by imposing volume conservation, i.e.,
dViv (t)
= qin (t) − qout (t), i = l, r
(4)
dt
where the flows q are determined similarly to (2). We use a time-varying elastance model to predict
ventricular pressures piv (t) [48, 51, 55, 60],
piv (t) = Eiv (t)[Viv (t) − Vid ],
i = l, r,
(5)
where Vd [ml] denotes the volume at zero end-systolic pressure [48, 52] and Eiv (t) [mmHg/ml] denotes
the time-varying elastance. In the above equations subscript i denote the left and right ventricles,
respectively. For each ventricle, time-varying elastance E(t) is modeled using a piecewise sinusoidal
function of the form
πt
/2 + Em
0 ≤ t ≤ TM
(EM − Em ) 1 − cos
TM
(6)
E(t) = (E − E ) cos π(t − TM ) + 1 /2 + E
m TM ≤ t ≤ TM + TR
M
m
T
R
Em
TM + TR ≤ t ≤ T,
where TM and TR denote the time for maximum (systolic) elastance (TM ) and the remaining time to
relaxation (TR ). To account for varying heart rate, we express these times as fractions of the heart
period T , i.e., TM,f rac = TM /T and TR,f rac = TR /T . We assume that peak elastance occurs at the
same time for both left and right ventricles; thus we assume that the values of the two parameters
TM and TR remain the same between the two sides of the heart. Em and EM denote that minimum
and maximum elastance of each ventricle. The maximum and minimum elastance differ significantly
between the right and the left ventricle, in particular for the CHF patient studied in this manuscript.
CARDIOVASCULAR & RESPIRATORY DYNAMICS IN CONGESTIVE HEART FAILURE
5
Thus we include four elastance parameters Eml , Emr and EMl , EMr and two timing parameters TM
and TR .
Similar to previous studies [45, 14, 50], the ventricular valves are modeled using time-varying
resistances {Rmv (t), Rav (t), Rtv (t), Rpv (t)} defined as a function of the pressure drop across the
valves. A small baseline resistance is used to define an “open” valve (subscript “o”) and a resistance
that is several orders of magnitude larger is used to define the “closed” valve (subscript “c”). An
exponential function is applied to describe the degree of openness as a function of the pressure
gradient. The effective resistance of a valve is then defined by
i
h
(7)
Rvalve = min Rvalve,o + e−k(pin −pout ) , Rvalve,c .
The parameter Rvalve,o is the small resistance allowing flow out of the ventricle, k describes the
speed of the transition from open to closed, and Rvalve,c is a value large enough to effectively shut
off the flow through the valve. Since this function is non-smooth at the junctions of the exponential
and Rvalve,c , a smoothing function [11]
!
X
exp(xi /ε) ,
min(x) = −ε log
ε
i
where 0 < ε < 1 denotes the degree of smoothness (in this study we used ε = 0.5) and x denote the
vector to be minimized.
All equations and initial conditions for the cardiovascular model are given in the Appendix.
2.2. Respiratory system. The respiratory system is modeled using components allowing for gas
exchange, transport, and metabolism. We model the dynamics of the two metabolite gases, O2 and
CO2 , while we do not account for inert gases such as N2 . As shown in Figure 1, a tissue compartment
connects each peripheral arterial compartment with each peripheral venous compartment. Dynamic
gas concentrations in each tissue compartment reflect O2 consumption and CO2 production during
metabolism as well as convection via blood flow into and out of each compartment. The model
also includes two pulmonary components. The alveolar space has a dynamic volume, in which O2
and CO2 are exchanged between the lungs and the pulmonary vasculature. The lungs have been
modeled using rigid dead space compartments connecting the alveolar space with the atmosphere.
The rigid-walled dead space is divided into three compartments of the same size to account for some
of the effects of the pulmonary branching. Gas concentrations and partial pressures are predicted in
all compartments. The inputs to the model include HR and volumetric airflow V̇IE , which provides
information about tidal volume VT and ventilation frequency fR .
Standard material balance equations describe respiration in the tissue compartments. The following symbol convention will be used: c represents concentration, T represents a generic tissue
compartment which can be chosen to be systemic tissue S or brain tissue B. Generic gas quantity
is denoted by g and gas fractional amount by F . Venous outflow is denoted by v and arterial inflow
by a. Thus we denote the total amount of a gas in a tissue compartment by AT,g [ml] which is given
by
AT,g = VT,g cT,g .
This equation describes AT,g by the product of the effective tissue volume V [ml] (constant) available
for the gas and the concentration c [mlgas /mlblood ] of the gas in the volume. The change in amount of
gas in a compartment is equal to the sum of the amount of gas produced or consumed by metabolism
M [ml/sec] and the amount added or removed by the bloodstream qT [ml/sec].
dcT,g
dVT,g
dAT,g
=
cT,g + VT,g
= MT,g + qT (ca,g − cT,g ).
dt
dt
dt
6
L.M. ELLWEIN, S.R. POPE, A. XIE, J. J. BATZEL, C.T. KELLEY, M.S. OLUFSEN
Note, the concentration in the systemic arteries (i.e., in the body and the brain) are the same, since
no metabolism has been accounted for on this side. Hence we denote the arterial concentration for
ca . Thus, Assuming dVT,g /dt = 0, this equation reduces to
dcT,g
= MT,g + qT (ca,g − cT,g ).
(8)
dt
The tissue compartments are considered well-mixed and equilibrated with exiting venous concentration. Note that the gas concentration csv,g is calculated as a mixture of the concentrations from the
incoming systemic venous stream qs and cerebral stream qcv so that
cS,g qs + cB,g qcv
,
csv,g =
qs + qcv
where cS,g and cB,g are the systemic and cerebral concentrations of each gas, respectively.
Let A denote the alveolar compartment; then the quantity of alveolar gas is given by
VT,g
VA,g = VA FA,g ,
which is the product of alveolar volume VA and gas fraction FA,g . The change in quantity of alveolar
gas is represented by a mass balance relation parallel to the one developed for the tissue compartment,
taking into account this time a time-varying alveolar volume, and with gas transport via fluid flowing
to and from the lungs via pulmonary capillaries, and gas exchange with environment via inspiration
and expiration. Let subscript p represent the pulmonary compartment. Thus we have,
dVA,g
dVA
FA,g
dVA
= FA,g
+ VA
=
Fi,g + qp (csv,g − ca,g ).
dt
dt
dt
dt
In this representation Fi,g denotes the fraction of gas in the air that is either being inspired or expired
into the alveolar compartment. Hence, i = D3 during inspiration since inspired air is coming from
the adjacent dead space region and i = A during expiration since air leaving the alveoli is alveolar
air equilibrated with the pulmonary capillaries. Rearranging to express the rate of change of alveolar
gas fraction gives
dVA
dFA,g
(FD3 ,g − FA,g ) + qp (csv,g − ca,g ), inspiration
=
VA
dt
q (c
dt
expiration.
p sv,g − ca,g ),
Gas fractions are converted to partial pressures via the relationship
FA,g = pA,g /(pamb − pwater ) = pA,g /713,
where pamb is the ambient air pressure of 760 mmHg and water vapor partial pressure pwater equals
47 mmHg at body temperature of 37◦ , i.e.,
dVA (pD3 ,g − pA,g )
VA dpA,g
+ qp (csv,g − ca,g ), inspiration
=
dt
713
q (c
713 dt
expiration.
p sv,g − ca,g ),
Because blood gas concentrations are reported in [mlST P D /ml] (STPD is the Standard Temperature
(0◦ C), barometric Pressure at sea level and Dry gas), but alveolar volumes are in BTPS (standardized to Body Temperature, barometric Pressure at sea level, Saturated with water vapor: body
temperature and pressure, saturated), we convert tissue concentrations to BTPS. Incoming air is
immediately humidified once it enters the nasal passages [7, 8] and expired air is a composition of
alveolar air and dead space air at BTPS, therefore terms with those quantities are not converted.
The final equations are obtained by using the conversions and multiplying through by 713, i.e.,
dVA
dpA,g
(pD3 ,g − pA,g ) + 863 · qp (csv,g − ca,g ), inspiration
(9)
VA
=
dt
863 · q (c
dt
− c ),
expiration.
p
sv,g
a,g
CARDIOVASCULAR & RESPIRATORY DYNAMICS IN CONGESTIVE HEART FAILURE
7
Additional modeling considerations concern the relationship between the pulmonary capillaries and
the systemic arteries. First, an anatomical shunt is present in the pulmonary circulation. This consists of O2 -deficient blood that bypasses the alveoli for physiological or pathological reasons. Typical
shunt values range from 2-5%, with a larger shunt percentage possibly indicating a pathological condition [8, 7]. The subject studied has no known pulmonary health issues so we assume a 2% shunt.
Therefore only 98% of the cardiac output becomes oxygenated, altering the alveolar equations to
read as
dVA
dpA,g
(pD3 ,g − pA,g ) + 0.98 · 863qp (cv,g − ca,g ), inspiration
=
(10)
VA
dt
0.98 · 863q (c − c ),
dt
expiration.
p v,g
a,g
Second, we note that the thin alveolar wall allows for almost immediate equilibration of gases between
the alveoli denoted by A and the pulmonary capillaries; thus we assume that the concentrations of
blood gases is the same in the pulmonary capillaries and in the systemic arteries. This concentration
is denoted by psa,g , i.e., we assume pA,g = psa,g as an auxiliary equation.
Connected to the alveolar compartment are three compartments of equal volume with a total volume representing anatomical dead space. Each dead space is considered a well-mixed compartment
with units VBT P S , in ml. Material balance equations for the dead space compartments reflect change
in gas levels due to airflow, with opposite directions of flow for inspiration versus expiration. The
relation FA,g = pA,g /713 holds, and equation units are all in BTPS. Thus following the derivation
of (10),
dpD1 ,g
dt
dpDi ,g
VDi
dt
dpDi ,g
Expiration: VDi
dt
dpD3 ,g
VD3
dt
Inspiration: VD1
=
=
=
=
dVA
(pI,g − pD1 ,g ),
dt
dVA
(pDi−1 ,g − pDi ,g ), i=2,3.
dt
dVA
(pDi ,g − pDi+1 ,g ), i=1,2,
dt
dVA
(pD3 ,g − psa,g ).
dt
(11)
(12)
Pressure pI,g is the partial pressure of the gas in the inspired air.
Note that dVA /dt is positive during inspiration and negative during expiration. The rate of change
of alveolar volume dVA /dt is equivalent to the ventilation airflow V̇IE . Thus, the alveolar volume
can be predicted as
Z
(13)
VA = V̇IE dt.
To give a correct value for the alveolar volume, additional information is needed to offset the integration constant. We have chosen to adjust this assuming that the minimum alveolar volume should
match the FRC [ml], which we determine as a function of height H [cm] and weight W [kg], i.e., we
assume
min(VA ) = FRC,
FRC = (3.8 · H/100 − 3.41 · W/H − 2.74) · 1000
The above estimation for FRC is based on work by Stocks and Quanjer [56]. Furthermore, it should
be noted that the use of the ”dot” notation in V̇IE is a standard way to indicate a volumetric flowrate
as opposed to a rate of change of volume. The airflow V̇IE is measured during experimentation and
is used as an input to the model to drive the gas concentration dynamics.
O2 and CO2 have different affinities for hemoglobin, therefore behave differently in the gas versus liquid phases. Gas dissociation laws are used to convert alveolar gas pressures to blood gas
concentrations.
8
L.M. ELLWEIN, S.R. POPE, A. XIE, J. J. BATZEL, C.T. KELLEY, M.S. OLUFSEN
In this study we use equations also used by Batzel et al. [4],
cT,CO2
=
KCO2 pT,CO2 + kCO2 ,
cT,O2
=
K1 (1 − e−K2 pT ,O2 )2 .
Note that the law for CO2 is linear while the law for O2 is exponential. This reflects general behavior,
but does not account for the the dependencies of each gas on the other (Bohr and Haldane effects)
as well as factors such as pH and temperature.
All respiratory equations and initial values are listed in the Appendix.
3. Experimental Methods. The data analyzed in this study include continuous (sampled at
128 Hz) measurements of systemic arterial blood pressure (psa ), cerebral blood flow velocity vc
measured from the middle cerebral artery (MCA), and end tidal partial pressure of CO2 in expiratory
air. In addition we have a measure for left ventricular ejection fraction, as well as anthropometric
measurements of height, weight, and gender. These data are obtained from Dr. Skatrud’s group,
Department of Medicine, University of Wisconsin.
The subject is a male age 55, height 178 cm, weight 82.3 kg with CHF but no known sleep apnea
syndrome. Data used for this study were recorded while the subject was in semirecumbent position
during normal breathing (for 10 min). Experiments were started between 8.00 and 9.00 am, to
standardize the effect of diurnal variability of cerebral vasomotor reactivity [2].
A 2-MHz pulsed Doppler ultrasound system (Neurovision 500 M; Multigon Industries, Yonkers,
NY) was used to continuously measure cerebral blood flow velocity in the proximal segment of the
middle cerebral artery (MCA). The MCA was insonated through the right temporal bone window
using search techniques described in Otis and Ringelstein [46]. After detection and optimization of
the Doppler signal, the probe was mechanically secured using a headband device and probe holder
to provide a fixed angle of insonation for the duration of the experiment. The subject, in the
semirecumbent position, was asked to keep his head still and eyes open throughout the experiment.
Heart rate was obtained from the electrocardiogram, and arterial pressure (psa ) was measured beat
by breat in the middle finger of the left hand by photoelectric plethysmography (Finapres, Ohmeda,
Louisville CO). Tidal volume (VT ) and breathing frequency were measured with a pneumotachograph
Model 3700, Hans Rudolph, Kansas City, MO) that was attached to a leak-free nasal mask. End
tidal PETCO2 tensions was sampled from the mask and measured by gas analyzers (#S-3A/I &
CD-3; Ametek, Pittsburgh PA). Detailed descriptions of the experimental protocol can be found
in [63].
4. Parameterization.
4.1. Cardiovascular parameters. Nominal parameter values and initial conditions for the cardiovascular model were estimated from the subject’s anthropometric measurements. A complete list of
all initial parameter values can be found in Table 1. We start by setting up predictions for nominal
parameter values used to predict time-varying elastance. Parameters needed include maximum and
minimum elastance of the left ventricle (EMi , Emi , i = l, r), as well as fractions predicting the timing
of the cardiac cycle (TM,f rac , TR,f rac ).
Nominal parameter values for end diastolic elastance are obtained from estimated diastolic ventricular pressure pdia , end diastolic volume EDV, and zero pressure volume Vd as
piv,dia
,
i = l, r.
Emi =
EDViv − Vid
Diastolic ventricular pressures are set using literature values [29]. The subject studied has CHF and
is thus expected to have an enlarged left ventricle, while the size of the right ventricle is closer to
normal. We estimate these volumes using results for CHF patients without sleep-apnea reported by
Tkacova et al. [59].
CARDIOVASCULAR & RESPIRATORY DYNAMICS IN CONGESTIVE HEART FAILURE
9
End systolic elastances are estimated using a similar relation, but as functions of systolic ventricular pressure psys , end systolic volume ESV, and zero pressure volume Vd . Systolic ventricular
pressure is obtained from the maximum measured arterial pressure. End systolic volume is obtained
by subtracting stroke volume (SV) from the end diastolic volume: ESV = EDV − SV. Stroke volume
is estimated from end left ventricular diastolic volume and ejection fraction (EF, measured 26% for
the subject studied): SV = EF · EDVlv .
The timing fractions TM,f rac and TR,f rac were estimated from literature values suggested by
Ottesen and and Danielsen [47] and Heldt [30]. We assume that the ejection of the left and the right
sides of the heart are synchronous, thus we use the same values for both ventricles.
Initial values for blood pressures were obtained partly from the data and partly from literature
estimates. All arterial pressures were scaled relative to the measured arterial pressure, whereas
venous pressures were set using standard literature values. Initial blood pressures were used both
in computation of initial resistances and compliances and as initial conditions for the differential
equations.
Initial flows were scaled to cardiac output, which was computed from stroke volume SV and mean
heart rate HR, i.e., CO = SV · HR. Mean heart rate was obtained from the measurements. Flows
in the circuit was distributed to let 20% cardiac output go to the brain, while 80% was directed to
the systemic arteries.
Resistors were predicted using Ohm’s law as
R=
pi − pi+1
qi
and compliances were predicted using the pressure volume relation (1). Estimates of total blood
volume was computed as a function of body surface area (BSA, m2 ), estimated from Mosteller’s
formula [42]
p
BSA = (W · H)/3600,
where W is the subjects weight in kg and H is the subjects height in cm. Total blood volume (ml)
was computed using Baker’s formula [3] as
Vt = (23.9 · BSA − 1.229) · 1000.
Distributions of volume and prediction of unstressed volumes were obtained using values from
Beneken and DeWitt [6].
4.2. Respiratory parameters. Nominal values for metabolic rates and tissue volumes are given
in Table 2. As is standard practice, all tissue gas volumes and blood gas concentrations are given
in STPD, thus units are consistent. Metabolic rates were set using standard allometric scaling
proportional to body mass by the power of 3/4 [61, 62] using values in Table 2. We used metabolic
rates given in [4, 34, 27] for total systemic (including both the body and the brain) CO2 (MCO2 ) and
O2 (MO2 ) combined with a metabolic rate for the brain for CO2 (MB,CO2 ). To compute metabolic
rates for oxygen in the brain MB,O2 we assumed that the ratio of metabolism between oxygen and
carbon dioxide in the brain was approximately equal to one given that brain tissue burns primarily
carbohydrate (glucose) ([27]). Finally, we used these four metabolic rates to adjust metabolic rates
in the body. Similarly, for volumes of the gases we used total systemic volumes and brain volumes
to get the volumes in the body, based on values given by Batzel [4]. Alveolar volume was a dynamic
quantity as shown in (13). Dead space volume was set proportional to the body weight in pounds
(the subject weight 82.3 kg or 181.3 lbs). Finally, the coefficients of the dissociation equations are
assumed to be independent of the size of the subject.
10
L.M. ELLWEIN, S.R. POPE, A. XIE, J. J. BATZEL, C.T. KELLEY, M.S. OLUFSEN
Table 1. Nominal values for all cardiovascular parameters.
Parameter
EDVlv [ml]
EDVrv [ml]
EF
SV [ml]
ESVl
ESVr
HR [bpm]
CO [l/min]
pdsa [mmHg]
plv,sys [mmHg]
prv,sys [mmHg]
plv,dia [mmHg]
plv,dia [mmHg]
ppa [mmHg]
ppv [mmHg]
psa [mmHg]
psv [mmHg]
pca [mmHg]
pcv [mmHg]
qs [ml/sec]
qca , qc , qcv [ml/sec]
qpa , qpv [ml/sec]
Rmv , Rav [mmHg sec/ml]
Rtv , Rpv [mmHg sec/ml]
Rs [mmHg sec/ml]
Rca [mmHg sec/ml]
Rc [mmHg sec/ml]
Rcv [mmHg sec/ml]
Rp [mmHg sec/ml]
Vsa [ml]
Vsv [ml]
Vca [ml]
Vcv [ml]
Vpa [ml]
Vpv [ml]
Csa [ml/mmHg]
Csv [ml/mmHg]
Cca [ml/mmHg]
Ccv [ml/mmHg]
Cpa [ml/mmHg]
Cpv [ml/mmHg]
Ac [cm2 ]
Physiologic description
End diastolic volume (left ventricle)
End diastolic volume (right ventricle)
Ejection fraction
Stroke volume
End systolic volume (left ventricle)
End systolic volume (right ventricle)
mean heart rate
Cardiac output
Measured arterial pressure
Systolic left ventricular pressure
Systolic right ventricular pressure
Diastolic left ventricular pressure
Diastolic right ventricular pressure
Pulmonary arterial pressure
Pulmonary venous pressure
Systemic arterial pressure
Systemic venous pressure
Cerebral arterial pressure
Cerebral venous pressure
Systemic flow
Flow in cerebral circulation
Flow in pulmonary circulation
Mitral and aortic valve resistances
Tricuspid and pulmonary valve resistances
Systemic resistance
Cerebral arterial resistance
Cerebral resistance
Cerebral venous resistance
Pulmonary resistance
Systemic artrial blood volume
Systemic venous blood volume
cerebral arterial blood volume
Cerebral venous blood volume
Pulmonary arterial blood volume
Pulmonary arterial blood volume
Systemic arterial compliance
Systemic venous compliance
Cerebral arterial compliance
Cerebral venous compliance
Pulmonary arterial compliance
Pulmonary venous compliance
Cerebral scaling factor
Value
312
100
0.26
EF · EDVl
EDVl − SV
EDVr − SV
Reference
[59]
[8, 29]
measured
measured
SV · HR
max(pdsa )
30
3
6
20
3.3
pdsa
6.6
psa · 0.99
7
0.8 CO
0.2 CO
[8, 29]
0.001
0.001
(psa − psv )/qs
(psa − pca )/qca
(pca − pcv )/qc
(pcv − psv )/qcv
(ppa − ppv )/qp
0.1178 · Vt
0.6091 · Vt
0.237 · Vt
0.936 · Vt
0.0288 · Vt
0.1243 · Vt
0.3 · Vsa /psa
0.08 · Vsv /psv
0.22 · Vca /pca
0.08 · Vcv /pcv
0.58 · Vpa /ppa
0.11 · Vpv /ppv
0.3
measured
measured
[8, 29]
[8, 29]
[8, 29]
[8, 29]
[8, 29]
measured
[8, 29]
measured
[8, 29]
[8, 29]
[8, 29]
estimated
estimated
[6]
[6]
[6]
[6]
[6]
[6]
[6]
[6]
[6]
[6]
[6]
[6]
estimated
4.3. Parameter estimation. Model parameters discussed in the parameter above are obtained
using physiological considerations and allometric scaling, so even though they to some extend have
been adapted to the patient with CHF studied here, significant variations from these standard
values is to be expected. Below we discuss how to estimate model parameters though the solution to the inverse problem: given data for cerebral blood flow velocity vc , arterial blood pressure
psa , end tidal partial pressure of expiratory CO2 pexp,CO2 , and cardiac ejection fraction EF find
the set of parameters that minimize the difference between computed and measured values of the
observed quantities. The coupled model uses heart rate and airflow as inputs to predict these quantities. However, the model contains a large number of parameters (37) including 24 cardiovascular
parameters and 13 respiratory parameters. The cardiovascular parameters include 9 resistances
CARDIOVASCULAR & RESPIRATORY DYNAMICS IN CONGESTIVE HEART FAILURE
11
Table 2. Nominal values for metabolic rates, tissue volumes, and gas dissociation constants. All
values are adapted from [4, 34, 27].
Parameter
MCO2 [mlST P D /sec]
MO2 [mlST P D /sec]
MB,CO2 [mlST P D /sec]
MB,O2 [mlST P D /sec]
MS,CO2 [mlST P D /sec]
MS,O2 [mlST P D /sec]
VT,CO2 [mlST P D ]
VT,O2 [mlST P D ]
VB,CO2 [mlST P D ]
VB,O2 [mlST P D ]
VS,CO2 [mlST P D ]
VS,O2 [mlST P D ]
VA,CO2 [mlBT P S ]
VA,O2 [mlBT P S ]
VD [mlBT P S ]
K1 [mlST P D /ml]
K2 [mmHg−1 ]
KCO2 [mlST P D mmHg/ml]
kCO2 [mlST P D /ml]
Physiologic description
Systemic tissue metabolic rate of CO2
Systemic tissue metabolic rate of O2
Cerebral tissue metabolic rate of CO2
Cerebral tissue metabolic rate of O2
Systemic (body) tissue metabolic rate of CO2
Systemic (body) tissue metabolic rate of O2
Systemic tissue volume of CO2
Systemic tissue volume of O2
Cerebral tissue volume of CO2
Cerebral tissue volume of O2
Systemic tissue volume of CO2
Systemic tissue volume of O2
Alveolar tissue volume of CO2
Alveolar tissue volume of O2
Total dead space volume
Dissociation coefficient for O2
Dissociation coefficient for O2
Dissociation coefficient for CO2
Dissociation coefficient for CO2
Value
4.333
5.167
0.875
MB,CO2
MCO2 − MB,CO2
MO2 − MB,O2
15000
6000
900
1000
VT,CO2 − VB,CO2
VT,O2 − VB,O2
3200
2500
181.1
0.200
0.046
0.0065
0.244
R = {Rs ,Rca ,Rc ,Rcv ,Rp ,Rav,o ,Rmv,o ,Rpv,o ,Rtv,o }, 6 compliances C = {Csa ,Cca ,Ccv ,Csv , Cpa ,Cpv },
8 heart parameters θheart = {Vrd ,Vld ,Emr ,Eml ,EMr ,EMl ,TM,f rac , TR,f rac }, and a scaling factor Ac .
The respiratory parameters include 3 metabolic rates M = {MCO2 ,MO2 ,MB,CO2 }, 4 gas tissue volumes V = {VT,CO2 , VT,O2 , VB,CO2 , VB,O2 }, the lung dead space volume VD , 4 dissociation constants
K = {K1 ,K2 ,KCO2 ,kCO2 , }, and a fraction indicating alveolar air in the exiting air stream falv .
Solving this inverse problem uniquely is not possible using this complex model, since it is likely that
many combinations of these parameters can give rise to the same solution. Thus, the goal here is
to identify a limited set of uncorrelated parameters that can be estimated reliably. To do so, we
use sensitivity analysis to rank parameters from the most to the least sensitive, and we use subset
selection to select a set of uncorrelated parameters. Subsequently, we use gradient based nonlinear
optimization to estimate this reduced set of parameters, while the remaining parameters will be
fixed at their nominal values.
The data analyzed in this study comprise baseline values, thus it is essential that the solution
of the system allows all states to reach “steady state” (in this study steady state means that the
model should display steady oscillatory behavior). Timescales in the cardiovascular model are short,
and this model will reach steady state within a few cycles. However, the respiratory model operates
on much slower timescales. To analyze how long the model should run to reach steady state we
analyzed timescales for each of the two systems. Time constants in the cardiovascular model are all
of the same order of magnitude, while time constants in the respiratory model vary significantly. The
largest time constant in the respiratory model is associated with the effective systemic tissue CO2
volume, which is approximately 14.1 liter. To compare the two models, we look at time constants
related to cerebral arterial pressure pca and concentration of systemic tissue CO2 (cS,CO2 ). These
time constants appear in the equations
pca − pcv
1
psa − pca
dpca
,
−
=
dt
Cca
Rca
Rc
MS,CO2 + qs (ca,CO2 − cS,CO2 )
dcS,CO2
.
=
dt
VS,CO2
12
L.M. ELLWEIN, S.R. POPE, A. XIE, J. J. BATZEL, C.T. KELLEY, M.S. OLUFSEN
0.57
cS,CO2 [mlSTPD/ml]
0.565
0.56
0.555
0.55
0.545
0.54
0
1000
2000
3000
4000
time [sec]
5000
6000
7000
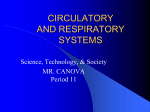
Figure 2. Dynamics of concentration of CO2 in the systemic tissue computed using nominal parameter value, sequence between the two vertical lines denotes the last sequence of the data.
The time constant for these two equations are approximately (Cca Rca Rc )/(Rca + Rc ) ≈ 0.0167
seconds and VS,CO2 /qs ≈ 257 seconds, respectively. These estimates indicate that we need long
sequences of baseline data to reach steady state dynamics. In this study we analyze 172 seconds of
data, thus to ensure steady state dynamics we repeat the data-segment 40 times to reach an end
time of approximately 7000 seconds. Figure 2 show dynamics of the tissue CO2 concentration.
Another important issue is that each respiratory cycle contain approximately 4-5 cardiac cycles,
requiring significantly smaller time steps to resolve cardiovascular dynamics than respiratory dynamics. Consequently, computation time for one simulation with the coupled cardiovascular-respiratory
model is approximately 23 min on a 3 GHz Mac Pro with 4 Dual-Core Intel processors and 12 GB
memory, rendering it computationally intensive to solve the parameter estimation problem using the
coupled model.
The cardiovascular and respiratory systems are weakly coupled. The respiratory model depends
on blood flow through the pulmonary, systemic and brain tissues, while as stated the cardiovascular
model does not depend on quantities from the respiratory model. Physiologically, the thoracic
arteries and veins depend on respiration since change of volume in the lungs imposes oscillation of
the external pressure in the tissue surrounding the thoracic arteries and veins. Such oscillations can
be observed in measurements of arterial pressure, even on the finger pressure measurements used
for analysis in this study. However, this slow oscillation is a secondary effect not included in the
present study. Furthermore, when control of the system is included respiration will impact cerebral
vascular resistance and compliance through autoregulation.
Based on the above observations, we decoupled the models. The parameter estimation problem
was solved by first estimating parameters for the cardiovascular model. Using the optimized cardiovascular parameters, systemic, pulmonary and cerebral mean blood flows were computed and
used as inputs to the respiratory model. Finally, respiratory model parameters were estimated. A
solution to the original coupled model was found using the optimized cardiovascular and respiratory
parameter values and this solution was compared with the experimental data. This was done to
ensure that the optimized parameters from the decoupled models could predict the dynamics of the
complete model.
4.4. Least squares cost. As mentioned earlier, model parameters are estimated by minimizing the
least squares error between computed and measured values of arterial pressure, cerebral blood flow
velocity, and left ventricular ejection fraction (for the cardiovascular model) and end tidal partial
CARDIOVASCULAR & RESPIRATORY DYNAMICS IN CONGESTIVE HEART FAILURE
13
pressure of expiratory CO2 for the respiratory model. Similar to previous studies [50, 15] we note
that to accurately predict cardiovascular dynamics it is important to account for changes in systolic
and diastolic values of arterial pressure and cerebral blood flow velocity. For each timeseries, the
data are measured at a fixed frequency (128 Hz); thus the quantities (pressure, velocity, partial
pressure of CO2 ) are observed at N equally spaced times, ti . The timeseries analyzed contain a
given number of cardiac cycles (M ), thus for arterial pressure and cerebral blood flow velocity we
have M observations of systolic and diastolic values. In addition, we have an average value for
ejection fraction (EF). Since the study is done during steady state, we assume that the ejection
fraction should be the same for each of the M cardiac cycles. In summary, we have the following
observations:
• Arterial blood pressure psa (ti ), i = 1 : N [mmHg]
• Cerebral blood flow velocity vc (ti ), i = 1 : N [cm/sec]
• Systolic arterial blood pressure psa,sys,j , j = 1 : M [mmHg]
• Diastolic arterial blood pressure psa,dia,j , j = 1 : M [mmHg]
• Systolic cerebral blood flow velocity vc,sys,j , j = 1 : M [cm/sec]
• Diastolic cerebral blood flow velocity vc,dia,j , j = 1 : M [cm/sec]
• Left ventricular ejection fraction EFj , j = 1 : M = 0.26
• End tidal partial pressure of expiratory CO2 pexp,CO2 (ti ), i = 1 : N [mmHg].
Each of these data vectors has an associated predicted vector, which we denote by a superscript (p).
p
p
The predicted vectors are ppsa , vcp , ppsa,sys , ppsa,dia , vc,sys
, vc,dia
, EF p , and ppexp,CO2 .
Since the parameter estimation problem is solved separately for the cardiovascular and the respiratory models, we define two residual vectors Rcar and Rresp , as
T
Rcar = Rpsa , Rvc , Rpsa,sys , Rpsa,dia , Rva,sys , Rva,dia , REF ,
T
Rresp = Rpexp,CO2 .
where each component is scaled to account for the number of elements in the vector and relative to
the data, i.e.,
T
p
ppi (tN ) − pi (tN )
pi (t1 ) − pi (t1 )
1
,
,··· ,
Ri = √
pi (t1 )
pi (tN )
K
where i = psa , vc , psa,sys , psa,dia , . . . , EF , and K = N, M , respectively.
Thus, the vector Rcar has 2N + 5M entries, while Rresp has N entries. For each of the two
models, the least squares cost J is defined by
J = kRi k22 = RiT Ri ,
i = car, resp.
(14)
Minimizing the cost function is a nonlinear least squares problem. Solutions were found using the
Levenberg-Marquardt variant of the Gauss-Newton optimization method [32]. Before solving the
least squares problem we used sensitivity analysis and subset selection to prune the set of parameters.
4.5. Sensitivity analysis. Sensitivity analysis gives a measure of how much the output of a model
is affected by changes in the model parameters. For the cardiovascular part of the model, sensitivities
were computed for arterial blood pressure, ppsa , cerebral blood flow velocity vcp , and ejection fraction
EF p . For each quantity x, the sensitivity to a parameter θ is a time-varying quantity, given by
θ0
dxi for i = 1, . . . , N.
dθ
xi
θ=θ0
To remove the effects of poorly scaled parameters and output, each component of the derivative is
weighted by the parameter value and the reciprocal of predicted pressure. This gives sensitivities as
dimensionless quantities, allowing them to be compared amongst each other.
14
L.M. ELLWEIN, S.R. POPE, A. XIE, J. J. BATZEL, C.T. KELLEY, M.S. OLUFSEN
To rank parameters from the most to the least sensitive we use a weighted 2-norm to obtain a
sensitivity for each quantity. For the cardiovascular model, we compute sensitivities with respect to
three quantities (psa , vc , and EF), then take the mean over the three quantities, i.e,
√
√
√
Scar,θ = mean{kSppsa ,θ k2 / N, kSvcp ,θ k2 / N kSEF p ,θ k2 / M }.
However, the respiratory model is only validated against one quantity (end tidal partial pressure of
expiratory CO2 , i.e., the sensitivity is given by
√
Sresp,θ = kSpexp,CO2 k2 / N .
If the model is insensitive to a parameter, it should be not be considered during an optimization.
4.6. Subset Selection. Let θ be the vector of P model parameters. Let R be the model residual.
Subset selection looks at the Jacobian, dR/dθ, and attempts to find a subset of columns that are
“maximally independent”. We employ a method from [24] which also appears in [25]. The method
was also used in [50, 15]. The method includes the following steps
• Compute a Jacobian matrix at nominal parameter values, R′ (θ0 ) = dR/dθ|θ=θ0 , with error
estimate ε.
• Find a singular value decomposition of R′ (θ0 ) = U ΣV T with
Σ = diag(σ1 , . . . , σP )
and singular values σ1 ≥ σ2 ≥ · · · ≥ σP .
• Determine the number of columns, k, by counting the number of singular values larger than ε.
• Use QR factorization with column pivoting [25] on VkT where Vk is the matrix consisting of
the first k columns of V . The factorization is
VkT P = QR.
• The first k components of θT P = [θn1 · · · θnP ] should be used in the optimization.
Label the vector of k chosen parameters θk and the vector of remaining parameters θP −k . These steps
ensure that the condition number of the reduced Jacobian, κ(dR/dθk ) = kdR/dθk k2 k(dR/dθk )† k2
remains small, and that dR/dθk does a good job of representing dR/dθP −k [25].
5. Results. We first present results from the sensitivity analysis, then we discuss the subset selection algorithm and present simulation results obtained from the nonlinear least squares optimization.
5.1. Sensitivity analysis. For both the cardiovascular and the respiratory models we computed
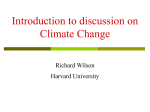
and ranked relative sensitives as described above. Figure 3 shows that both models contain both sensitive and insensitive parameters, but no clear jump separates the two groups. For both models we defined all parameters with a sensitivity greater than 10−2 as sensitive. This choice allows us to include
all parameters that we can account for using physiological arguments. For the cardiovascular model
this leaves 16 parameters including xcar,sens = {Vld ,Emr ,Rc ,Eml ,TM,f rac,Rp ,Csv ,Csa ,Cpv ,EMl ,EMr ,
Rs ,Vrd ,Rca ,Rcv ,Cca }. Note that all heart valve resistances are insensitive. From previous work [50,
15] we know that Ac is correlated with Rc , thus we keep this parameter constant and do not include
this parameter in our list of parameters that we seek to estimate using nonlinear optimization. For
the respiratory model, including parameters with sensitivity larger than 10−2 allows us to pick 6
parameters including xresp,sens = {MCO2 ,VD ,KCO2 ,kCO2 ,VT,CO2 ,VB,CO2 ,MB,CO2 }. Note, we do not
include any data predicting partial pressure of O2 , thus all parameters related to prediction of O2
partial pressures/concentrations are insensitive.
CARDIOVASCULAR & RESPIRATORY DYNAMICS IN CONGESTIVE HEART FAILURE
15
Figure 3. Ranked sensitivities, top graph shows ranking for the cardiovascular model and bottom
graph shows ranking for the respiratory model. For both graphs, blue squares denote sensitivities
computed using the initial (nominal) parameter values, and the red diamonds denote sensitivities
computed using the optimized parameters. Note, that the y-axis is a log scale.
5.2. Subset selection. For each subsystem, we investigated correlation between parameters using
subset selection. For the cardiovascular model, subset selection allowed us to extract five uncorrelated
parameters including xcar,sub = {Rc , Rs , Ca ,TM,f rac, EMl }. It should be noted that these are the
same cardiovascular parameters found to be uncorrelated in our previous studies [50, 15]. Estimation
of these five parameters using nonlinear optimization did not allow us to accurately predict the
observed data. An analysis of the remaining parameters (not picked by subset selection) revealed
that including a sixth parameter Cca allowed us to better predict the data. We remind the reader
that subset selection was based on initial parameter values. We repeated the subset selection with
optimized parameter values, and at this stage Cca was included in the subset. Furthermore, it
should be noted, that if we ran the models using data from a young subject, the same cardiovascular
parameters were identified, but for the young subject it was not necessary to also estimate arterial
cerebral compliance.
Before predicting sensitivities for the respiratory model we used optimized cardiovascular parameters to compute the mean flow in the systemic q s , cerebral q c , and pulmonary q p circulations.
Along with airflow data these flows were used as inputs to the model. These quantities were kept
fixed during the subset selection. Results from subset selection allowed us to estimate 4 parameters including xresp,sub = {KCO2 , kCO2 , MS,CO2 , VD }. It should be noted that none of the selected
parameters were insensitive.
5.3. Nonlinear optimization. For both models parameters were estimated using the LevenbergMarquardt variant of the Gauss-Newton optimization method [32]. Optimized parameters are given
in Table 3. For the cardiovascular model data were subsampled at 64 Hz to speed up simulations,
and computations settled at steady state within the data analyzed. For the respiratory model data
were subsampled at 4.2667 Hz to speed up simulations, furthermore to ensure that steady state was
reached respiratory data were repeated 40 times. The comparison used to compute the least squares
error were done over the last repeat of the data. Results of optimizations are shown in Figures 4
16
L.M. ELLWEIN, S.R. POPE, A. XIE, J. J. BATZEL, C.T. KELLEY, M.S. OLUFSEN
Table 3. Optimized model parameters, note the value for TM,f rac is the fraction relative to the
length of the cardiac cycle. Averaged model quantities include ejection fraction, cardiac output,
mean heart rate, as well as systemic, cerebral, and pulmonary flow.
Parameter
Rs
Rc
Csa
Cca
EM l
TM,f rac
EF
CO
HR
qs
qc
qp
KCO2
kCO2
MS,CO2
VD
Description
Systemic resistance
Cerebral resistance
Systemic arterial compliance
Cerebral arterial compliance
Maximum left ventricular elastance
Time for maximum ventricular elastance
Ejection fraction
Cardiac output
mean heart rate
Mean systemic flow
Mean cerebral flow
Mean pulmonary flow
Dissociation constant
Dissociation constant
Metabolic rate systemic tissue
Total deadspace volume
Optimized
1.28
2.54
0.536
2.96
0.721
0.139
0.262
4.92
62.5
55.0
26.9
82.0
0.00688
0.261
4.20
151
Unit
mmHg sec/ml
mmHg sec/ml
mmHg/ml
mmHg/ml
ml/mmHg
l/min
beats/min
ml/sec
ml/sec
ml/sec
mlST P D mmHg/ml
mlST P D mmHg/ml
mlST P D mmHg/sec
ml
and 5. The cardiovascular model used heart rate as an input, and the respiratory model used airflow
and mean blood flows computed from the cardiovascular model with optimized parameters.
6. Discussion. Results from the cardiovascular and respiratory models (Figures 4, 5, and 6) showed
that the modular model approach used in this study enable prediction of both cardiovascular and
respiratory quantities. Results from the coupled model were indistinguishable from the results
obtained with each of the two models indicating that using mean values for flows do not impact the
respiratory model significantly, which is to be expected since respiration occurs over a much slower
timescale as the cardiovascular oscillations.
In addition to estimating observed quantities, we also computed all internal states and most
of these were within physiological bounds as discussed below. It should be noted that techniques
used for parameter estimation do not guarantee that internal states cannot fluctuate away from
physiological values, even though initial parameter estimates were within physiological bounds. This
is one of the main problems with the proposed method. Besides including bounds on all model
parameters, we did not impose additional constraints limiting the states within certain bounds.
Consequently some states did drift away from expected values.
In regards to cardiovascular characteristics as reflected by the model for this subject with CHF,
we note that approximately 30% of cardiac output was utilized as cerebral blood flow. This is
large, however, cerebral blood flow velocity measured for this subject was significantly larger than
mean velocities reported in the literature [28]. This could be due to poor circulation in the body
or exceptionally high values from the transcranial Doppler measurements. This subject exhibits
a severely enlarged left ventricle (consistent with left ventricular failure) and reduced pumping
effectiveness, with an ejection fraction of 26%. Neverless, the cardiac output (modeled) is close to
normal. This type of behavior is seen in approximately half the patients suffering from CHF [43].
With optimized parameters the maximum left ventricular volume was approximately 317 ml,
which is close to initial volume chosen as 312 ml. The minimum ventricular volume was approximately 238 ml, yielding a stroke volume of 79 ml and with the mean heart rate of 62.5 beats/min
this gives an approximate CO of 4.9 computed from the flows in the model (see Table 3). Systemic
venous pressures were approximately 7.2 mmHg somewhat higher than normal, which is expected
for a patient with CHF (see Table 4). Pulmonary arterial pressures were approximately 23 mmHg
CARDIOVASCULAR & RESPIRATORY DYNAMICS IN CONGESTIVE HEART FAILURE
100
80
100
vc [cm/sec]
100
Data
Model
80
60
40
0
50
100
time [sec]
150
psa [mmHg]
120
Data
Model
100
80
60
150
152
154
156
158
vc [cm/sec]
100
80
60
40
150
152
154
156
time [sec]
0.32
0.28
0.27
Data
Model
80
50
100
time [sec]
150
Data
Model
100
80
152
154
156
158
160
Data
Model
100
90
80
152
154
156
time [sec]
0.28
158
160
Model
Data
0.275
0.27
0.265
0.26
0.255
0.26
0.25
150
90
150
Ejection Fraction (EF)
0.29
100
100
60
150
160
0.3
50
120
Model
Data
0.31
Ejection Fraction (EF)
158
80
0
160
Data
Model
Data
Model
100
60
0
150
vc [cm/sec]
50
psa [mmHg]
60
0
120
psa [mmHg]
Data
Model
vc [cm/sec]
psa [mmHg]
120
17
50
100
Heartbeat
150
0.25
50
100
Heartbeat
150
Figure 4. Simulation results cardiovascular model. Top panel shows arterial pressure and cerebral
blood flow velocity for the full dataset, second panel shows a zoom for 150 ≤ t ≤ 160 seconds.
Bottom panel shows computed and expected ejection fraction (set at 26%). Left graphs give results
with initial (nominal) parameter values, while the right graphs show results with the optimized
values.
18
L.M. ELLWEIN, S.R. POPE, A. XIE, J. J. BATZEL, C.T. KELLEY, M.S. OLUFSEN
35
35
30
30
pexp,CO2 [mmHg]
40
pexp,CO2 [mmHg]
40
25
25
20
20
15
15
10
10
5
5
0
0
50
100
time [sec]
0
0
150
35
35
30
30
25
150
25
20
20
15
15
10
10
5
5
0
100
100
time [sec]
pexp,CO2 [mmHg]
40
pexp,CO2 [mmHg]
40
50
110
120
130
time [sec]
140
150
0
100
110
120
130
time [sec]
140
150
Figure 5. Estimation of respiratory parameters minimizing difference between measured and computed values of partial pressure of CO2 . Left graphs show computations with initial parameters and
right graphs show results with optimized parameters.
arterial
exp
40
35
pCO2 [mmHg]
30
25
20
15
10
5
0
100
110
120
130
time [sec]
140
150
Figure 6. Model simulation of psa,CO2 and pexp,CO2 showing relation between these quantities
during inhalation and exhalation
CARDIOVASCULAR & RESPIRATORY DYNAMICS IN CONGESTIVE HEART FAILURE
19
and pulmonary venous pressures were approximately 5.5 mmHg. This is also to be expected for a
patient with left ventricular CHF (see Table 4). Heart rate (not modeled) was within normal range.
For this model both cerebral and systemic vascular resistance and compliance were kept constant.
The total resistance RT = (1/RB + 1/Rs ) = 0.86, where RB = Rca + Rc + Rcv is fairly low, again
this is to be expected in CHF where CO is lower than normal, and for this subject in particular,
where a large quantity of the blood goes to the brain. Moreover, the somewhat large proportion of
flow to the brain could also be a result of the somewhat simplified modeling included for the cerebral
arteries. The blood flow velocity measured is from the middle cerebral arteries, this has then been
scaled (assuming constant area of the major cerebral arteries) to compute a total flow to the brain.
Without information about anatomical quantities for the size of the cerebral arteries, this scaling
factor cannot be computed accurately, and the magnitude of the scaling factor Ac would impact the
optimized values for the cerebrovascular resistance Rc since these two parameters are correlated as
stated earlier. However, if e.g., the area of all major cerebral vessels (PCA, MCA and ACA) were
measured e.g., with an angiogram, then this scaling parameter could be computed from data.
For the respiratory quantities values for dead space pD,CO2 and pD,O2 , arterial values pa,CO2
and pa,O2 , and systemic values pS,CO2 and pS,O2 (calculated from dissociation laws) are reasonable.
Dynamics of pA,CO2 (equivalent with pa,CO2 ) are shown in Figures 5 and 6. Dead space values
for CO2 oscillate between zero (inhaled air) and end-expiratory air approximately the same as
alveolar air. Oxygen values follow similar reasonable patterns. It should be noted that brain partial
pressures pB,CO2 and pB,O2 did not match typical values so well in the optimized case. Estimates
of the dissociation constants varied from the initial guesses which resulted in pB,CO2 approximately
43 mmHg (too low) and pB,O2 approximately 48 mmHg (too high). There are likely several reasons
for this. Firstly, the data for cerebral blood velocity for this subject was rather high, which would
tend to depress brain pB,CO2 and raise pB,O2 . Secondly, we did not have data on O2 which might
impact the results. Further, research indicates that normal cerebral metabolism is distorted in CHF
and cerebral energy deficits can exist in certain cerebral tissue [35]. This complicates the picture for
the estimation process.
These observations lead us to conclude that the proposed methodology and model can be used for
quantitative prediction of changes within several subjects with CHF. To use this model to compare
quantities from a larger population it should be emphasized that the model should be used with care.
It is important that nominal parameters reflect known characteristics from a subject with CHF, in
particular since only a subset of the parameters will be estimated. Conclusions based on analysis of
parameters obtained from several subjects should all be interpreted related to the nominal parameter
values used. Furthermore, additional measurements that would increase predictability of the model
parameters include measurements of cardiac output and estimation of diameters of major cerebral
vessels. Knowing these quantities would allow better prediction of systemic and arterial flow as
well as help to get better estimation of the scaling factor needed, which would help in prediction of
the scaling factor relating MCA CBFV to CBF. Furthermore, if constants used in dissociation laws
(optimized with our respiratory model) are fixed, subset selection allows estimation of the tissue and
brain CO2 metabolic rates as well as the deadspace volume. The parameter values for deadspace
volume were identical to simulation reported here, while parameters for tissue metabolic rate went
down slightly (from 4.20 to 4.16) and the parameter for brain CO2 metabolic rate was reduced
from its initial value (from 1.04 to 0.87). Furthermore, simulations with this set of parameters
leads to similar dynamics that were observed in results presented above. Again, it should be noted
that it is essential that caution is used when choosing parameters fed to the subset selection. Subset
selection will give a subset of uncorrelated parameters that can be estimated given particular nominal
parameter values and initial conditions for the differential equations.
20
L.M. ELLWEIN, S.R. POPE, A. XIE, J. J. BATZEL, C.T. KELLEY, M.S. OLUFSEN
Table 4. Generic state changes in left systolic CHF.
State
Mean pap [mmHg]
Mean pvp [mmHg]
Mean pas [mmHg]
Mean pvs [mmHg]
Mean plv [mmHg]
Mean pla [mmHg]
LVEDP [mmHg]
LVESP [mmHg]
LVEDV [ml]
LVESV [ml]
LVEF [ml]
CO [mlmin]
SV [ml]
HR [beat/min]
Systemic resistance [mmHg · s /ml]
Fluid retention [ml]
Value
increase
increase
decrease or stable
increase
steady to increase
increase
increase
steady or increase
increase
increase
decrease
decrease
decrease
increase
increase
increase
Source
[44]
[40, 31]
[49]
[31]
[41]
[49]
[41]
[41]
[10, 49]
[10, 49]
[10, 20]
[49]
[49]
[49, 20]
[31]
[31, 19]
Acknowledgments. Olufsen and Ellwein were partially supported by National Science Foundation under grant DMS-0616597 and OISE-524249, Batzel was suported in part by FWF (Austrian
Research Funds) project P18778-N13, Pope and Kelley was supported in part by National Science
Foundation under grant DMS-0707220, and Xie was supported in part by the American Lung Association of Wisconsin.
Appendix.
6.1. Cardiovascular model. Blood pressures, ventricular volumes, and intrathoracic pressure.
dppa
dt
dppv
dt
dpsa
dt
dpsv
dt
dpca
dt
dpcv
dt
dVlv
dt
dVrv
dt
=
=
=
=
=
=
=
=
ppa − ppv
prv − ppa
/Cpa
−
Rpv
Rp
ppv − plv
ppa − ppv
/Cpv
−
Rp
Rmv
psa − psv
psa − pca
plv − psa
/Csa
−
−
Rav
Rs
Rca
pcv − psv
psv − prv
psa − psv
/Csv
+
−
Rs
Rcv
Rtv
psa − pca
pca − pcv
−
/Cca
Rca
Rc
pcv − psv
pca − pcv
/Ccv
−
Rc
Rcv
plv − psa
ppv − plv
−
Rmv
Rav
prv − ppa
psv − prv
−
.
Rtv
Rpv
CARDIOVASCULAR & RESPIRATORY DYNAMICS IN CONGESTIVE HEART FAILURE
21
Table 5. Initial values for the cardiovascular model. Note initial values for the cardiovascular
system are set using the corresponding nominal parameter values given in Table 1.
Variable
ppa [mmHg]
ppv [mmHg]
pdsa [mmHg]
psv [mmHg]
pca [mmHg]
pcv [mmHg]
Physiologic description
Pulmonary arterial pressure
Pulmonary venous pressure
Systemic arterial pressure
Systemic venous pressure
Cerebral arterial pressure
Cerebral venous pressure
Value
20
3.3
pdsa
6.6
psa · 0.99
7
Reference
[8, 29]
[8, 29]
measured
[8, 29]
measured
[8, 29]
Vlv [ml]
Vrv [ml]
Left ventricular volume
Right ventricular volume
EDVlv = 312
EDVrv = 100
[59]
[8, 29]
Note the airflow V̇IE is defined below. Heart valves
Rav
Rmv
Rpv
Rtv
i
h
= min Rav,o + e−2(plv −psa ) , Rav,c
i
h
= min Rmv,o + e−2(ppv −plv ) , Rmv,c
h
i
= min Rpv,o + e−2(prv −ppa ) , Rpv,c
i
h
= min Rtv,o + e−2(psv −prv ) , Rtv,c .
Ventricular pressures
plv (t) =
prv (t) =
Elv (t)[Vlv (t) − Vld ]
Erv (t)[Vrv (t) − Vrd ].
where
Elv (t) =
Erv (t) =
πt
Eml + (EMl − Eml ) 1 − cos
/2
TM
π(t − TM )
+ 1 /2
Eml + (EMl − Eml ) cos
TR
Eml
πt
/2
E
+
(E
−
E
)
1
−
cos
mr
Mr
mr
TM
π(t − TM )
+
1
/2
E
+
(E
−
E
)
cos
mr
Mr
mr
TR
Emr
0 ≤ t ≤ TM
TM ≤ t ≤ TM + TR
TM + TR ≤ t ≤ T,
0 ≤ t ≤ TM
TM ≤ t ≤ TM + TR
TM + TR ≤ t ≤ T.
Note, the timing parameters TM and TR are the same for both the left and right ventricles. Input
to this model is heart rate HR. Output from the model is arterial blood pressure psa (t) and cerebral
blood flow velocity vc = (pca − pcv )/Rc . Initial values for these differential equations are listed in
Table 5 (below), while nominal values for all model parameters are listed in Table 1 and optimized
values for estimated parameters are given in Table 3.
22
L.M. ELLWEIN, S.R. POPE, A. XIE, J. J. BATZEL, C.T. KELLEY, M.S. OLUFSEN
6.2. Respiratory model.
dcS,CO2
dt
dcS,O2
dt
dcB,CO2
dt
dcB,O2
dt
=
MS,CO2 + qs (ca,CO2 − cS,CO2 )/VS,CO2
=
−MS,O2 + qs (ca,O2 − cS,O2 )/VS,O2
=
MB,CO2 + qc (ca,CO2 − cB,CO2 )/VB,CO2
=
−MB,O2 + qc (ca,O2 − cB,O2 )/VB,O2 .
Inspiration
dpD1,CO2
dt
dpD1,O2
dt
dpD2,CO2
dt
dpD2,O2
dt
dpD3,CO2
dt
dpD3,O2
dt
dpa,CO2
dt
dpa,O2
dt
= V̇ie (pi,CO2 − pD1,CO2 )/VD1
= V̇ie (pi,O2 − pD1,O2 )/VD1
= V̇ie (pD1,CO2 − pD2,CO2 )/VD2
= V̇ie (pD1,O2 − pD2,O2 )/VD2
= V̇ie (pD2,CO2 − pD3,CO2 )/VD3
= V̇ie (pD2,O2 − pD3,O2 )/VD3
= 863 · 0.98 · qp (cv,CO2 − ca,CO2 ) + V̇ie (pD3,CO2 − pa,CO2 )/VA
= 863 · 0.98 · qp (cv,O2 − ca,O2 ) + V̇ie (pD3,O2 − pa,O2 )/VA .
Expiration
dpD1,CO2
= V̇ie (pD1,CO2 − pD2,CO2 )/VD1
dt
dpD1,O2
= V̇ie (pD1,O2 − pD2,O2 )/VD1
dt
dpD2,CO2
= V̇ie (pD2,CO2 − pD3,CO2 )/VD2
dt
dpD2,O2
= V̇ie (pD2,O2 − pD3,O2 )/VD2
dt
dpD3,CO2
= V̇ie (pD3,CO2 − pa,CO2 )/VD3
dt
dpD3,O2
= V̇ie (pD3,O2 − pa,O2 )/VD3
dt
dpa,CO2
= 863 · 0.98 · qp (cv,CO2 − ca,CO2 )/VA
dt
dpa,O2
= 863 · 0.98 · qp (cv,O2 − ca,O2 )/VA .
dt
Note, instantaneous airflow is obtained from integrating the air flow velocity data as described in
equation (13).
Inputs to the stand alone respiratory model are airflow velocity, average systemic, pulmonary, and
cerebral blood flow obtained by solving the cardiovascular model. For the coupled model, these flows
CARDIOVASCULAR & RESPIRATORY DYNAMICS IN CONGESTIVE HEART FAILURE
23
are computed at any instant in time. Initial values for the respiratory model are given in Table 6,
while nominal parameters for all respiratory parameters are listed in Table 2, and optimized values
for estimated parameters are given in Table 3.
Table 6. Initial values for the respiratory model.
Variable
pD1,CO2 [mmHg]
pD1,O2 [mmHg]
pD2,CO2 [mmHg]
pD2,O2 [mmHg]
pD3,CO2 [mmHg]
pD3,O2 [mmHg]
pa,CO2 [mmHg]
pa,O2 [mmHg]
cS,CO2 [mlSTPD /ml]
cS,O2 [mlSTPD /ml]
cB,CO2 [mlSTPD /ml]
cB,O2 [mlSTPD /ml]
Physiologic description
CO2 partial pressure lung deadspace 1
O2 partial pressure lung deadspace 1
CO2 partial pressure lung deadspace 2
O2 partial pressure lung deadspace 2
CO2 partial pressure lung deadspace 3
O2 partial pressure lung deadspace 3
Systemic arterial CO2 partial pressure
Systemic arterial O2 partial pressure
Systemic tissue CO2 concentration
Systemic tissue O2 concentration
Cerebral tissue CO2 concentration
Cerebral tissue O2 concentration
Value
5
159
6
158
7
157
40
100
0.543
0.128
0.569
0.112
Reference
[27, 33]
[27, 33]
[27, 33]
[27, 33]
[27, 33]
[27, 33]
[58]
[18]
[18]
[18]
[27, 33]
[27, 33]
REFERENCES
[1] P.N. Ainslie, J.C. Ashmead, K. Ide, B.J. Morgan, and M. J. Poulin, Differential responses to CO2 and sympathetic
stimulation in the cerebral and femoral circulations in humans, J Physiol, 566 (2005), 613–624.
[2] S. F. Ameriso, J. G. Mohler, M. Suarez, and M. Fisher, Morning reduction of cerebral vasomotor reactivity,
Nerology, 44 (1994), 1907–1909.
[3] R. J. Baker, D. D. Kozoll, and K. A. Meyer, The use of surface area as a basis for establishing normal blood
volume, Surg Gynecol Obstet, 104 (1957), 183–189.
[4] J. J. Batzel, F. Kappel, and S. Timischl-Teschl, A cardiovascular-respiratory control system model including
state delay with application to congestive heart failure in humans, J Math Biol, 50 (2005), 293-335.
[5] S. J. Bennett, M. J. Sauvë, and R. M. Shaw, A conceptual model of cognitive deficits in chronic heart failure, J
Nurs Scholarsh, 37 (2005), 222–228.
[6] J. Beneken and B. DeWitt, A physical approach to hemodynamic aspects of the human cardiovascular system,
in “Physical Bases of Circulatory Transport: Regulation and Exchange” (eds. E. Reeve and A. Guyton), W. B.
Saunders, Philadelphia, PA, 1967, 1–45.
[7] R. M. Berne and M. N. Levy, Physiology, C. V. Mosby Company, Second edition, 1988.
[8] W. Boron and E. Boulpaep, Medical Physiology, W. B. Saunders, Philadelphia, PA, 2003.
[9] S. N. Caparas, M.J Clair, R. S. Krombach, J. W. Hendrick, W. V. Houck, S. B. Kribbs, R. Mukherjee, G. E.
Tempel, F. G. Spinale, Brain blood flow patterns after the development of congestive heart failure: effects of
treadmill exercise, Crit Care Med, 28 (2000), 209–214.
[10] K. Chatterjee and B. Massie. Systolic and diastolic heart failure: differences and similarities, J Card Fail, 13
(2007), 569–576.
[11] X. Chen, L. Qi, and K-L. Teo, Smooth convex approximation to the maximum eigenvalue function, J Global Opt,
30 (2004), 253–270.
[12] N. S. Cherniack, Apnea and periodic breathing during sleep, New England J Med, 341 (1999), 985–987.
[13] F. Dong and W. F. Langford, Models of Cheyne-Stokes respiration with cardiovascular pathologies, J Math Biol,
57 (2008), 497–519.
[14] L. Ellwein, H. T. Tran, C. Zapata, V. Novak, and M. S. Olufsen, Sensitivity analysis and model assessment:
mathematical models for arterial blood flow and blood pressure, J Cardiovasc Eng, 8 (2008), 94–108.
[15] L. M. Ellwein, Cardiovascular and respiratory regulation, modeling and parameter estimation, Ph.D. Thesis,
Applied Mathematics, North Carolina State University, Raleigh, NC, 2008.
[16] G. E. Foster, M. J. Poulin, and P. J. Hanly, Intermittent hypoxia and vascular function: implications for obstructive sleep apnea, Exp Physiol, 92 (2007), 51–65.
[17] S. Javaheri, T. J. Parker, J. D. Liming, W. S. Corbett, H. Nishiyama, L. Wexler, G. A. Roselle, Sleep apnea in 81
ambulatory male patients with stable heart failure. Types and their prevalences, consequences, and presentations,
Circulation, 97 (1998), 2154–2159, 1998.
[18] S. I. Fox, Human Physiology, Wm C Brown Publishers, Dubuque, IA, 1993.
24
L.M. ELLWEIN, S.R. POPE, A. XIE, J. J. BATZEL, C.T. KELLEY, M.S. OLUFSEN
[19] G. S. Francis. Pathophysiology of chronic heart failure, Am J Med, 110 (2001), 37S–46S.
[20] N. Fukuda, H. Shinohara, K. Sakabe, S. Morishita, Y. Fukuda, and Y. Tamura, Evaluation of right ventricular
function in patients with congestive left heart failure by the Doppler derived total cardiac performance index (tei
index), J Echocard, 5 (2007), 11–17.
[21] A. Garcia-Touchard, V. K. Somers, L. J. Olson, and S. M. Caples, Central sleep apnea: implications for congestive
heart failure, Chest, 133 (2008), 1495–1504.
[22] D. Georgiadis, M. Sievert, S. Cencetti Cerebrovascular reactivity is impaired in patients with cardiac failure, Eur
Heart J, 21 (2000), 407–413.
[23] J. M. Golbin, V. K. Somers, and S. M. Caples, Obstructive Sleep Apnea, cardiovascular disease, and pulmonary
hypertension, Proc Am Thorac Soc, 5 (2008), 200–206.
[24] G. H. Golub, V. Klema, and G. W. Stewart, Rank Degeneracy and the Least Squares Problem, Technical Report
TR-456, Department of Computer Science, University of Maryland, College Park, MD, 1976.
[25] G. Golub and C. Van Loan, Matrix Computations, The Johns Hopkins Univ Press, Baltimore, MD, 1989.
[26] R. Gopinathannair, A. Mazur, and B. Olshansky, Syncope in congestive heart failure, J Cardiol, 15 (2008),
303–312.
[27] F. S. Grodins, J. Buell, and A. J. Bart, Mathematical analysis and digital simulation of the respiratory control
system, J Appl Physiol, 22 (1967), 260–276.
[28] N. Gruhn, F. S. Larsen, S. Boesgaard, G. M. Knudsen, S. A. Mortensen, G. Thomsen, J. Aldershvile. Cerebral
blood flow in patients with chronic heart failure before and after heart transplantation, Stroke, 32 (2001), 2530–
2533.
[29] A. Guyton and J. Hall, Textbook of Medical Physiology, W. B. Saunders, Philadelphia, PA, 1996.
[30] T. Heldt, Computational Models of Cardiovascular Response to Orthostatic Stress, Ph.D. Thesis, Harvard/MIT
Division of Health Science and Technology, MIT, 2004.
[31] A. M. Katz, Heart failure: a hemodynamic disorder complicated by maladaptive proliferative responses, J Cell
Mol Med, 7 (2003), 1–10.
[32] C. T. Kelley, Iterative methods for optimization, SIAM, Philadelphia, PA, 1999.
[33] M. C. K. Khoo, A model-based evaluation of the single breath CO2 test, J Appl Physiol, 68 (1990), 393–399.
[34] M. C. K. Khoo, A. Gottschalk, and A. I. Pack, Sleep-induced periodic breathing and apnea: A theoretical study,
J Appl Physiol, 70 (1991), 2014–2024.
[35] C. W. Lee, J. H. Lee, J. J. Kim, S. W. Park, M. K. Hong, S. T. Kim, T. H. Lim, and S. J. Park, Cerebral
metabolic abnormalities in congestive heart failure detected by proton magnetic resonance spectroscopy, J Am
Coll Cardiol, 33 (1999), 1196 –1202.
[36] C. W. Lee, J. H. Lee, T. H. Lim, H. S. Yang, M. K. Hong, J. K. Song, S. W. Park, S. J. Park, J. J. Kim,
Prognostic significance of cerebral metabolic abnormalities in patients with congestive heart failure, Circulation,
103 (2001), 2784–2787.
[37] G. S. Longobardo, N. S. Cherniack, and B. Gothe, Factors affecting respiratory system stability, Ann Biomed
Eng, 17 (1989), 377–396.
[38] K. Lu, J. Clark, F. Ghorbel, D. Ware, and A. Bidani, A human cardiopulmonary system model applied to the
analysis of the Valsalva maneuver, Am J Physiol, 281 (2001), H2661–H2679.
[39] K. Lu, W. Clark, F. H. Ghorbel, C. S. Robertson, D. L. Ware, J. B. Zwischenberger, and A. Bidani, Cerebral
autoregulation and gas exchange studied using a human cardiopulmonary model, Am J Physiol Heart Circ Physiol,
286 (2004), 584–601.
[40] S. Magder, S. Veerassamy, and J. H. Bates. A further analysis of why pulmonary venous pressure rises after the
onset of lv dysfunction, J Appl Physiol, online first Oct. 9, 2008.
[41] S. Mak, E. R. Azevedo, P. P. Liu, and G. E. Newton. Effect of hyperoxia on left ventricular function and filling
pressures in patients with and without congestive heart failure, Chest, 120 (2001), 467–473.
[42] R. Mosteller, Simplified calculation of body surface area, N Engl J Med, 317 (1987), 1098.
[43] J. O. Mudd and D. A. Kass. Tackling heart failure in the twenty-first century, Nature, 451 (2008), 919–928.
[44] K. M. O’Dell, J. S. Kalus, S. Kucukarslan, and B. Czerska. Nesiritide for secondary pulmonary hypertension in
patients with end-stage heart failure, Am J Health Syst Pharm, 62 (2005), 606–609.
[45] M. S. Olufsen, J. T. Ottesen, H. T. Tran, L. M. Ellwein, L. A. Lipsitz and V. Novak. Blood pressure and blood flow
variation during postural change from sitting to standing: model development and validation, J Appl Physiol, 99
(2005), 1523–1537.
[46] S. M. Otis and E. B. Ringelstein, The transcranial Doppler examination: principles and applications of transcranial Doppler sonography, in Neurosonology, by C. H. Tegeler, V. L. Babikian, and C. R. Gomez (eds), Mosby,
St. Louis, MO,
[47] J. T. Ottesen and M. Danielsen, Modeling ventricular contraction with heart rate changes, J Theo Biol, 22 (2003),
337–346.
CARDIOVASCULAR & RESPIRATORY DYNAMICS IN CONGESTIVE HEART FAILURE
25
[48] J. T. Ottesen, M. S. Olufsen and J. Larsen, Applied Mathematical Models in Human Physiology, SIAM, Philadelphia, PA, 2004.
[49] W. W. Parmley. Pathophysiology of congestive heart failure, Clin Cardiol, 15 (Suppl) (1992), I5–I12.
[50] S. R. Pope, L. M. Ellwein, C. L. Zapata, V. Novak, C. T. Kelley, M. S. Olufsen, Estimation and identification of
parameters in a lumped cerebrovascular model, Math Biosci Eng, 6 (2009).
[51] V. Rideout Mathematical and computer modeling of physiological systems, Prentice Hall, Englewood Cliffs, NJ,
1991.
[52] G. S. Schroff, J. S. Janicki, and K. T. Weber, Left ventricular systolic dynamics in terms of its chamber mechanical
properties, Am J Physiol Heart Circ Physiol, 14 (1983), H110–H124.
[53] D. D. Sin, F. Fitzgerald, J. D. Parker, G. Newton, J.S. Floras, T.D Bradley, Risk factors for central and
obstructive sleep apnea in 450 men and women with congestive heart failure, Am J Respir Crit Care Med, 160
(1999), 1077-1078.
[54] P. Solin, T. Roebuck, D. P.Johns, E.H. Walters, M.T. Naughton, Peripheral and central ventilatory responses
in central sleep apnea with and without congestive heart failure, Am J Respir Crit Care Med, 162 (2000), ;
162(6):2194-2200.
[55] N. Stergiopoulos, J. Meister, and N. Westerhof, Determinants of stroke volume and systolic and diastolic aortic
pressure, Am J Physiol, 270 (1996), H2050–H2059.
[56] J. Stocks and P. H. Quanjer, Reference values for residual volume, functional residual capacity and total lung
capacity, J Biomech Eng, 124 (2002), 9–20.
[57] S. Y. Sun, W. Wang, I. H. Zucker, H. D. Schultz, Enhanced peripheral chemoreflex function in conscious rabbits
with pacing-induced heart failure, J Appl Physiol, 86 (1999), 1264–1272.
[58] V. Thomas, F. Costes, T. Busso, Estimation of arterial PCO2 from a lung model during ramp exercise in healthy
young subjects, Resp Physiol Neurobiol, 156 (2007), 259–265.
[59] R. Tkacova, M. J. Hall, P. P. Liu, F. S. Fitzgerald, and T. D. Bradley, Left ventricular volume in patients with
heart failure and cheyne-stokes respiration during sleep, Am J Respir Crit Care Med, 156 (1997), 1549–1555.
[60] M. Ursino Interaction between carotid baroregulation and the pulsating heart: a mathematical model, Am J
Physiol, 44 (1998), H1733–H1747.
[61] G. B. West, J. H. Brown, and B. J. Enquist, A general model for the origin of allometric scaling laws in biology,
Science, 276 (1997), 122–126.
[62] C. R. White and R. S. Seymour, Allometric scaling of mammalian metabolism, J Exp Biol, 208 (2008), 1611–1619.
[63] A. Xie, J. B. Skatrud, R. Khayat, J. Dempsey, B. Morgan, and D. Russell, Cerebrovascular response to carbon
dioxide in patients with congestive heart failure, Am J Resp Crit Care Med, 172 (2005), 371–378.
[64] A. Xie, J. V. Skatrud, B. Morgan, B. Chenuel, R. Khayat, K. Reichmuth, J. Lin, J. A. Dempsey, Influence of
cerebrovascular function on the hypercapnic ventilatory response in healthy humans, J Physiol, 577 (Pt 1) (2006),
319–29.