Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
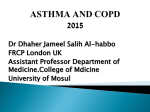
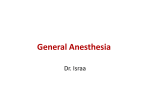
Severe status asthmaticus: Management with permissive hypercapnia and inhalation anesthesia Gökhan M. Mutlu, MD; Phillip Factor, DO, FCCP; David E. Schwartz, MD, FCCP; Jacob I. Sznajder, MD, FCCP Objective: To describe the difficulties that can be encountered during mechanical ventilation of severe status asthmaticus and to discuss the safety of permissive hypercapnia as a ventilatory strategy and the role and limitations of inhalation anesthesia in the treatment of refractory cases. Design: Case series and review of literature. Setting: Intensive care unit of a tertiary care hospital. Patients: Two patients with severe status asthmaticus. Interventions: Administration of inhalational anesthetics. Measurements and Main Results: Both patients had respiratory failure secondary to status asthmaticus requiring mechanical ventilation and permissive hypercapnia. They also received inhalational anesthetics because of refractory bronchoconstriction. Levels of PaCO2 in each case were among the highest and most prolonged elevations (>150 mm Hg for several hours) reported to M anagement of status asthmaticus includes the administration of bronchodilators, corticosteroids, and, in very severe, refractory cases, mechanical ventilation. Concerns that the risks of high end-inspiratory pressures and attendant barotrauma and volutrauma exceed the benefits of normalization of arterial blood gases have shifted the aim of therapy from normalizing arterial blood gases to protecting the lungs and tolerating elevated levels of arterial CO2. This “permissive hypercapnia” has increasingly been accepted as a strategy to prevent complications associated with severely elevated lung volumes and From Pulmonary and Critical Care Medicine, Evanston Northwestern Healthcare, Evanston, IL (GMM, PF); Pulmonary and Critical Care Medicine, Northwestern University Medical School, Chicago, IL (GMM, PF, JIS); and the Department of Anesthesiology, University of Illinois at Chicago, and Michael Reese Hospital, Chicago, IL (DES). Address request for reprints to: Jacob I. Sznajder, MD, Division of Pulmonary and Critical Care Medicine, Northwestern University, 300 East Superior, Tarry 14-707, Chicago, IL 60611. E-mail: [email protected] Copyright © 2002 by Lippincott Williams & Wilkins Crit Care Med 2002 Vol. 30, No. 2 date. In one case, life-threatening difficulties with ventilation were encountered related to the use of an anesthesia ventilator. Although they had complications related to the severity of their illnesses, both were treated to recovery. Conclusions: Mechanical ventilation in severe status asthmaticus can be challenging. Permissive hypercapnia is a relatively safe strategy in the ventilatory management of asthma. High levels of hypercapnia and associated severe acidosis are well tolerated in the absence of contraindications (i.e., preexisting intracranial hypertension). Inhalation anesthesia may be useful in the treatment of refractory cases of asthma but should be used carefully because it may be hazardous owing to poor flow capabilities of most anesthesia ventilators. (Crit Care Med 2002; 30:477–480) KEY WORDS: status asthmaticus; mechanical ventilation; complications; inhalational anesthetics; permissive hypercapnia dynamic hyperinflation (1). Although it is widely practiced, there is no consensus on the level of hypercapnia that is considered safe. “How permissive can we be?” remains an unanswered question. We report two patients with severe status asthmaticus treated with mechanical ventilation and permissive hypercapnia, who also received inhalational anesthetics. Each case is among the highest and most prolonged elevations in PaCO2 in the literature. Both patients had significant complications but were treated to complete recovery. Difficulties during mechanical ventilation, permissive hypercapnia, and the use of anesthesia ventilators to deliver inhalational anesthetics can be a challenge to the treatment of very severe asthma. CASE 1 A 24-yr-old woman with a history of mild, persistent asthma came to the emergency department with complaints of shortness of breath and wheezing of 1 day’s duration. She had never been hospitalized for asthma and had been treated only with albuterol. In the emergency department, she was noted to be in severe respiratory distress and was orotracheally intubated. She subsequently received intravenous corticosteroids and albuterol via continuous nebulization. Because of severe bronchoconstriction and high peak airway pressures, she was sedated with midazolam, paralyzed with vecuronium, and admitted to the intensive care unit (ICU). Physical exam upon arrival to the ICU revealed limited air movement and subcutaneous emphysema around the neck and upper chest. Initial ventilator settings on a Puritan-Bennett 7200 ventilator (Mallinckrodt, Hazelwood, MO) were assist-control, rate of 12/minute, tidal volume of 500 mL (8 mL/kg of total body weight), and positive end-expiratory pressure (PEEP) of 5 cm H2O. The peak inspiratory flow was 80 L/min, FIO2 was 1.0, and peak (Ppeak) and plateau pressures (Pplat) were 94 and 40 cm H2O respectively. Intrinsic PEEP (PEEPi) was 20 cm H2O. An arterial blood gas (ABG) showed pH 7.21, PaCO2 54 mm Hg, and PaO2 442 mm Hg. Laboratory data including chemistry and complete blood count were all within normal limits. Urine drug-of-abuse screen was negative. Chest radiography demonstrated bilateral hyperinflated lungs, subcutaneous emphy477 sema, and pneumomediastinum. To decrease the inspiratory:expiratory ratio, the inspiratory flow rate was gradually increased to 120 L/min and tidal volume was decreased to 400 mL, which resulted in a Ppeak 100 cm H2O, and Pplat 34 cm H2O. Subsequent ABGs demonstrated worsening of acute respiratory acidosis (pH 6.99, PaCO2 120 mm Hg, and PaO2 93 mm Hg with an FIO2 of 0.6). Aminophylline and sodium bicarbonate infusions were started. High PEEPi (20 cm H2O) induced transient mild hypotension and prompted decreasing the respiratory rate to 7 breaths/min, which reduced PEEPi to 14 cm H2O and increased systolic blood pressure to 100 –110 mm Hg. Repeated ABGs following these changes showed PaCO2 oscillating between 180 and 185 mm Hg for 4 hrs, as demonstrated in Figure 1. Lack of improvement in PaCO2 and worsening hypoxemia (PaO2/ FIO2 140 mm Hg) after the initial 6 hrs of treatment prompted the start of isoflurane by inhalation delivered via an Ohmeda 7000 anesthesia ventilator (DatexOhmeda, Madison, WI). Initial manual bag ventilation before the patient was placed on the anesthesia ventilator resulted in the development of bilateral pneumothoraces that were decompressed by tube thoracostomies. An ABG obtained after the patient had been on the anes- thesia ventilator for 2 hrs demonstrated a pH of 6.68, a PaCO2 of 202 mm Hg, and a PaO2 of 162 mm Hg. Because of lack of improvement in clinical status, worsening hypercapnia and low exhaled tidal volumes (~100 mL), the patient was disconnected from the anesthesia ventilator. Three hours after the resumption of ventilation using a Puritan-Bennet ventilator, an ABG revealed a PaCO2 of 180 mm Hg and peak and plateau pressures were 94 and 32 cm H2O, respectively. Over the next 8 hrs, her airway pressures and ABGs improved such that the patient’s PaCO2 was 80 mm Hg 36 hrs after admission to ICU and sodium bicarbonate and neuromuscular blockade infusions were discontinued. At 48 hrs, the patient continued to improve with near normalization of PaCO2 and peak airway pressures. The chest tubes were subsequently removed and the patient was extubated on the fourth and fifth hospital days, respectively. The patient developed generalized weakness, presumably secondary to neuromuscular blockers and corticosteroids. Electromyographic studies showed small, short-duration, polyphasic motor unit action potentials and were consistent with a myopathic process with an increase in creatine phosphokinase, which peaked at 3500 U/L before returning to normal. Because of persistent generalized weakness, the patient was discharged to a rehabilitation facility on the eighth hospital day. Motor strength returned to normal by 8 wks after discharge. CASE 2 Figure 1. Patient 1. Arterial blood gas analyses during the initial 36 hrs of admission. 478 A 28-yr-old woman with moderate persistent asthma presented to the emergency department with 2 days history of increasing dyspnea and wheezing. Initial examination revealed a respiratory rate of 30 breaths/min and diffuse wheezing with a prolonged expiratory phase. She was treated with nebulized albuterol continuously and intravenous corticosteroids. Her initial ABG revealed pH 7.27, PaCO2 53 mm Hg, and PaO2 128 mm Hg while wearing a face mask with high-flow oxygen and continuous albuterol. Shortly thereafter, the patient complained of worsening dyspnea, and after 0.5 mL of epinephrine (1:1000) subcutaneously, the patient vomited a large quantity of gastric contents and lost consciousness. After intubation, a large, unmeasured quantity of gastric contents was suctioned from the endotracheal tube. Subsequently, the patient was heavily sedated and while being ventilated manually at 10 breaths/min with a bag/valve device, had a pH 7.07 and a PaCO2 of 107 mm Hg. She was given nebulized albuterol and ipratropium bromide via the endotracheal tube, and intravenous aminophylline, before transfer to the ICU. Upon arrival in the ICU the patient, was ventilated with an Hamilton Veolar ventilator (Hamilton Medical, Reno, NV) set to assist control mode at 16 breaths/ minute, tidal volume of 450 mL (7.5 mL/ kg), PEEP of 5 cm H2O, peak inspiratory flow rate of 130 L/min, and FIO2 of 1.0. The patient was sedated with lorazepam and fentanyl and paralyzed with vecuronium. The peak and plateau pressures were 85 and 36 cm H2O, respectively. A repeat ABG showed worsening respiratory acidosis, pH 6.99, PaCO2 145 mm Hg, and PaO2 130 mm Hg. A supine anteroposterior chest radiograph showed bilateral infiltrates, a deep-sulcus sign on the left, and pneumomediastinum for which a thoracostomy tube was placed into the left hemithorax. In addition to continuous nebulized albuterol, the patient received magnesium (4 g intravenously over 30 mins followed by an infusion of 1 g/hr), and a sodium bicarbonate drip. The ventilatory rate was reduced to 10 breaths/min because of high PEEPi (18 mm Hg) but a subsequent ABG showed pH 6.90, PaCO2 218 mm Hg, and PaO2 153 mm Hg. At that point, inhalation anesthesia was begun using isoflurane. High Ppeak required that inhalation anesthesia be delivered via continuous manual bagging via the circle system of an anesthesia ventilator (Ohmeda 7000, Datex-Ohmeda). Isoflurane was initially administered at an inspired concentration of 5% and then titrated down to 1% to 2% because of systolic blood pressures ⬍90 mm Hg. While on isoflurane therapy, peak airway pressure decreased from 85 to 62 cm H2O within 1 hr and fell further to 50 cm H2O after approximately 8 hrs, which allowed use of the anesthesia ventilator set to produce an exhaled tidal volume of 400 –500 mL. As shown in Figure 2, inhalational agents were associated with progressive improvement in ventilation and oxygenation. An ABG obtained while the patient was receiving isoflurane showed improved pH (7.07) and diminished PaCO2 (120 mm Hg). The patient was continued on inhalation anesthesia for approximately 30 hrs, during which time her airway pressures and ABGs continued to improve. Crit Care Med 2002 Vol. 30, No. 2 Figure 2. Patient 2. Arterial blood gas analyses during the initial 36 hrs of admission. The patient was later noted to have a peak serum creatine phosphokinase level of 37,830 U/L, with a rising creatinine of 2.0 mg/dL from an admission value of 1.1 mg/dL. General anesthesia and paralysis were discontinued toward the end of day 2. Over the next 2 days, the patient improved, which allowed for extubation on the fifth hospital day. She was transferred to an intermediate care unit the following day where she continued to improve with normalization of creatine phosphokinase. Electromyographic studies obtained on the eighth hospital day were consistent with a myopathic process (small, shortduration, polyphasic motor unit action potentials). She was discharged on the 11th hospital day with physical therapy at home. Two months later, she was doing well and her asthma was clinically stable. DISCUSSION These two cases illustrate important issues in the treatment of severe status asthmaticus with extreme hypercapnia. First, they support current understanding regarding the safety of permissive hypercapnia, even at very high levels of PaCO2, for prolonged periods as encountered in these patients. The evolution of hypercapnia, acidosis, and PaO2/FIO2 for each patient is presented in Figures 1 and 2. PaCO2 ⬎150 mm Hg and pH ⬍7.0 persisted for 16 hrs in the first patient and Crit Care Med 2002 Vol. 30, No. 2 for 9 hrs in the second one. Second, both cases address the limitations of anesthesia ventilators in the setting of very high airway resistance. Permissive Hypercapnia. The vast majority of patients with asthma exacerbations are successfully managed with conventional therapy including corticosteroids, inhaled 2-adrenergic agonists, and oxygen, without the need for assisted ventilation. Additional adjunctive therapies, including helium-oxygen mixture, magnesium, and aminophylline, are also sometimes helpful in patients who do not respond promptly (2). Approximately 2% of patients hospitalized for acute asthma require ventilatory assistance (3, 4). Permissive hypercapnia or controlled hypoventilation has become a commonplace strategy to limit complications of mechanical ventilation (e.g., volutrauma) that may result from extreme dynamic hyperinflation (1, 2, 5). Permissive hypercapnia is defined as limitation of alveolar ventilation with acceptance of elevated arterial CO2 concentrations to protect the lungs against large tidal volume ventilation (volutrauma) and hemodynamic consequences of increased intrathoracic pressures (5, 6). Several studies that incorporated permissive hypercapnia into the ventilatory management of acute respiratory failure suggest that moderate levels of hypercapnia are well tolerated and carry few deleterious effects, thus outweighing the potential adverse affects of hypercapnia. Furthermore, it has been suggested that in the setting of acute organ injury, hypercapnia may be protective whereas hypocapnia may worsen the underlying organ dysfunction (7). The beneficial effects of hypercapnia may be attributable to acidosis-related attenuation of reactive oxygen species formation and apoptosis (8, 9). Although there is no consensus on the level of hypercapnia that is safe, most physicians avoid PaCO2 levels ⬎100 mm Hg. A major concern regarding permissive hypercapnia is the development of intracellular acidosis. Acute hypercapnia causes a decrease in intracellular and extracellular pH. Intracellular pH returns to 90% of normal within 3 hrs as a result of effective intracellular buffers (e.g., proteins and phosphates), reduced proton generation, and changes in transmembrane ion exchange (1, 10). Thus, in normoxic environments acute hypercapnia has limited potential for inducing severe intracellular acidosis and related cytotoxicity (11–13). The major contraindication for permissive hypercapnia is related to the vasodilatory effects of CO2 on cerebral T his report illustrates the challenges of mechan- ical ventilation in severe status asthmaticus, supports the notion that permissive hypercapnia is relatively safe, and highlights the need for careful forethought in the use of inhalational anesthetics for the treatment of status asthmaticus. vessels. Cerebral blood flow reaches its maximum at PaCO2 levels of ~120 mm Hg (14), which may increase intracranial pressure and aggravate preexisting intracranial hypertension (e.g., space-occupying lesion, head trauma, and severe hypertension) (1). Whereas hypercapnia in the absence of hypoxemia has not been associated with cerebral edema in experimental models (15), permissive hypercapnia can cause subarachnoid hemorrhage and cerebral edema in humans (16 –18). Clinical reports of hypercapniainduced intracranial hypertension and resulting cerebral edema include fixed, dilated pupils (17, 18), quadriparesis, hyperreflexia, and extensor plantar reflexes (19). Most of these neurologic findings are reversible and resolve with improvement in hypercapnia and intracranial pressure. In the absence of a preexisting cerebral disease, hypercapnia-associated intracranial hypertension appears to be well tolerated (20). Hypovolemia is also a contraindication, as acute hypercapnia can cause a transient fall in cardiac contractile force (by interfering with the response of myofilaments to calcium) and precipitate cardiovascular collapse, particularly during low inotropic states (21, 22). Inhalational Anesthetics. Inhalational anesthetics are potent bronchodilators and have been successfully used in the management of status asthmaticus refractory to conventional therapy. However, they are generally reserved for the most refractory cases. Inhalational anes479 thetics have been shown to decrease airway resistance, dynamic hyperinflation, and intrinsic positive end-expiratory pressure (23). They result in rapid bronchodilatory response as a result of relaxation of airway smooth muscle (23), and their use has been associated with early liberation from mechanical ventilation (24). Several case reports describe the successful use of inhalational anesthetics in the management of refractory asthma (24 –27). A limitation is that even though readily available, internists as well as intensivists not trained in anesthesia may not be familiar with the anesthesia ventilators and the inability of these ventilators to ventilate against increased airway resistance. These ventilators differ from the commonly used ICU ventilators in their flow and pressure capabilities. Specifically, these ventilators are not capable of generating inspiratory pressures sufficient to ventilate patients with severely elevated airway resistance. The decrease in inspiratory flow that occurs with increasing airway pressure limits the tidal volume delivered and therefore maximal minute ventilation of anesthesia ventilators (28). In fact, mean inspiratory flow decreases to only 40 L/min when Ppeak reaches 60 cm H2O and continues to decrease further with increasing airway pressure. Because of these limitations, as in the first case presented, inhalation anesthesia may be more hazardous than beneficial. New anesthesia ventilators (e.g., Ohmeda 7810, Datex-Ohmeda) have increased flow capabilities and anesthetic agents can be administered via modified Siemens Servo 900D ventilators (Siemens Medical Systems, Iselin, NJ) (29). If neither is available, the alternative is manual bagging until the airway pressure is low enough to allow the use of an anesthesia ventilator. Although many physicians feel uncomfortable with PaCO2 levels above 80 – 100 mm Hg, several case reports indicate that short durations of extreme hypercapnia (⬎150 mm Hg) are well tolerated (13, 30, 31). A recent report described the case of an asthmatic patient who had a maximum PaCO2 of ~200 mm Hg for 10 hrs with no immediate or late consequences (32). The patients we report had PaCO2 levels that are among the highest reported in the medical literature. This extreme hypercapnia was the result, in part, of the limited ability of commonly available anesthesia ventilators to deliver inhalational agents. Importantly, both pa480 tients recovered fully despite prolonged, extreme hypercapnia. Both patients had complications related to very high airway pressures and difficulties associated with the use of inhalational anesthetics, however, both recovered with no major consequences attributable to prolonged hypercapnia. 16. 17. 18. REFERENCES 1. Feihl F, Perret C: Permissive hypercapnia. How permissive should we be? Am J Respir Crit Care Med 1994; 150:1722–1737 2. Corbridge TC, Hall JB: The assessment and management of adults with status asthmaticus. Am J Respir Crit Care Med 1995; 151: 1296 –1316 3. Scoggin CH, Sahn SA, Petty TL: Status asthmaticus. A nine-year experience. JAMA 1977; 238:1158 –1162 4. Mountain RD, Sahn SA: Clinical features and outcome in patients with acute asthma presenting with hypercapnia. Am Rev Respir Dis 1988; 138:535–539 5. Darioli R, Perret C: Mechanical controlled hypoventilation in status asthmaticus. Am Rev Respir Dis 1984; 129:385–387 6. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The Acute Respiratory Distress Syndrome Network. N Engl J Med 2000; 342: 1301–1308 7. Laffey JG, Kavanagh BP: Carbon dioxide and the critically ill—too little of a good thing? Lancet 1999; 354:1283–1286 8. Allen DB, Maguire JJ, Mahdavian M, et al: Wound hypoxia and acidosis limit neutrophil bacterial killing mechanisms. Arch Surg 1997; 132:991–996 9. Xu L, Glassford AJ, Giaccia AJ, et al: Acidosis reduces neuronal apoptosis. Neuroreport 1998; 9:875– 879 10. Siesjo BK: Quantification of pH regulation in hypercapnia and hypocapnia. Scand J Clin Lab Invest 1971; 28:113–119 11. Kraig RP, Petito CK, Plum F, et al: Hydrogen ions kill brain at concentrations reached in ischemia. J Cereb Blood Flow Metab 1987; 7:379 –386 12. Goldman SA, Pulsinelli WA, Clarke WY, et al: The effects of extracellular acidosis on neurons and glia in vitro. J Cereb Blood Flow Metab 1989; 9:471– 477 13. Xu Y, Cohen Y, Litt L, et al: Tolerance of low cerebral intracellular pH in rats during hyperbaric hypercapnia. Stroke 1991; 22: 1303–1308 14. Autoregulation. Arterial and intracranial pressure. In: Cerebral Flow and Metabolism. Edvinsson L, MacKenzie ET, McCulloch J (Eds). New York, Raven Press, 1993, pp 553–580 15. Cohen Y, Chang LH, Litt L, et al: Stability of brain intracellular lactate and 31P-metabolite levels at reduced intracellular pH during 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. prolonged hypercapnia in rats. J Cereb Blood Flow Metab 1990; 10:277–284 Rodrigo C, Rodrigo G: Subarachnoid hemorrhage following permissive hypercapnia in a patient with severe acute asthma. Am J Emerg Med 1999; 17:697– 699 Dimond JP, Palazzo MG: An unconscious man with asthma and a fixed, dilated pupil. Lancet 1997; 349:98 Gaussorgues P, Piperno D, Fouque P, et al: Intracranial hypertension during status asthmaticus. Ann Fr Anesth Reanim 1987; 6:38 – 41 Zender HO, Eggimann P, Bulpa P, et al: Quadriparesia following permissive hypercapnia and inhalational anesthesia in a patient with severe status asthmaticus. Intensive Care Med 1996; 22:1001 Lanier WL, Weglinski MR: Intracranial pressure. In: Clinical Neuroanesthesia. Cucchiara RF, Michenfelder JD, (Eds). New York, Churchill Livingstone, 1991, pp 77–110 Foex P, Fordham RM: Intrinsic myocardial recovery from the negative inotropic effects of acute hypercapnia. Cardiovasc Res 1972; 6:257–262 Orchard CH, Kentish JC: Effects of changes of pH on the contractile function of cardiac muscle. Am J Physiol 1990; 258:C967–C981 Maltais F, Sovilj M, Goldberg P, et al: Respiratory mechanics in status asthmaticus. Effects of inhalational anesthesia. Chest 1994; 106:1401–1406 Parnass SM, Feld JM, Chamberlin WH, et al: Status asthmaticus treated with isoflurane and enflurane. Anesth Analg 1987; 66: 193–195 Echeverria M, Gelb AW, Wexler HR, et al: Enflurane and halothane in status asthmaticus. Chest 1986; 89:152–154 Johnston RG, Noseworthy TW, Friesen EG, et al: Isoflurane therapy for status asthmaticus in children and adults. Chest 1990; 97: 698 –701 Saulnier FF, Durocher AV, Deturck RA, et al: Respiratory and hemodynamic effects of halothane in status asthmaticus. Intensive Care Med 1990; 16:104 –107 Marks JD, Schapera A, Kraemer RW, et al: Pressure and flow limitations of anesthesia ventilators. Anesthesiology 1989; 71:403– 408 Schwartz DE: The use and monitoring of inhalation anesthetics in the intensive care unit. In: Principles and Practice of Monitoring in the Intensive Care Unit. Tobin MJ (Ed). New York, McGraw-Hill, 1998, pp 1251–1266 Potkin RT, Swenson ER: Resuscitation from severe acute hypercapnia. Determinants of tolerance and survival. Chest 1992; 102: 1742–1745 Slinger P, Blundell PE, Metcalf IR: Management of massive grain aspiration. Anesthesiology 1997; 87:993–995 Adnet F, Plaisance P, Borron SW, et al: Prolonged severe hypercapnia complicating near fatal asthma in a 35-year-old woman. Intensive Care Med 1998; 24:1335–1338 Crit Care Med 2002 Vol. 30, No. 2