Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
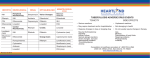
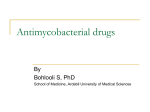
S50 Use of Rifabutin in the Treatment of Pulmonary Tuberculosis Carlo Grassi and Vittoria Peona From the Respiratory Diseases Clinic, Pavia, Italy This article reviews recent studies conducted outside the United States assessing the efficacy and safety of rifabutin in the treatment of tuberculosis (TB) in HIV-infected patients, in patients with newly diagnosed TB, and in patients with multidrug-resistant TB. A 6-month pilot study of 50 Ugandan patients with TB associated with HIV infection showed that rifabutin and rifampin were similarly effective with regard to conversion of sputum-smear findings (sputum conversion) and in bringing about clinical and radiologic improvement. Compared with rifampin, rifabutin showed potential for reducing the time to sputum conversion for these patients. Multicenter studies in five countries compared two rifabutin dosages (150 mg/d and 300 mg/d) with rifampin as part of a combination regimen for treatment of newly diagnosed TB in 935 patients. Rifabutin compared favorably with rifampin in sputum conversion; administration of 150 mg/d of rifabutin yielded good results and the fewest adverse effects. The use of rifabutin by 270 patients in five countries who had multidrug-resistant TB (...... 90% of isolates tested were resistant to rifampin and isoniazid) was assessed in another study. For the majority of these patients, signs and symptoms diminished; onethird had bacteriologic conversions. Major factors contributing to the resurgence of tuberculosis (TB) include the growing rate of HIV infection, poor housing, overcrowding, and migration [1]. Of these factors, HIV infection is the most potent risk factor for the development of active TB. Because HIV destroys CD4 T lymphocytes and macrophages, cells that play a central role in antimycobacterial defenses, people with HIV infection are more vulnerable than the general population to reactivation of latent Mycobacterium tuberculosis infection [2]; clinical disease follows quickly after infection. This problem is especially prevalent in developing countries. Since the late 1980s, the annual number of patients with both TB and HIV infection has nearly tripled in Zambia and more than doubled in Malawi and Uganda [3]. Diagnosis of TB in patients with HIV infection may be delayed because of atypical presentation or poor management. Such delays in treatment may lead to an increased period of infectivity and transmission to other susceptible persons [4]. Drug resistance may also play a role. Patients who have been treated with a first-line agent that proves to be ineffective only after several weeks have elapsed [5] may have infected other susceptible individuals during that period. Managing the TB epidemic depends not only on preventing reactivation of latent infection but also on preventing primary transmission of TB [6]. The aims of treatment of active disease are to eliminate M tuberculosis from sputum cultures in the shortest time, to prevent the emergence of drug resistance, and to prevent relapse. The dramatic increase in single drug-resistant and multidrug-resistant strains of M. tuberculosis has raised concern throughout the medical community. From January to March 1991, 10% of all culture-positive cases of TB in the United States were found to be resistant to isoniazid and/or rifampin [7]. The overall rate of resistance of M. tuberculosis to one or more drugs was found to be 14.2% [7]. Noncompliance is probably the major factor associated with the increased incidence of drug-resistant strains: nearly 95% oftreatment failures are due to this cause [8]. Standard treatment regimens for drug-susceptible TB, such as administration of isoniazid/rifampin/pyrazinamide for 2 months and then isoniazid/rifampin for 4 months, yield cure rates of >95% [9]. Even for isoniazid-resistant organisms, cure rates of >90% are achievable by addition of ethambutol or streptomycin to the regimen [9-11]. However, resistance to both isoniazid and rifampin markedly reduces the efficacy of treatment and is associated with failure rates of 40%-70% [10-12]. Rifabutin is active against a variety of mycobacteria, including M. tuberculosis and atypical strains such as Mycobacterium intracellulare and Mycobacterium avium [13, 14]. It has greater activity than rifampin against M. tuberculosis and, more important, is active against . . . . 35% of strains that are resistant to rifampin [15, 16]. Comparison of Rifabutin and Rifampin in the Treatment of TB in HIV-Infected Patients Study Design Reprints or correspondence: Professor Carlo Grassi, Respiratory Diseases Clinic, via Taramelli 5, 27100 Pavia, Italy. Clinical Infectious Diseases 1996;22(Suppll):S50-4 © 1996 by The University of Chicago. All rights reserved. 1058-4838/96/2201-0052$02.00 The first direct comparison of rifabutin and rifampin in the treatment of HIV-I-associated TB was conducted by Schwander et al. [17], who studied 50 Ugandan patients with HIV-1 infection and culture-positive pulmonary TB. The pilot em 1996;22 (Suppl 1) Treatment of Pulmonary TB with Rifabutin study was designed to evaluate the feasibility of a larger, phase III trial using a four-drug regimen with rifabutin instead of rifampin. A 2-month initiation phase of treatment consisted of the administration of isoniazid (300 mg/d), ethambutol (800 or 1,200 mg/d), pyrazinamide (1,500 or 2,000 mg/d), and either rifampin (450 or 600 mg/d) or rifabutin (150 or 300 mg/d). The lower dosages were used for patients with body weights of <50 kg. After the initial phase, ethambutol and pyrazinamide were withdrawn, and patients received daily treatment with isoniazid and either rifampin or rifabutin for an additional 4 months. To improve compliance, patients received their medication at the Joint Clinical Research Centre in Kampala twice weekly during the initiation phase and once weekly during the continuation phase. Results Forty-one patients (82%) completed the 6-month treatment course, and their conditions improved. Six patients, 4 treated with the rifabutin regimen and 2 with the rifampin regimen, died during the study period (5 died of nonmycobacterial HIVassociated complications and 1 of a multidrug-resistant M. fortuitum infection). Three patients were withdrawn because of protocol violations. Clinical improvement was assessed by the decrease in mean body temperature and mean respiration rate, the decrease in frequency of productive cough and night sweats, and the increase in Kamofsky performance score and body weight. None ofthese parameters differed significantly between the treatment regimens. Radiologically evident improvement was seen in 95% of patients receiving the rifabutin regimen and in 100% of patients receiving the rifampin regimen. Microbiological efficacy was assessed by measuring the time from the first day of therapy to (1) the first of three consecutive negative sputum smears and cultures or (2) a negative sputum smear followed by consistent absence of sputum production. Sputum conversion (i.e., conversion of sputum smear findings to negative) occurred in 42 patients, 21 in each treatment group. However, patients receiving the rifabutin regimen had a significantly lower number of positive smears during the first 8 weeks of treatment than did patients receiving the rifampin regimen (P < .05, log rank test). The number of patients was too small to show a statistically significant difference between the two groups in terms of the mean time to sputum conversion. More than half of the patients in each treatment group reported mild, moderate, or (rarely) severe episodes of arthralgia up to week 8. Other, less frequently reported symptoms were myalgia, nausea, vomiting, gastrointestinal discomfort, and loss of appetite. After week 8, the frequency and grade of these symptoms decreased when the amount of study medication was decreased. No major differences in frequency or grade of S51 severity of any of the reported side effects were observed between the two groups. Conclusions In this pilot study of patients with TB and HIV infection, both rifampin and rifabutin regimens were effective in inducing clinical and radiological improvement. Both regimens were well tolerated. However, the sputum of patients treated with the rifabutin regimen was significantly more rapidly cleared of acid-fast bacilli than was that of patients treated with the rifampin regimen. A larger study is warranted to confirm this observation. An earlier sputum conversion time may have important implications for shortening the infectious period of pulmonary TB and reducing further spread of M. tuberculosis. Treatment of Newly Diagnosed Pulmonary TB in HIVNegative Patients Study Design To assess the efficacy and safety of rifabutin in the treatment of newly diagnosed TB, five multicenter, randomized, open, controlled studies were conducted. An identical protocol was used in studies originating in Argentina, Brazil, and Thailand. Data from these studies were combined for analysis [18]. Two additional protocols were used in studies conducted in South Africa and Spain [19, 20]. Patients with previously untreated TB were eligible for the studies in all five countries. They were required to have two sputum cultures positive for M. tuberculosis plus clinical signs and symptoms and radiological evidence of disease. Patients included in these studies were HIV-negative. A total of 520 patients were enrolled in the three studies with the identical protocol. In the Spanish and South African studies, 415 patients were enrolled. There were no significant differences between the treatment groups regarding demographics and baseline findings. In the three combined studies, patients were randomly assigned to an 8-week multidrug regimen of rifabutin (150 mg/d or 300 mg/d) or rifampin (600 mg/d) plus isoniazid (300 mg/d), ethambutol (25 mg/[kg' dD, and pyrazinamide (30 mg/[kg' dD. Treatment with the same dosages ofrifampin or rifabutin plus isoniazid was then continued for an additional 16 weeks. In the South African study, patients received either rifabutin (300 mg/d) or rifampin (600 mg/d) plus isoniazid (400 mg/d), ethambutol (1,200 mg/d), and pyrazinamide (2,000 mg/d) for 8 weeks, followed by 16 weeks of triple-drug therapy (administered twice weekly) with rifabutin (300 mg/d) or rifampin (600 mg/d) plus isoniazid (600 mg/d) and ethambutol (2,400 mg/d). Patients in the Spanish study received daily doses of either rifabutin (300 mg/d) or rifampin (600 mg/d) plus isoniazid S52 Grassi and Peona Table 1. Rifabutin vs. rifampin in the treatment of newly diagnosed tuberculosis: rates of success (bacteriologic conversion noted at last valid observation), per data combined from several studies [18]. Success rate (percent of patients) Rifabutin Study site Rifampin 600 mgld Argentina Brazil Thailand All sites 87 82 97 89 150 mgld 300 mgld 100 94 92 89 92 81 99 94 (300 mg/d) for 36 weeks; ethambutol (25 mg/[kg . d]) was added to the regimen during the first 8 weeks of treatment. Efficacy The criteria used to assess efficacy were the same for all five studies. Sputum samples were collected prior to initiation of drug therapy, fortnightly for the first 2 months of therapy, and then at weeks 12, 16, and 24 (and 36 in the Spanish study). Therapeutic efficacy was evaluated by assessment of bacteriologic conversion of sputum cultures from positive to negative. Conversion was considered to have occurred if two successive sputum cultures were negative at the end of the treatment or at the last valid observation (the last visit at which the patient had a recorded value on the case record form while receiving treatment; patients with missing data on cultures or who had withdrawn from the study for any reason were considered treatment failures). If conversion occurred by week 12, it was not necessary to have two successive negative cultures for conversion to be considered valid. Clinical efficacy was assessed by the monitoring of the occurrence of fever, dyspnea, cough, and anorexia and by performance of clinical laboratory tests and regular chest roentgenography. In the combined studies, patients who were successfully treated were followed up by means of cultures performed every 6 months for up to 2 years after therapy was completed. If two successive cultures were positive during this follow-up period, after culture negativity had been achieved during treatment, then the patient was considered to have had a relapse. em 1996; 22 (Suppl 1) also comparable among the treatment groups: 34 days for rifampin and 37 days for each of the rifabutin groups. Follow-up data for patients in the combined studies show a low relapse rate. A total of 5 patients (1 %) relapsed, of whom 2 were in the 300-mg rifabutin group, 1 was in the rifampin group, and 2 were in the 150-mg rifabutin group. Symptoms of fever, cough, and anorexia, which had been reported by more than half of the patients at the time of enrollment, diminished dramatically during treatment in all three groups. At the end of treatment, .improvement was evident on the chest roentgenograms of 97%-100% of all patients. In the South African and Spanish studies, the rate ofbacteriologic conversion among patients treated with rifabutin was similar to that among those treated with rifampin. In the Spanish study, 80% of patients in the rifampin group and 87% of patients treated with rifabutin had negative cultures at week 36. In the South African study, treatment with rifampin resulted in a 90% success rate at the last valid observation, vs. a 95% success rate for treatment with rifabutin (data on file, Pharmacia, Milan, Italy). Adverse Events In the three combined studies, adverse events were reported by 9% of patients receiving rifampin vs. 8% of patients receiving 150-mg doses of rifabutin and 17% of patients receiving 300-mg doses of rifabutin. Gastrointestinal symptoms were the most common adverse effect in all three treatment groups. The 150-mg dose of rifabutin was associated with fewer musculoskeletal, hematologic, and lymphatic abnormalities and fewer gastrointestinal complaints than were the 300-mg dose of rifabutin and rifampin. Discontinuation of treatment due to an adverse event occurred for no patients in the 150-mg rifabutin group, one patient in the rifampin group, and five in the 300-mg rifabutin group. Of the adverse events reported, 26% in the rifampin group, 4% in the 150-mg rifabutin group, and 8% in the 300-mg rifabutin group were considered severe. Three of 5 deaths that occurred were considered drug-related: 2 in the 300-mg rifabutin group (thrombocytopenia and cerebral hemorrhage occurred in 1 patient and severe vomiting in the other) and 1 in the rifampin group (severe gastrointestinal disease, purpura, and erythematous rash occurred). Conclusions Results A total of 513 patients in the combined studies had positive cultures at baseline and were included in the intent-to-treat analysis. The rate at which bacteriologic conversion was noted at each patient's last valid observation was 94% in the group receiving 150-mg doses ofrifabutin, 92% in the group receiving 300-mg doses of rifabutin, and 89% in the group receiving rifampin (table 1). The median time to culture conversion was The results of these studies show that a 150-mg dose of rifabutin, a 300-mg dose of rifabutin, and rifampin are all effective in clearing sputum of M. tuberculosis. Rifabutin compared favorably with rifampin in terms of bacteriologic conversion and clinical improvement. Good results were achieved with 150 mg of rifabutin, and this lower dosage was associated with fewer adverse effects than the number occurring with rifampin or 300 mg of rifabutin. The results suggest that rifa- em 1996;22 (Suppl 1) Treatment of Pulmonary TB with Rifabutin butin is well tolerated and is an effective alternative to rifampin in multidrug regimens for the treatment of newly diagnosed pulmonary TB. Treatment of Chronic Multidrug-Resistant Pulmonary TB 50 ~ .e...... E CD ~ c. CD The conditions of patients with chronic multidrug-resistant pulmonary TB often fail to respond to anti-TB therapy with rifampin and isoniazid, which are generally used in combination with other drugs. The safety and efficacy of rifabutin as an alternative to rifampin in this patient population were assessed in five uncontrolled, open studies in centers in Algeria, Argentina, France, South Africa, and Spain [21]. A total of 270 patients with confirmed pulmonary TB who had failed to respond to previous standard therapy were enrolled. Nearly 60% of these patients were considered to have severe advanced disease at baseline. Approximately 80% of patients had previously completed a 12-week course of antiTB therapy; 70% had completed at least 6 months of treatment. Patients were allocated to receive treatment with a 6- to 12month multidrug regimen including rifabutin (300 mg/d or 450 mg/d). The lower dosage was used if a patient weighed <50 kg. Nine patients in the French study weighing> 50 kg received 600 mg/d. Concomitant antimycobacterial medication was selected according to the results of in vitro susceptibility testing of sputum isolates. Fifty-eight percent of patients received kanamycin; 50%, ethambutol; 48%, pyrazinamide; and 24.5%, isoniazid. Efficacy Efficacy was assessed by the monitoring of conversion of sputum cultures from positive to negative during the treatment period. Conversion was considered to have occurred if two successive cultures were negative at the end of treatment or at the last valid observation (defined as the time when data were last recorded for each patient, regardless of the length of treatment). If conversion occurred at week 12, only one negative culture was considered necessary. Clinical improvement was assessed by the reduction of signs and symptoms ofTB (i.e., cough, dyspnea, and anorexia) from the baseline evaluation to the last valid observation. If a patient had been observed at baseline only, this was considered the last valid observation. Drug Resistance Different methods of assessing the drug susceptibility of M. tuberculosis isolates were used in the various studies; thus, different breakpoints were adopted for the definition of susceptibility and resistance. For this reason, comparison of suscepti- 40 30 > .~ 0) Q) Study Design S53 c: E :::J 20 '5 enc. 10 o Argentina (n=68) Spain (n=33) Algeria (n=46) France (n=35) S. Africa Combined (n=38) (n=220) Figure 1. Rifabutin in the treatment of multidrug-resistant tuberculosis: rates of bacteriologic conversion of sputum, as noted at the last valid observation (intent-to-treat analysis). bility data across studies cannot be regarded as accurate. Overall, 90% of strains tested were resistant to rifampin and isoniazid, 75% were resistant to streptomycin, and 50% were resistant to ethambutol. Results The percentage of patients for whom bacteriologic conversion was noted at the last valid observation (intent:.:to-treat analysis) is presented in figure 1. Overall, at the last valid observation, bacteriologic conversion had occurred for 34% of all patients analyzed. The results appeared to be independent of the concomitant medication administered. Adverse Events Eleven patients (4% of all patients treated) were prematurely withdrawn from study because of an adverse event. Adverse events that resulted in early discontinuation of therapy were related primarily to the gastrointestinal system. Although a number of patients' hematologic and biochemical values changed during the study, none showed evidence of severe hepatic, renal, or hematologic toxicity. Eighteen patients died of TB during the study. Conclusions In these five studies, rifabutin proved beneficial for patients with chronic drug-resistant pulmonary TB that had been unresponsive to previous therapies, including those with rifampin. In the majority of patients, the signs and symptoms of disease diminished during treatment; in one-third ofthe patients, mycobacteria were cleared from the sputum. The drug regimens used in these studies were well tolerated, and the incidence of ad- S54 Grassi and Peona verse events was low. Few patients discontinued treatment as a result of adverse effects oftherapy. Rifabutin, as a component of combination drug therapy, is associated with a positive risk:benefit ratio in the treatment ofpatients with chronic multidrug-resistant pulmonary TB. Summary The results of these studies, which explored the safety and efficacy of the use of rifabutin in the treatment of patients with TB and HIV, with newly diagnosed TB, and with multidrugresistant TB, suggest that rifabutin can play a role in therapy for TB. It is acknowledged, however, that many ofthe data contained in this review have (to date) been published only in abstract form and, as such, can best be described as preliminary. Nevertheless, some interesting findings have emerged from these studies. Although the pilot study of HIV-infected patients with TB was too small to show a statistically significant difference between rifabutin and rifampin with regard to the mean time to sputum conversion, the results for rifabutin were promising. Rifabutin was associated with a lower number of positive smears in the first 8 weeks of treatment; this finding, if confirmed by a large-scale clinical trial, could have important implications for shortening the infectious period of TB. This would greatly reduce the transmission of this disease among high-risk patients. In the treatment of newly diagnosed TB in HIV-negative patients, rifabutin was shown to be as effective as rifampin in combination regimens. Particularly at a lower dosage of 150 mg/d, rifabutin showed good efficacy and had a favorable tolerability profile. Predictably, higher doses of rifabutin were more effective in patients with chronic multidrug-resistant TB. Rifabutin clearly has considerable potential for use in the treatment of multidrug-resistant TB, particularly when susceptibility to rifabutin and resistance to rifampin and other drugs have been demonstrated. The results of these studies await confirmation in larger, well-controlled, comparative trials. Furthermore, in view of the importance of compliance in preventing the development of resistance, future studies should address this issue specifically. Although several aspects of optimizing rifabutin therapy remain to be resolved, evidence to date clearly indicates that rifabutin is an effective alternative to rifampin in the treatment ofTB. References 1. Brudney K, Dobkin J. Resurgent tuberculosis in New York City: human immunodeficiency virus, homelessness and the decline of tuberculosis control programs. Am Rev Respir Dis 1991; 144:745-9. em 1996;22 (Suppl 1) 2. Di Perri G, Cruciani M, Danzi MC, et al. Nosocomial epidemic of active tuberculosis among HIV-infected patients. Lancet 1989;2:1502-4. 3. Klaudt K, ed. TB: a global emergency. WHO report on the TB epidemic [WHOITB/94.177]. Geneva: World Health Organization, 1994. 4. Barnes PF, Bloch AB, Davidson PT, et al. Tuberculosis in patients with human immunodeficiency virus infection. N Engl J Med 1991; 324:1644-50. 5. Davey RT Jr. Mycobacterial disease in HIV infection: recent therapeutic advances. In: Lane HC, moderator. Recent advances in the management of AIDS-related opportunistic infections. Ann Intern Med 1994; 120:945-55. 6. Hamburg MA, Frieden TR. Tuberculosis transmission in the 1990s. N Engl J Med 1994;330:1750-1. 7. Bloch AB, Cauthen GM, Onorato 1M, et al. Nationwide survey of drug resistant tuberculosis in the United States. JAMA 1994;271:665-71. 8. Davidson PT, Le HQ. Drug treatment of tuberculosis-1992. Drugs 1992;43:651-73. 9. Combs DL, O'Brien RJ, Geter LJ. USPHS tuberculosis short course chemotherapy trial 21: effectiveness, toxicity and acceptability. The report of the final results. Ann Intern Med 1990; 112:397-406. 10. Hong Kong Chest Service/British Medical Research Council. Controlled trial of 2, 4, and 6 months of pyrazinamide in 6-month-three-timesweekly regimens for smear-positive pulmonary tuberculosis, including an assessment of a combined preparation of isoniazid, rifampicin and pyrazinamide. Am Rev Respir Dis 1991; 143:700-6. 11. Mitchison DA, Nunn AJ. Influence of initial drug resistance on the response to short course chemotherapy of pulmonary tuberculosis. Am Rev Respir Dis 1986; 133:423-30. 12. Iseman MD, Madsen LA. Drug-resistant tuberculosis. Clin Chest Med 1989; 10:341-53. 13. Della Bruna C, Schioppacassi G, Ungheri D, Jabes D, Morvillo E, Sanfilippo A. LM 427, a new spiropiperidylrifamycin: in vitro and in vivo studies. J Antibiot (Tokyo) 1983;36:1502-6. 14. Heifets LB, Iseman MD, Lindholm-Levy PJ. Determination of MICs of conventional and experimental drugs in liquid medium by the radiometric method against Mycobacterium avium complex. Drugs Exp Clin Res 1987; 13:529-38. 15. Woodley CL, Kilburn 10. In vitro susceptibility of Mycobacterium avium complex and Mycobacterium tuberculosis strains to a spiro-piperidyl rifamycin. Am Rev Respir Dis 1982; 126:586-7. 16. Mitchison DA, Ellard GA, Grosset J. New antibacterial drugs for the treatment of mycobacterial disease in man. Br Med Bull 1988;44: 757-74. 17. Schwander S, Riisch-Gerdes S, Mateega A, et al. A pilot study of antituberculous combinations comparing rifabutin with rifampin in the treatment ofHIV-associated tuberculosis: a single, blinded, randomized evaluation in Ugandan patients with HIV-1 infection and pulmonary tuberculosis. Tuber Lung Dis 1995;76:210-8. 18. Gonzales-Montaner LJ, Natal S, Yongchalyud P, et al. Rifabutin for the treatment of newly diagnosed pulmonary tuberculosis: a multinational, randomized, comparative study versus rifampin. Tuber Lung Dis 1994;75:341-7. 19. Felten MK. Preliminary experience with rifabutine (ansamycin LM 427) in patients with newly diagnosed pulmonary tuberculosis (PTB) and chronic disease [abstract A 136]. Joint Annual Meeting of the American Lung Association and the American Thoracic Society (New Orleans). Am Rev Respir Dis 1987; 135(4): part 2. 20. Rey R, Ramos A, Munoz L, et al. Estudio clinico controlado con rifabutina en e1 tratamiento de la tuberculosis pu1monar inicial [abstract]. Primo Congreso Luso-espanol de Pneumologia (Lisbon), 21-24 May 1989. 21. Rey-Duran R, Boulahbal F, Gonzales-Montaner LJ, et al. Role ofrifabutin in the treatment of chronic drug-resistant pulmonary tuberculosis. In: Program and abstracts of the 7th International Conference on AIDS: Satellite Symposium on the Therapeutic Approach to Mycobacterial Infections in AIDS. Florence, Italy: Istituto Superiore di Sanita, 1991:33-5.