Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
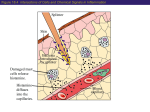
A Comparison of a Single-Step Cold-Dry Air Challenge and a Routine Histamine Provocation for the Assessment of Bronchial Responsiveness in Children and Adolescents* Bernhard Steinbrugger, MD; Ernst Eber, MD; Manfred Modi, MD; Elisabeth Weinhandl; and Maximilian S. Zach, MD Background: It has remained unclear whether bron¬ chial responsiveness as measured by a single-step cold-dry air challenge (CACh) correlates closely to the responsiveness that is assessed by a routine pharma¬ cologic challenge. Methods: On 2 consecutive days, we performed a CACh and a histamine challenge in 128 symptom- and medication-free pediatric and adolescent asthma pa¬ tients. The CACh consisted of 4 min of isocapnic hyperventilation of -10°C, absolutely dry air; respon¬ siveness was expressed by the induced change in FEVi (AFEVi). The histamine challenge consisted of se¬ quential inhalations of incremental increases in con¬ centrations of histamine; responsiveness was expressed by the concentration which caused a 20% fall of FEVi (PC20). Results: Five children did not bronchoconstrict suffi¬ ciently in the histamine challenge for measuring a PC20 and were excluded from analysis. In the remain¬ ing 123, AFEVi (CACh) ranged from +5 to -73%, PC20 (histamine) from 0.05 to 7.2 mg/mL. There was a sta¬ tistically significant correlation between AFEVi and measured by routinelysubstances like active inhaling pharmacologically histamine or methacholine; alternatively, it can be as¬ sessed by challenges that apply physical stimuli like the hyperventilation of cold and dry air (cold-dry air challenge=CACh). The CACh can be done in two ways. Some authors have advocated a multiple-step approach with increas¬ ing levels of cold-dry air hyperventilation; in analogy to challenges, a dose-response curve is pharmacologic constructed and bronchial responsiveness is expressed as that dimension of hyperventilation that causes a change of lung function.12 Others have predetermined used a single-step approach; after applying one single dose of cold-dry air hyperventilation, bronchial respon- TJronchial responsiveness is -¦"* Respiratory and Allergic Disease Division, Pediatric of Graz, Austria. University Department,received November 8, 1994; revision accepted Febru¬ Manuscript ary 24, 1995. Pediatric Dept, University of Reprint requests: Dr. Steinbrugger, A-8036 Graz, Austria *From the Graz, Auenbruggerplatz 30, PC20 (r=0.54, p<0.001), but also a considerable scatter of individual data points around the regression line. Fifty-two subjects were hyperresponsive by CACh and 114 by histamine criteria. Conclusions: There is a relatively weak correlation between the results of these two challenges; thus, one cannot be substituted one for the other. Histamine appears as more sensitive in detecting airway hyper¬ responsiveness than CACh. The poor correlation be¬ tween the responses to these two challenges can be explained by differences between the challenge pro¬ tocols, or, alternatively, by differences between ap¬ plied stimuli and activated mechanisms. (CHEST 1995; 108:741-45) CACh=cold-dry air challenge; FEVi=forced expiratory volume in 1 s; PC20=provocation concentration of hista¬ mine causing a 20% fall in FEVi Key words: bronchial responsiveness; cold-dry lenge; histamine provocation; pediatric asthma air chal¬ quantified in terms of the effected change The relationship of the responses to a conventional challenge on one side and CACh on the pharmacologic other has been studied repeatedly, but results have so far remained contradictory. Several studies that com¬ the responses to a multiple-step CACh with pared those to a histamine or methacholine challenge dem¬ onstrated a very close correlation.8"12 When comparing a histamine or methacholine provocation to a singlestep CACh, however, some authors found close cor¬ relations,13 while others observed only weak correla¬ tions with a relatively low correlation coefficient and a substantial scatter around the regression line.14,15 One study, done in a small number of pediatric subjects, failed altogether to find a correlation between hista¬ mine and CACh responses.5 When compared with conventional pharmacologic a single-step CACh has several practical challenges, and theoretical advantages for measuring bronchial responsiveness.5"7 Before substituting a single-step siveness is in lung function.3"7 CHEST /108 / 3 / SEPTEMBER, 1995 Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21720/ on 05/02/2017 741 challenge, however, the pharmacologic the responses to these two relationship between different types of challenges requires further evalua¬ tion. We therefore compared the responses to a single-step CACh and to a conventional histamine challenge in a large group of pediatric subjects with a CACh for a wide range of bronchial responsiveness. Methods Subjects Subjects were the first 150 participants of an ongoing epidemi¬ ologic study that evaluates all asthma patients of this pediatric res¬ piratory center 1.5 years after having become symptom-free and 1 year after having become medication-free. This epidemiologic study aims at evaluating the prognostic value of lung function, bronchial responsiveness, and allergy skin test reactivity by doing these mea¬ surements and then following up the patients clinically and with repeated measurements. This group of subjects was believed to be ideally suited for the present comparison of two bronchial provo¬ cation methods for several reasons: (1) a previous pilot study had shown this group as having a wide range of bronchial responsive¬ ness,16 and (2) the absence of any antiasthmatic medication that could influence both challenge mechanisms differently. Twenty-two of these 150 subjects were excluded from being challenged. Six patients had marked airwayin obstruction without significant bronchodilator responsiveness their baseline lung functions. Ten further patients remained unable to cooperate with lung function testing and/or hyperventilate sufficiently in the CACh. Another six refused to do more than one bronchial challenge pro¬ cedure. The remaining 128 patients, 48 girls and 80 boys, had a mean age of 13.1 years (SD=2.7; range, 7.8 to 19.4), a mean body weight of 51.4 kg (SD=16.2; range, 23 to 94), and a mean body length of 158 cm (SD=14.3; range, 126 to 187). All were well trained to cooper¬ ate with lung function testing and bronchial provocation proce¬ dures. All were long-term patients of this pediatric asthma center who, previously, before becoming symptom free, had met the clin¬ ical definition of bronchial asthma,17 and had been treated with various antiasthmatic medications (disodium cromoglycate, topical steroids, theophylline, bronchodilators) for a minimum of 3 years before becoming medication free. Single-Step CACh Single-step CACh was done according to an established proto¬ col.5' Cold and dry air was produced by a commercially available heat exchanger (RHES; Jaeger; Wuerzburg, Germany). After the measurement of prechallenge FEVi, subjects hyperventilated ab¬ solutely dry, 10°C air at 75% of their maximum voluntary venti¬ lation for 4 min. The correct level of hyperventilation was main¬ tained by having the subjects compete with a target balloon. A CO2 analyzer continuously monitored the CO2 concentration in the ex¬ pired air, and CO2 was added to the inspired air to keep the sub¬ ject eucapnic. Three minutes after termination of the CACh, FEVi was measured again. The change of FEVi (AFEVi) from the preCACh to the post-CACh measurement was expressed in percent baseline FEVi. For this method, a 9% fall of FEVi or more defines airway hy¬ perreactivity.5,1819 Histamine Challenge Histamine challenge was done according to the present Austrian standardization,20 which is based on the method of Cockcroft et al.21 As a tidal breathing method, this approach is identical with a later European standardization,2 with the exception of using a nebulizer a higher output. Briefly, each step ofthis multiple-step protocol consists of a 2-min inhalation by quiet tidal breathing through a mouthpiece using a nose clip. The first aerosol inhaled after the baseline measurement of FEVi is the diluent, and this is followed at 5-min intervals by doubling concentrations of histamine from 0.03 to 8.0 mg/mL. The FEVi is measured before, at 30 and 60 s, and at 2.5 min after each inhalation. The test is stopped when the FEVi has fallen by 20% or more from baseline or when having gone through all concentrations of histamine. A dose-response curve is constructed by plotting the percent fall in FEVi against the concentration of histamine on a log scale. The result is expressed as the concentration of histamine with causing a 20% fall in FEVi (PC20). Based on the output (0.46 mL/min) of the nebulizer used (Inhalierboy; Pari; Starnberg, Germany), a PC20 under 4 mg/mL defines airway hyperreactivity.20 Study Protocol The two different challenges were done in random order, at 10 days. Before the first challenge, a brief history clinical examination was performed; patients presenting with a recent history and/or the symptoms of an acute respiratory tract infection or an allergen exposure were not accepted for testing, but received a second, later (minimum interval, 6 weeks) appointment. Before each challenge, subjects rested for 1 h in a controlled climate (20°C, 40% relative humidity). Lung function testing was done on a water-filled spirometer (Spiro-Junior; Jaeger; Wuerzburg, Germany) in accordance with standardized guidelines.22 FEVi was expressed in absolute terms and in percent predicted as based on established reference standards.23 After each challenge, recovery of lung function was observed for 20 min; if by then the FEVi had not returned to baseline, the patient was treated with nebulized salbutamol. Such treatment was also administered immediately after the challenge when the patient subjectively felt any shortness of breath. Informed consent to the study was obtained from patients and am on 2 consecutive was obtained and a parents. The least squares correlation analysis was used for the statistical comparison of the responses to CACh and histamine. Logarithmic transformation of the PC20 values was performed for this regres¬ sion analysis. Prechallenge lung functions were compared by one¬ way analysis of variance. A p value of 0.05 and below was taken as indicating statistical significance. Results In five subjects, a 20% fall of FEVi could not be effected in the entire histamine challenge, and a PC20 could thus not be determined. These subjects were excluded from further analysis. In the remaining 123 subjects, the baseline FEVi measurements before CACh (100.7± 11.2% predicted; range, 62 to 126) did not differ significantly from those before the histamine challenge (98.4± 11.1% pre¬ dicted; range, 66 to 126). The induced change in FEVi (CACh) was -11.4±13.8% baseline (range, +5 to -73%). The PC20 (histamine) was 1.87±1.96 mg/mL (range, 0.05 to 7.2). The correlation of AFEVi (CACh) to PC20 (histamine) is shown in Figure 1. This correlation was statistically However, as illustrated by a rel¬ significant (p<0.001). low correlation coefficient (r=0.54) and a con¬ atively siderable scatter of individual data points, this corre¬ lation remained a relatively weak one. 742 Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21720/ on 05/02/2017 Clinical Investigations n = l23 r = o.5a p< 0.001 1I 2 Sg30± 0,06 0,125 Figure 1. Correlation of AFEVj (CACh) to PC20 (histamine). Dashed lines indicate the 0,25 Histamine challenge PC 20 (mg/ml) 52 subjects were found to be hyperAlthoughtoonly the CACh, 114 were hyperresponsive to responsive the histamine challenge. Fifty subjects met the defi¬ nition of bronchial hyperresponsiveness in both tests; conversely, seven were normoresponsive in both prov¬ ocations. Sixty-four were hyperresponsive by histamine but normoresponsive by CACh criteria. Only two subjects with a normal histamine response met the definition of bronchial hyperresponsiveness by CACh criteria; their AFEVi (CACh) was -10% and -11%, to the CACh respectively. Thus, a positive response histamine criteria predicted hyperresponsiveness by with a probability of 96.2%, while a negative CACh response predicted normoresponsiveness by histamine criteria with a probability of only 15.8%. Discussion demonstrates a statistically significant studybetween the airway response to a single relationship dose of cold-dry air hyperventilation on one side, and bronchial responsiveness, as measured by a routine histamine challenge, on the other. As indicated by a around the This wide scatter of the individual data points regression line, however, this correlation remained a weak one. For practical purposes, this indi¬ relatively that the result of a single-step CACh can hardly substitute for measuring bronchial responsiveness by a routine histamine challenge, and vice versa. Such a weakness in the observed correlation could be ex¬ plained by one or several of the following factors: (1) technical inconsistencies in performing the challenges; (2) conceptual differences between the challenge and (3) basic differences between applied procedures; stimuli and activated mechanisms. Data points in the figure indicate that the studied population was somewhat skewed toward subjects with increased airway responsiveness, and the only mildlyarises whether the correlation would cates question have borders between normal and increased bron¬ chial responsiveness for both challenges. been better if subjects had been more evenly distrib¬ uted. As the scatter of data points increases with increasing airway responsiveness, however, a substan¬ tial gain in the quality ofthe correlation by a more even distribution seems highly unlikely. Noise from some inaccuracies in the application of the challenge is an unlikely explanation for the major part of the observed scatter. A previous study of CAChs, done with the same repeated single-step and challenge protocol, has demonstrated technique excellent short-term reproducibility.5 Furthermore, care was taken in the present study to avoid technical and to exclude subjects who did not hyperven¬ pitfalls tilate sufficiently. One previous study that compared the response to a single-step CACh with the outcome of a pharmacologic challenge found a close correla¬ tion,13 while another such investigation failed to do so5; both studies were done in only a small number of subjects. Two other similar investigations demon¬ strated statistically significant, but relatively weak cor¬ relations.1415 Of these two, the investigation by Filuk et al15 has many similarities to the present study. These authors also found a substantial scatter of individual data points around the regression line and suggested that this finding could be explained by frequently ob¬ served technical difficulties, especially a noncompliance of many of their subjects with the hyperventila¬ tion protocol. Based on the above-mentioned care that was taken to avoid such technical inaccuracies in the present study, it seems that this hypothesis can now be rejected, and that other explanations for the apparent weakness of this correlation must be looked for. As an alternative explanation, the observed differ¬ ence in the responses to a single-step CACh and a routine histamine challenge might stem from basic differences between the protocols of the two chal¬ the case of the histamine challenge, a doselenges. Incurve was constructed and bronchial responresponse CHEST /108 / 3 / SEPTEMBER, 1995 Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21720/ on 05/02/2017 743 by siveness was characterized that bronchoconstrictor concentration that effected a certain predetermined lung function. In the case of the single-step change ofa size-corrected CACh, predetermined bronchocon¬ strictor dose was administered, and bronchial respon¬ siveness was quantified in terms of effected lung function changes. These two approaches differ sub¬ and one might speculate that this difference stantially, for the observed weakness of correlation. accounts Such a speculation might find some support from the relevant literature. It seems that those who applied CACh by a multiple-step protocol and thereby imi¬ tated the protocol of routine pharmacologic challenges found closer correlations to histamine and methacho¬ line provocations than those using a single-step CACh.8"15 On the other side, this hypothesis implies that single-step and multiple-step CACh protocols, using the same stimulus and recruiting the despite same reaction mechanisms, would produce two types of bronchial response measurements that are only Paradoxically, such directly com¬ weakly correlated. parative studies of single-step and multiple-step CACh have as yet not been done (to our knowledge). The third hypothesis, offering an explanation for the in the correlation of observedweakness AFEVi (CACh) and PC20 (histamine), relates to the obvious differ¬ ences between applied stimuli and activated mecha¬ nisms. Unlike aerosols of histamine and metha¬ choline, nonpharmacologic challenges do not act di¬ rectly on bronchial smooth muscle, but rather invoke intermediate events like the release of mediators from cells in the airway lumen and submucosa.24 A bron¬ choalveolar lavage study in mildly asthmatic subjects demonstrated that isocapnic hyperventilation effects increases in a spectrum of bronchoactive mediators and inflammatory cells.25 Clearly, when different chal¬ stimuli and activate different lenges apply different should be measuring different types mechanisms, they of airway responsiveness. To take this concept further, there might be no such entity as "nonspecific" bron¬ chial responsiveness, and the responses to any type of provocation might, at least in part, remain specific for the applied stimulus. Coming back to the relatively weak correlation be¬ tween AFEVi (CACh) and PC20 (histamine) that was observed in the present study, it seems that technical inconsistencies can be excluded from the list of possi¬ ble reasons; thus, one is left with the question of dif¬ ferent protocols vs different stimuli. Design and results of the present study do not allow us to decide between these two alternatives; thus, further relevant studies are needed. urgently When using the respective established cutoff points between normal and increased bronchial responsive¬ ness, the histamine provocation defined many more subjects as hyperreactive than the CACh. While only CACh-positive subjects, both with marginally el¬ evated AFEVi (CACh), remained histamine-negative, no less than 64 presented with the combination of normal CACh and increased histamine responsiveness. A routine histamine provocation will thus define a higher proportion of a given population as having bronchial hyperresponsiveness than a single-step CACh. It follows that a single-step CACh has a high positive predictive value for a positive histamine chal¬ but a low negative predictive value for a nega¬ lenge, tive histamine result. This finding is in agreement with the work of Galdes-Sebaldt et al,26 who compared and pharmacologic challenges for nonpharmacologic bronchial asthma in a pediatric population; identifying was less sensitive but more found that a CACh they for asthma than a conventional meth¬ specific defining acholine challenge. Such findings could be understood as one range of bronchial responsiveness being divided two by two differently placed borderlines; alternatively, however, these results might again indicate that one is at two somehow related but nevertheless dif¬ looking ferent of bronchial types responsiveness. extent, the observed poor correlation be¬ tween CACh and histamine responses could be a spe¬ cial feature of the studied population. Pediatric asthma To some in or nearing remission could be characterized by a tendency toward positive responses to direct pharma¬In ones to indirect stimuli. cologic stimuli, and negative contrast, currently active asthma could be character¬ ized by positive responses to both direct and indirect stimuli. If this was true, pediatric asthma could be staged by comparing the responses to pharmacologic and nonpharmacologic challenges. Results of the present study, however, do not allow us to draw such conclusions, and further studies, comparing the CACh and histamine responses of patients with clinically ac¬ in tive asthma to those with asthma remission, are needed. When compared with pharmacologic provocations, nonpharmacologic challenges might have several the¬ oretical and practical advantages.24 By applying natu¬ rally occurring stimuli and by activating intermediate events like mediator releases from cells in the airways, challenges might be a more mean¬ nonpharmacologicmodel of hyperreactive airway disease ingful laboratory than the inhalation of bronchoconstrictor substances. Furthermore, such provocations are ethically more acceptableairin epidemiologic work.10 In the case of there is the additional cold-dry ofhyperventilation, a stimulus that is more easily stan¬ advantage using dardized than a bronchoconstrictor aerosol. Such aerosol application of the stimulus is complicated by numerous factors like different nebulizer output, losses in tubing and valves, interindividual differences in breathing pattern and aerosol deposition, etc.2 From a pediatric viewpoint, there are the additional unre- 744 Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21720/ on 05/02/2017 Clinical Investigations solved problems relating to a size correction of air en¬ trapment and aerosol deposition; in fact, these prob¬ lems invalidate any comparison of such response measurements between children of different age and size 27 Such methodologic drawbacks must result in inac¬ and thus illustrate the need to search for alternatives. Of those presently available, single-step CACh is probably the most attractive one. It is brief and thus can be applied accurately to pedi¬ atric patients with limited compliance.3-7 Its relative maximum reaction pla¬ safetyinstems fromwithreaching a and teau patients asthma7 from the lack of any late asthmatic reaction.28 There is some indication that CACh might help identify patients with life-threaten¬ ing asthma.29 The present study adds to this body of that a single-step CACh cannot by showing knowledge for a conventional pharmacologic simply substitute rather measures a specific type of but challenge, bronchial responsiveness. Like any other measure¬ ment of bronchial responsiveness, however, the result of a CACh should be interpreted in relation to the patient's clinical history. 11 Heaton RW, Henderson AF, Costello JF. Cold air as a bronchial provocation technique: reproducibility and comparison with his¬ tamine and methacholine inhalation. Chest 1984; 86:810-14 12 Tessier P, Ghezzo H, L'Archeveque J, et al. Shape of the doseresponse curve to cold air inhalation in normal and asthmatic subjects. Am Rev Respir Dis 1987; 136:1418-23 13 Aquilina AT. Comparison of airway reactivity induced by hista¬ curate measurements References 1 Assoufi BK, Dally MB, Newman-Taylor AJ, et al. Cold air test: a for airway reactivity. Bull Eur Phys¬ simplified standard method Respir 1986; 22:349-57 iopathol 2 Sterk PJ, Fabbri LM, Quanjer PH, et al. Airway responsiveness: standardized challenge testing with pharmacological, physical and sensitizing stimuli in adults. Eur Respir J 1993; 6(suppl 16):53-83 3 McLaughlin FJ, Dozor AJ. Cold air inhalation challenge in the diagnosis of asthma in children. Pediatrics 1983; 72:503-09 4 Tal A, Pasterkamp H, Serrette C, et al. Response to cold air hy¬ perventilation in normal and in asthmatic children. J Pediatr 1984; 104:516-21 dose-response interrelation with a reaction plateau. J Allergy Clin Immunol 1987; 80:9-17 8 Hargreave FE, Ryan G, Thomson NC, et al. Bronchial respon¬ siveness to histamine or methacholine in asthma: measurement and clinical significance. J Allergy Clin Immunol 1981; 68:347-55 9 O'Byrne PM, Ryan G, Morris M, et al. Asthma induced by cold air and its relationship to nonspecific bronchial responsiveness to methacholine. Am Rev Respir Dis 1982; 125:281-85 10 Weiss JW, Rossing TH, McFadden ER, et al. Relationship between bronchial responsiveness to hyperventilation with cold air and methacholine in asthma. J Allergy Clin Immunol 1983; 72:140-44 15 16 17 18 19 1993; 147:565-72 20 Osterreichische Gesellschaft fur Lungenerkrankungen und Tufur klinische Atemphysiologie. berkulose-Arbeitsgemeinschaft Empfehlungen zur standardisierung der inhalativen provokation zur messung der unspezifischen bronchialen reaktivitat. Prax Klin 40:356-64 Pneumol 1986; 21 Cockcroft DW, Killian DN, Mellon JJA, et al. Bronchial reactiv¬ 22 23 ity to inhaled histamine: a method and clinical survey. Clin Allergy 1977; 7:235-43 Quanjer PH, Tammeling GJ, Cotes JE, et al. Lung volumes and forced ventilatory flows: report of working party standardization of lung function tests, European Community for Steel and Coal: official statement of the European Respiratory Society. Eur Respir J 1993; 6(suppl 16):5-40 Hibbert ME, Lannigan A, Landau LJ, et al. Lung function val¬ from a longitudinal study of healthy children and adolescents. Pediatr Pulmonol 1989; 7:101-09 24 Anderson SD, Smith CM. Osmotic challenges in the assessment of bronchial hyperresponsiveness. Am Rev Respir Dis 1991; ues Kump H, et al. Cold air challenge of airway in children: practical application and theoretical hyperreactivity aspects. Pediatr Res 1984; 18:469-78 6 Reisman J, Mappa L, deBenedictis F, et al. Cold air challenge in children with asthma. Pediatr Pulmonol 1987; 3:251-54 7 Zach MS, Polgar G. Cold air challenge of airway hyperreactivity 5 Zach M, Polgar G, in children: 14 mine, methacholine, and isocapnic hyperventilation in normal and asthmatic subjects. Thorax 1983; 38:766-70 Nair N, Hopp RJ, Alper BJ, et al. Correlation of methacholineinduced non-specific bronchial reactivity and cold air hyperven¬ tilation challenge. Ann Allergy 1986; 56:226-28 Filuk RB, Serrette C, Anthonisen NR. Comparison of responses to methacholine and cold air in patients suspected of having asthma. Chest 1989; 95:948-52 Steinbrugger B, Zach M. Bronchiale reaktivitat bei klinisch beschwerdefreien jugendlichen asthmapatienten. Monatsschr Kinderheilkd 1990; 138:389-91 National Heart, Lung and Blood Institute, National Institutes of Health. International consensus report on diagnosis and treat¬ ment of asthma. Eur Respir J 1992; 5:601-41 Zach M, Hadl M. Die kaldufthyperventilationsprovokation. normalwertbereiche einzelner lungenfunktionsparameter im kindesalter. Atemw Lungenkrkh 1987; 7:298-99 Nicolai T, Mutius EV, Reitmeir P, et al. Reactivity to cold-air in normal and in asthmatic children in a survey hyperventilation of 5,697 schoolchildren in southern Bavaria. Am Rev Respir Dis 143:S43-46 25 Pliss LB, Ingenito EP, Ingram RH, et al. Assessment of bron¬ choalveolar cell and mediator response to isocapnic hyperpnea in asthma. Am Rev Respir Dis 1990; 142:73-8 26 Galdes-Sebaldt M, McLaughlin FJ, Levison H. Comparison of cold air, ultrasonic mist, and methacholine inhalations as tests of bronchial reactivity in normal and asthmatic children. J Pediatr 1985; 107:526-30 27 LeSouef PN. Can measurements of airway responsiveness be standardized in children? Eur Respir J 1993; 6:1085-87 28 Varga EM, Eber E, Zach MS. Cold air challenge for measuring airway reactivity in children: lack of a late asthmatic reaction. Lung 1990; 168:267-72 29 Zach MS, Karner U. Sudden death in asthma. Arch Dis Child 1989; 64:1446-51 CHEST /108 / 3 / SEPTEMBER, 1995 Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21720/ on 05/02/2017 745