Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
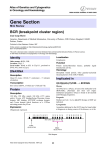
Published OnlineFirst September 8, 2011; DOI: 10.1158/1078-0432.CCR-11-0396 Clinical Cancer Research Cancer Therapy: Clinical See commentary by Smith and Shah, p. 6605 BCR–ABL Transcript Dynamics Support the Hypothesis That Leukemic Stem Cells Are Reduced during Imatinib Treatment Andrew M. Stein1, Dean Bottino2, Vijay Modur1, Susan Branford3, Jaspal Kaeda4, John M. Goldman5, Timothy P. Hughes3, Jerald P. Radich6, and Andreas Hochhaus7 Abstract Purpose: Imatinib induces a durable response in most patients with Philadelphia chromosome–positive chronic myeloid leukemia, but it is currently unclear whether imatinib reduces the leukemic stem cell (LSC) burden, which may be an important step toward enabling safe discontinuation of therapy. In this article, we use mathematical models of BCR–ABL levels to make inferences on the dynamics of LSCs. Experimental Design: Patients with at least 1 BCR–ABL transcript measurement on imatinib were included (N ¼ 477). Maximum likelihood methods were used to test 3 potential hypotheses of the dynamics of BCR–ABL transcripts on imatinib therapy: (i) monoexponential, in which there is little, if any, decline in BCR–ABL transcripts; (ii) biexponential, in which patients have a rapid initial decrease in BCR–ABL transcripts followed by a more gradual response; and (iii) triexponential, in which patients first exhibit a biphasic decline but then have a third phase when BCR–ABL transcripts increase rapidly. Results: We found that most patients treated with imatinib exhibit a biphasic decrease in BCR–ABL transcript levels, with a rapid decrease during the first few months of treatment, followed by a more gradual decrease that often continues over many years. Conclusions: We show that the only hypothesis consistent with current data on progenitor cell turnover and with the long-term, gradual decrease in the BCR–ABL levels seen in most patients is that these patients exhibit a continual, gradual reduction of the LSCs. This observation may explain the ability to discontinue imatinib therapy without relapse in some cases. Clin Cancer Res; 17(21); 1–10. 2011 AACR. Introduction Imatinib is a tyrosine kinase inhibitor (TKI) specifically developed to inhibit BCR–ABL, the oncoprotein encoded by the BCR–ABL fusion gene that results from the reciprocal translocation of chromosomes 9 and 22 (1, 2), which is the hallmark of chronic myeloid leukemia (CML). Despite the high response rates in patients with CML treated with imatinib (3), it is unknown whether responses can be maintained indefinitely after treatment discontinuation in most patients. To safely discontinue therapy, residual long- Authors' Affiliations: 1Novartis Institutes for BioMedical Research, Inc., Cambridge, Massachusetts; 2Novartis Pharmaceuticals Corporation, East Hanover, New Jersey; 3Department of Haematology, SA Pathology, Uni€matologie und Onkologie, versity of Adelaide, Adelaide, Australia; 4Ha €tsmedizin, Charite Virchow Klinikum, Berlin, Germany; 5HaemaUniversita tology Department, Hammersmith Hospital, London, United Kingdom; 6 Clinical Research Division, Fred Hutchinson Cancer Research Center, €matologie/Onkologie, Klinik fu €r Seattle, Washington; and 7Abteilung Ha €tsklinikum Jena, Jena, Germany Innere Medizin II, Universita Note: Supplementary data for this article are available at Clinical Cancer Research Online (http://clincancerres.aacrjournals.org/). Corresponding Author: Andrew M. Stein, Oncology, Novartis Institutes for BioMedical Research, Inc., 45 Sidney St. Cambridge, MA 02139. Phone: 617-256-7600; Fax: 609-981-4102; E-mail: [email protected] doi: 10.1158/1078-0432.CCR-11-0396 2011 American Association for Cancer Research. term leukemic stem cells (LSC) may need to be targeted by the TKI (4). For the purpose of this analysis, LSCs are defined as tumor-initiating cells (i.e., cells that have the capacity for long-term self-renewal and are capable of repopulating all hematopoietic cell compartments). This definition applies regardless of whether the LSCs are derived from normal stem cells or from transformed progenitors (5). Two contrasting sets of data pose a dilemma in understanding the effect of prolonged therapy on LSC populations in CML. First, in vitro experiments suggest that quiescent LSCs are not affected by imatinib, at least not detectably over the 3- to 12-day duration of the experiments (6, 7). In contrast, case reports (8–13) and data from a clinical trial (14) have described successful discontinuation from imatinib treatment after the achievement of low or undetectable levels of BCR–ABL in the blood, suggesting that long-term control of LSCs was obtained. To understand the dynamics of the LSC population over the course of therapy, we modeled responses to imatinib among patients treated on the landmark International Randomized Study of Interferon and STI571 (IRIS) trial. Hematopoiesis is a process in which a relatively small number of stem cells in the bone marrow produce a large number of differentiated blood cells. An analogous process happens in the leukemic cells of patients with CML (Fig. 1; ref. 15). At diagnosis, patients with CML have an unknown www.aacrjournals.org Downloaded from clincancerres.aacrjournals.org on June 17, 2017. © 2011 American Association for Cancer Research. OF1 Published OnlineFirst September 8, 2011; DOI: 10.1158/1078-0432.CCR-11-0396 Stein et al. Translational Relevance With the success of tyrosine kinase inhibitors (TKI) in inducing sustained responses in patients with chronic myeloid leukemia (CML), the question of whether patients can safely discontinue therapy and achieve "cure" has become of paramount importance in the field. Although imatinib induces strong responses in many patients with CML, it is unclear whether it targets leukemic stem cells (LSC), which may be necessary for patients to ultimately discontinue treatment and maintain their response. This article combines mathematical modeling with recent clinical observations of progenitor cell kinetics in the bone marrow to support the hypothesis that patients treated with imatinib exhibit a sustained, gradual reduction of LSCs. This model may explain the sustained responses in many patients after discontinuation of imatinib and may help to identify patients who can safely discontinue TKI therapy. number of LSCs that cycle between a proliferative and a quiescent phase. Some proliferating LSCs differentiate and become early progenitor cells (EPC), which themselves proliferate but no longer have the capacity for long-term self-renewal. After a series of approximately 20 cell divisions, the EPCs become late progenitor cells (LPC), which undergo a series of maturation stages until they become mature leukemic cells that migrate to the blood. It has previously been reported that most patients who undergo imatinib therapy exhibit an initial rapid decline in the BCR–ABL levels, followed by a more gradual decline (16, 17). A number of mathematical models have been developed to explain the BCR–ABL dynamics. Some assume that LSCs are reduced during imatinib therapy (18–20), whereas others argue that the LSCs are not affected (16, 17, 21). In this work, we examine 3 different interpretations of the biphasic BCR–ABL transcript dynamics that are observed in most patients: (i) The proliferating-quiescent hypothesis, in which initial response is due to the loss of proliferating LSCs and long-term responses are due to quiescent LSCs that die upon becoming proliferative (18, 19); (ii) The early stem cell hypothesis, in which initial response is due to death of EPCs and the long-term response is due to the reduction of LSCs that die upon becoming proliferative (22); (iii) The late-early progenitors hypothesis, in which initial response is due to death of LPCs, longterm response is due to death of EPCs, and the LSCs are not significantly depleted during imatinib therapy and may in fact expand (refs. 16, 17; Fig. 2). The 3 hypotheses were originally generated by 3 different modeling groups using IRIS data from their respective cohorts: the proliferatingquiescent model used data from the German cohort (18, 19), the late-early progenitors model used data from the Australian cohort (16, 17), and the early-stem model used data from all IRIS patients who had imatinib blood level concentration measurements (22). The kinetic data analysis makes use of the ratio of BCR– ABL transcripts to that of a control gene (typically BCR or ABL) in peripheral blood (23). We assumed that the BCR– ABL transcript level was directly proportional to the fraction of mature leukemic cells in the blood (24). In an effort to determine the effect of long-term imatinib therapy on LSCs, we used nonlinear mixed effect (NLME) modeling techniques to describe the BCR–ABL dynamics in patients with CML in chronic phase (CML-CP), with 7 years of follow-up on the IRIS study. Each patient was described by 1 of 3 dynamic response models: (i) monophasic patients, who exhibited a gradual BCR–ABL decline at rate m; (ii) biphasic patients, who exhibited an initial rapid BCR–ABL decline at rate a, followed by a more gradual decline at rate b; (iii) triphasic patients, who also exhibited an initial rapid BCR–ABL decline at rate a, followed by a gradual decline at rate b, but then a rapid increase at rate g as the disease relapses. We then used recent measurements of hematopoietic dynamics to make inferences on how the BCR–ABL dynamics relate to changes in the LSC population (Fig. 3 and Supplementary Fig. S1). Materials and Methods Patients and samples Samples for real-time quantitative PCR (RQ-PCR) were collected from peripheral blood: (i) after achievement of complete cytogenetic response (CCyR) in all patients; (ii) at 1, 2, and 3 months and then every 3 months thereafter in a Late progenitor cells Leukemic stem cells LT-HSC ST-HSC Early progenitor cells MPP CMP Self-renewal OF2 Clin Cancer Res; 17(21) November 1, 2011 GMP White blood cells Promonocyte Monocyte Neutrophilic myelocyte Granulocyte Basophilic myelocyte Basophil Figure 1. An illustration of leukemic hematopoiesis and a corresponding compartmental model used to describe it (15). The differential equations for this model are given in the Supplementary Appendix Fig. S2. CMP, common myeloid progenitor; GMP, granulocyte macrophage progenitor; LT-HSC, long-term hematopoietic stem cell; MPP, multipotent progenitor; ST-HSC, short-term hematopoietic stem cell. Clinical Cancer Research Downloaded from clincancerres.aacrjournals.org on June 17, 2017. © 2011 American Association for Cancer Research. Published OnlineFirst September 8, 2011; DOI: 10.1158/1078-0432.CCR-11-0396 BCR–ABL Transcript Dynamics on Imatinib A β PQ hypothesis α ~ decline of LSC-Ps β ~ decline of LSC-Qs LSC-Q LSC-P EPC LPC WBC EPC LPC WBC LPC WBC α β B ES hypothesis α ~ decline of EPCs β ~ decline of LSCs LSC-Q LSC-P α C LE hypothesis α ~ decline of LPCs β ~ decline of EPCs LSCs untouched LSC-Q LSC-P EPC β α Figure 2. A summary of 3 hypotheses for the biphasic response, in which each hypothesis is explored by using a different parameter set in the same structural model. A, the proliferating quiescent (PQ) model assumes the LSCs themselves undergo a biphasic decline due to LSCs transitioning between 2 states, proliferative (LSC-P) and quiescent (LSC-Q), such that they are only vulnerable to imatinib therapy in their proliferative state (18, 19). B, the early-stem (ES) model assumes the initial response is due to rapid killing of the EPCs and the long-term response is due to a depletion of the LSCs (22). C, the late-early progenitors (LE) hypothesis (17, 46, 47) assumes that the death rate of the progenitor pool is itself biphasic under imatinib treatment and the LSCs are not depleted at all (17, 46). gene), the U.K. measurement was used]. In all other cases, the measurement of minimum value was used, consistent with previous analyses (30–32). The effective range for the IS is BCR–ABL (IS) 10% (23). This upper limit is due to 2 sources of nonlinearity in the BCR–ABL ratio estimation: (i) Depending upon the primer design for the ABL control gene, both ABL and BCR–ABL are amplified when the BCR–ABL levels are high (33); (ii) An additional nonlinearity occurs for both the BCR and ABL control genes because healthy cells have 2 copies of the control gene (e.g., ABL), whereas leukemic cells have subpopulation of patients treated in Germany (25); (iii) every 3 months in subpopulations of patients treated in Australia and New Zealand; and (iv) at the discretion of physicians before achievement of CCyR. All RQ-PCR (BCR– ABL/control gene 100%) measurements were then converted to the international scale (IS) for BCR–ABL transcripts (23, 26–29). When multiple measurements existed within a 3-month interval, we followed the IRIS analysis protocol for choosing a single unique measurement [i.e., when one measurement was carried out at the U.K. lab (BCR control gene) and the other at the German lab (ABL control A B 2 2 µ´ 0 10 -2 10 BCR–ABL (IS)% BCR–ABL (IS)% 10 α´ 0 10 β´ -2 10 4 Time (y) 6 8 ү´ 10 0 2 4 Time (y) D 6 8 0 2 4 6 Time (y) 8 E 2 2 10 10 BCR–ABL (IS)% 2 BCR–ABL (IS)% 0 α´ 0 10 -2 10 α´ 0 10 0 10 -2 -2 10 10 0 www.aacrjournals.org C 2 10 BCR–ABL (IS)% Figure 3. BCR–ABL (IS)% for all 477 patients in this analysis, divided into 5 groups with an example patient highlighted within each group. A, slow-monophasic patients (n ¼ 44). B, fast-biphasic patients (n ¼ 282). C, fast-triphasic patients (n ¼ 14). D, fast-unknown (n ¼ 68). E, unknown (n ¼ 69). The asterisks ( ) indicate when a BCR– ABL (IS)% measurement fell below 0.0032, the approximate limit of quantification of the assay for all labs in the IRIS. The prime (0 ) symbol after the model parameters (m, a, b, and g) denotes that the slopes in the graph are the model parameters multiplied by the constant log10 e ¼ 0.43 (e.g., m0 ¼ 0.43 m). 2 4 Time (y) 6 8 0 2 4 Time (y) 6 8 Clin Cancer Res; 17(21) November 1, 2011 Downloaded from clincancerres.aacrjournals.org on June 17, 2017. © 2011 American Association for Cancer Research. OF3 Published OnlineFirst September 8, 2011; DOI: 10.1158/1078-0432.CCR-11-0396 Stein et al. 1 control gene and 1 BCR–ABL gene. In that case, even if the expression rates of ABL and BCR–ABL are equal, the BCR– ABL/ABL ratio is equal to L/(L þ 2H), in which L is the number of leukemic white blood cells (WBC) and H is the number of healthy WBCs. Because both L and H change with time, and BCR–ABL and ABL expression and amplification levels are not necessarily identical, there is no simple transformation that can be applied to remove this nonlinearity. Thus, although measurements above 10% are included in this analysis so that we can describe the full range of BCR–ABL dynamics for all patients, we emphasize that quantitative values of the parameters governing the dynamics at the start of treatment (A, a, m) should be used only in a qualitative fashion. Cell populations were described according to the presence of cell surface markers. We assumed proportional relationships between LSCs and CD34þ/CD38 cells, between EPCs and CD34þ/CD38þ cells, and between LPCs and CD38 cells. Model selection and parameter fitting In this analysis, we employed NLME modeling methodology, as is the recommended practice in developing population models of clinical data (34, 35). This approach is specifically designed to make maximal use of all available data and to handle sparse data without introducing biases. Therefore, all patients with at least 1 data point were included in the initial model-fitting analysis. Using Monolix (www.monolix.org, version 3.1) NLME software in Matlab (The MathWorks), we used maximum likelihood methods to fit the following mixture model to the log10 of the BCR– ABL dynamics R(t) once treatment begins at t ¼ 0: 8 log10 ðAemt Þ þ "; > > > > > monoexponential; with probability p1 > > > at bt > > log < 10 ðAe þ Be Þ þ "; biexponential ðtypical responseÞ; with probability p2 RðtÞ ¼ > > at bt gt > log > 10 ðAe þ Be þ Ce Þ þ "; > > > > > triexponential ðsecondary resistanceÞ; > : with probability p3 An additional strength of the NLME mixture-modeling approach is that all parameters (A, B, C, m, a, b, g, e, p1, p2, p3 ¼ 1 p1 p2) can be fit to the entire patient population simultaneously. The model represents 3 typical profiles: (i) monoexponential, in which there was little, if any, decline in BCR–ABL (IS)% at a rate m 0; (ii) biexponential, in which patients had a rapid initial decrease (a) in the BCR– ABL (IS)% followed by a more gradual response (b), which could be either increasing or decreasing; and (iii) triexponential, in which patients first exhibit a biphasic decline but then have a third phase when the BCR–ABL (IS)% increases rapidly with rate g > 0. The constant terms (A, B, C) are unitless and are restricted to be greater than zero because BCR–ABL (IS)% is always positive. Baseline BCR–ABL levels were approximately equal to the A parameter. In the limiting case that a patient had only a OF4 Clin Cancer Res; 17(21) November 1, 2011 single measurement at baseline, data from that patient informed the population average of the baseline measurement but did not influence the other parameter estimates. The rate constants (m, a, b, and g) have units of 1 per year. Before treatment starts, the BCR–ABL (IS)% is constant and equal to its initial value at t ¼ 0. Each model has an additive residual error term, e, that describes variability in the measurement due to assay variability, interoccasion variability, and model error. Due to limits of quantification of the PCR assay, we chose 0.0032% [a 4.5-log10 decrease in the BCR–ABL (IS)%] as the minimal level of detection of the assay for all labs and treated these measurements as left-censored data. In the original IRIS study, this was the limit at which a patient was defined as having achieved an undetectable number of BCR–ABL transcripts, defined as a complete molecular remission (CMR; ref. 32). This value has subsequently been used in other studies and is the desired limit of detection, although not always achievable because of differences in sample quality. Rather than remove all measurements below the limit of quantification or fix them at a certain value, we used a maximum likelihood approach, treating any measurement falling below the limit of detection as having an upper boundary of 0.0032%. This approach, referred to as method 3 (36), allows us to make optimal use of the measurements that fall below the limit of quantification. The patient population was then divided into 5 categories as shown in Fig. 3 and Supplementary Fig. S1. Three categories were based on the model categorization above (slow monophasic, fast biphasic, and fast triphasic). However, if a patient had only 1 data point, fewer than 2 months of follow-up, or no data in the first 2 years, the patient was classified as unknown. If a patient had fewer than 4 years of follow-up and was classified as biexponential by the model, we noted that the patient may in fact be triexponential; however, they were not followed long enough to detect the third phase. Therefore, patients with a fast response and fewer than 4 years of follow-up were classified as fast unknown because it was unknown whether they were biphasic or triphasic. As few as 2 data points were sufficient to classify many patients. For example, a baseline measurement of 100% followed by a 6-month measurement of 90% was indicative of slow-monophasic dynamics, whereas a 6month measurement of 1% indicated a fast initial response. To investigate whether there is a relationship between response category and clinical effect, we looked for differences in event-free survival (EFS) among 4 response categories (excluding those patients without sufficient data for classification). EFS was defined as the time between randomization and any of the following events on treatment: death because of any cause, progression to accelerated phase or blast crisis, increase in WBCs, loss of complete hematologic response, and loss of major cytogenetic response (37). The time was censored at the date of last assessment (hematology, extramedullary disease, or cytogenetic evaluation) Clinical Cancer Research Downloaded from clincancerres.aacrjournals.org on June 17, 2017. © 2011 American Association for Cancer Research. Published OnlineFirst September 8, 2011; DOI: 10.1158/1078-0432.CCR-11-0396 BCR–ABL Transcript Dynamics on Imatinib Results Of the 553 patients receiving imatinib at the start of treatment on the IRIS study, 477 had at least 1 BCR–ABL transcript measurement and were included in the analysis. BCR–ABL was measured for a median of 6.4 years, with a median of 8 data points for each patient. Of the 477 patients on the IRIS trial with at least 1 BCR– ABL measurement, 282 (59%) were classified as biphasic, 44 (9%) as shallow monophasic, and 14 (3%) as triphasic; 68 patients (14%) were fast responders but of undetermined type, and 69 patients (14%) had insufficient data for classification. The BCR–ABL transcript dynamics according to the IS for all patients, along with fits to representative patients in each category, are shown in Fig. 3. Histograms of the rate constants m, a, b, and g are plotted in Fig. 4. The median and the upper and lower quartiles of the NLME model parameters are reported in the Supplementary Appendix Table S1. The EFS outcomes of the 4 groups are summarized in Fig. 5. The biphasic patients had significantly better EFS than all other groups (P < 0.0001). In particular, only 10 of 282 (4%) biphasic patients experienced an event and 6 died for reasons unrelated to the disease. Of the 68 patients with Number of patients A 250 200 Fast (α) 89.2% (364/408) 150 100 50 Slow (μ) 10.8% (44/408) 0 0.1 1 10 100 Time (1/y) B Number of patients 140 Fast unknown (β) 18.7% (68/364) 120 100 80 60 40 Fast biphasic (β) 77.5% (282/364) 20 0 -1 0 1 2 Fast triphasic (γ) 3.8% (14/364) 3 4 5 Time (1/y) Figure 4. Distribution of patients for the A, initial reduction rate (m, a rate constants; n ¼ 408) and B, long-term BCR–ABL (IS)% dynamics (b and g rate constants; n ¼ 364). www.aacrjournals.org 1 Fast biphasic Probability of EFS for patients without an event. The relationship between the response category and EFS was then determined using a x2 2-sample test. 0.8 Unknown 0.6 Fast unknown 0.4 Slow monophasic Fast triphasic 0.2 0 0 1 2 3 4 5 6 7 8 Time (y) Figure 5. EFS according to patient group (P < 0.0001 for the comparison between fast-biphasic and all other categories). a fast-unknown response, 17 (25%) had an event. In contrast, 25 of 44 (57%) monophasic patients and 9 of 14 (64%) triphasic patients experienced an event. We also explored whether the a and b slopes were predictive of response by comparing the event rates of biphasic patients in the top and bottom quartiles in a and b using a log-rank test. The difference in survival was not significant for a (P ¼ 0.22), whereas the same comparison for b gave a significant difference (P ¼ 0.02). Among the entire patient population, a rapid initial response did correlate with improved outcome because the rapid responders excluded the slow-monophasic patients by definition. Among the rapid responders (biphasic and triphasic patients), however, a steeper a did not correlate with improved outcome. Given the ability of the model to subdivide the patient population into groups with very different outcomes, we next explored the biological interpretation of the model. The monophasic patients often exhibit primary resistance, though a small number of slow-monophasic patients do exhibit a slow, gradual decrease in BCR–ABL transcript levels over the course of therapy and obtain a CCyR. Only 17 of 44 monophasic patients (39%) achieved a CCyR on imatinib, and 39 (89%) either experienced an event or discontinued therapy because of an unsatisfactory response. The triphasic patients correspond to those exhibiting secondary resistance to imatinib, which is defined by the achievement and then loss of response. The third exponential (g) corresponds to an exponentially growing population of cells that do not respond to imatinib treatment. Although 12 of 14 triphasic patients (86%) achieved a CCyR, 14 (100%) experienced an event or discontinued therapy because of an unsatisfactory response. Finally, the biphasic patients, as described above, exhibited a superior response on imatinib. There are many possible interpretations of the biphasic response, which we explored. To interpret how b relates to leukemic hematopoiesis, particularly in biphasic patients, we considered 3 hypotheses described previously as the proliferating-quiescent, early-stem, and late-early progenitors hypotheses (Fig. 2). The 3 hypotheses are described with a single structural Clin Cancer Res; 17(21) November 1, 2011 Downloaded from clincancerres.aacrjournals.org on June 17, 2017. © 2011 American Association for Cancer Research. OF5 Published OnlineFirst September 8, 2011; DOI: 10.1158/1078-0432.CCR-11-0396 Stein et al. A number of experimental observations indicate that the EPCs are depleted on the faster (a) time scale, supporting the early-stem and proliferating-quiescent models over the late-early progenitors model, which predicts that EPCs decay on the slower (b) time scale. In healthy subjects, it takes approximately 5 days to mature from a myeloblast (the most immature differentiated cell) to the last myelocyte (the most mature hematopoietic cell that undergoes mitosis) and approximately 6.6 days to go from a myelocyte to a mature blood cell (38, 39). Furthermore, of the 9 patients with CML on imatinib therapy studied by Abe and colleagues (40), 7 exhibited a rapid depletion of EPCs to undetectable levels within the first 18 months of treatment. The remaining 2 patients had only 2 measurements, with 1 at baseline and 1 at year 4, and thus the BCR–ABL dynamics in the first year cannot be estimated. The 3 different models are depicted graphically alongside the data from Abe and colleagues (40) in Fig. 6, in which it is seen that the EPC kinetics are most consistent with the early-stem and proliferating-quiescent models, but not the late-early progenitors model. This evidence strongly suggests that EPC dynamics operate on time scales of weeks, which supports the early-stem and proliferating-quiescent hypotheses, both of which predict a long-term depletion of the LSCs. For all 3 models, the long-term dynamics of the WBCs (and in fact all progenitor compartments) will be parallel to model, with each hypothesis represented by a different set of parameter values. Although all 3 models exhibit the observed biphasic BCR–ABL response trajectories, the models make different assumptions in terms of LSC dynamics under imatinib treatment. The proliferating-quiescent model assumes that depletion of proliferating and quiescent stem cells, respectively, drive the a and b slopes of BCR–ABL decline. The early-stem model assumes that depletion of EPCs and stem cells drive the a and b slopes, respectively. Finally, the late-early progenitors model assumes that there is no significant LSC depletion with imatinib therapy and that the a and b slopes correspond instead to depletion of the LPCs and EPCs, respectively. The choice of parameters for each model and the corresponding equations are described in more detail in the Supplementary Appendix. As a consequence of adjusting the biological parameters of each model to fit the observed biphasic trajectories, the models make different predictions with respect to EPC kinetics. In particular, the late-early progenitors model predicts that EPCs have a half-life of approximately 180 days, corresponding to the b slope, whereas the early-stem and proliferating-quiescent models predict a much shorter half-life of 5 to 17 days, corresponding to the a slope. As the models make different predictions, we can use experimental observations on EPC kinetics to distinguish between the late-early progenitors, early-stem, and proliferating-quiescent models. Model/data comparison 100 Monophasic, decreasing -2 10 C LE hypothesis α ~ decline of LPCs β ~ decline of EPCs LSCs untouched EPC/LPC % LSC/(LSC+HSC) 0 2 4 102 101 100 Monophasic, increasing 10-1 10-2 0 2 Time (y) 4 WBC BCR–ABL (IS)% 10-1 10-2 0 4 102 101 10-1 100 2 102 101 100 10-1 -2 10 0 2 4 102 101 100 10-1 10-2 0 2 Time (y) WBCs 102 101 100 10-1 10-2 4 WBC BCR–ABL (IS)% LSC-P/EPC % LSC/(LSC+HSC) ES hypothesis α ~ decline of EPCs β ~ decline of LSCs 2 EPCs 102 101 WBC BCR–ABL (IS)% Biphasic, decreasing 10-2 EPC BCR–ABL (IS)% 10-1 0 B EPC BCR–ABL (IS)% 100 EPC BCR–ABL (IS)% A PQ hypothesis α ~ decline of LSC-Ps β ~ decline of LSC-Qs LSC-Q/LSC-P % LSC/(LSC+HSC) LSCs 102 101 4 0 2 4 0 2 4 0 2 Time (y) 4 102 101 100 10-1 10-2 102 101 100 10-1 10-2 Figure 6. Comparison between the mathematical models and patient data (from Abe and colleagues; ref. 40; N ¼ 9). Note that the late-early progenitors (LE) hypothesis, in which LSCs are not affected by imatinib, does not match the observed EPC dynamics. The EPCs plotted are granulocyte macrophage þ þ þ þ progenitors, characterized by the cell surface markers CD34 CD38 IL-3Ra CD45RA Lin . ES, early-stem; LSC-P, proliferating LSC; LSC-Q, quiescent LSC; PQ, proliferating-quiescent; HSC, hematopoietic stem cell. OF6 Clin Cancer Res; 17(21) November 1, 2011 Clinical Cancer Research Downloaded from clincancerres.aacrjournals.org on June 17, 2017. © 2011 American Association for Cancer Research. Published OnlineFirst September 8, 2011; DOI: 10.1158/1078-0432.CCR-11-0396 BCR–ABL Transcript Dynamics on Imatinib the long-term dynamics of the LSCs. In the proliferatingquiescent and early-stem models, the gradual decay of the LSCs is matched by a gradual decay in the WBCs and EPCs after year 1. In the late-early model, the leukemic WBC and EPC levels will eventually plateau after year 4. This property—that the more mature cell population dynamics parallel the LSC dynamics after sufficient treatment duration— is true for any generic model of hematopoiesis (Supplementary Appendix) and reflects the fundamental observation that all leukemic cells ultimately arise from LSCs. Thus, although residual progenitor cells are also detected after many years of continuous imatinib therapy (41), the models and the data from Abe and colleagues (40) suggest that these progenitors arise from persistent LSCs, rather than that particular progenitor cells persist in the bone marrow for years. Therefore, under constant therapy, after long durations, WBC dynamics serve as a surrogate measure for LSC dynamics. In the biphasic patient subset from the IRIS study presented above, 90% of patients were found to have b above 0.69 per year (Fig. 4B), meaning that the half-life of the slowest observable compartment was more than 1 year. We show above that this half-life is too long to describe the EPCs. Therefore, the gradual rate of decay (b) in BCR–ABL must correspond to an earlier hematopoietic population of cells with the capacity to persist in the bone marrow for many years. The only cells with the ability to persist in the bone marrow for many years are the LSCs. Therefore, we deduced that the gradual rate of reduction of the BCR–ABL (b) is best explained by a reduction of the LSCs. Discussion We used maximum likelihood methods to fit 3 different exponential functions to the BCR–ABL (IS)% data set for 477 patients with Philadelphia chromosome–positive (Phþ) CML-CP in the imatinib arm of the IRIS trial, with an average follow up of 7 years. Most patients (282 of 477; 59%) with Phþ CML-CP were best described by a biexponential model consisting of 2 slopes: an a slope, corresponding to the rapid initial decrease in the BCR–ABL transcripts at the start of treatment, and a b slope, corresponding to the long-term BCR–ABL transcript dynamics. A second population (44 of 477 patients; 9%) was best described by a gradual monoexponential model with little or no initial decrease in transcript levels, corresponding to primary resistance or minor response to imatinib. Finally, 14 of 477 patients (3%) were best described by a triexponential model, corresponding to an initial biphasic decline followed by a third increasing phase, which would be clinically described as molecular relapse, likely due to acquired resistance to imatinib. We note that 69 of 477 patients (14%) did not have sufficient data for classification and that 68 of 477 (14%) could only be classified as having a fast initial response, but whether they were biphasic or triphasic could not be determined. We argue that in those patients well described by the biexponential model, a gradual decline of LSCs during www.aacrjournals.org imatinib treatment is the only hypothesis that can explain (i) the observed gradual decline in the number of BCR–ABL transcripts in peripheral blood and (ii) known time scales of EPCs. The alternative explanation (late-early progenitors hypothesis; ref. 17) is that a population of progenitor cells persists in the marrow for many years, but this hypothesis cannot simultaneously explain (i) and (ii). We emphasize that although we use the 3 models to illustrate the different biological hypotheses for the a and b slopes, the main conclusion—that the LSCs are the only population of leukemic cells that have the ability to persist in the bone marrow for years and thus contribute to the gradual b slope—is model-independent (Supplementary Appendix). In the original paper, in which the late-early progenitors hypothesis was proposed, 2 observations were provided that supported the lack of depletion of the LSCs: (i) Three patients received imatinib for at least 1 year and all relapsed rapidly upon halting treatment, and (ii) in vitro, LSCs are resistant to imatinib on short-time scales (17). Rapid relapse upon discontinuation, however, occurs in all 3 models and, therefore, is not necessarily a function of lack of effect on LSCs (Supplementary Appendix Fig. S3). Furthermore, this work addresses LSC dynamics over many years of treatment, whereas the in vitro experiments that show no effect of imatinib on LSCs (6, 7) represent only a few days of treatment. Although our modeling approach can fit existing data to infer LSC kinetics over a long course of therapy, it provides little insight into the mechanisms underlying the stem cell depletion. It may be that in vivo LSCs are slightly susceptible to imatinib treatment but only over long time periods, which would explain why this susceptibility is not observed in vitro (6, 7). It may also be that other mechanisms for LSC depletion, not active in vitro, contribute to the decline, such as an immune response (42, 43) or competition of LSCs with residual normal hematopoietic stem cells for a limited number of niches (19). One potential limitation of this study is the simplified definitions of stem cells that were used. Although it is common practice, defining stem cells according to cell surface markers is imprecise. For example, not all CD34þ/ CD38 cells are able to reconstitute an immune system or generate a colony-forming unit. However, Abe and colleagues (40) evaluated the dynamics of several different subpopulations of progenitor cells (granulocyte–macrophage progenitors characterized by the cell surface markers CD34þCD38þIL-3RaþCD45RAþLin; common myeloid progenitors characterized by CD34þCD38þIL3RaþCD45RA Lin ; and megakaryocyte/erythroid progenitors characterized by CD34 þCD38 þIL3RaCD45RALin), and although our focus was on the granulocyte–macrophage progenitors, the dynamics of all 3 populations were similar. The model described here is a simplification of LSC biology. For example, it is possible for differentiated hematopoietic cells to become less differentiated, and proliferating leukemic cells can asymmetrically divide to produce quiescent leukemic cells or more differentiated cells. These phenomena were not Clin Cancer Res; 17(21) November 1, 2011 Downloaded from clincancerres.aacrjournals.org on June 17, 2017. © 2011 American Association for Cancer Research. OF7 Published OnlineFirst September 8, 2011; DOI: 10.1158/1078-0432.CCR-11-0396 Stein et al. included in the current model because the purpose of this model was to illustrate the basic differences between the existing hypotheses about the effect of imatinib on LSCs. The conclusions from this work can be generalized to more sophisticated models that more accurately capture LSC dynamics. The CML cell population is genetically heterogeneous. Thus, b only provides an estimate for the depletion rate of the most resistant, but still observable, population of LSCs. In some patients, there may still be a small population of LSCs in the marrow that is driven to quiescence under imatinib treatment. Persistently quiescent LSCs may remain undetectable with reverse transcriptase PCR based on BCR– ABL transcripts, and it may be cells such as these that account for rapid relapse in patients who discontinue imatinib years after achieving undetectable levels of BCR–ABL. Although both the early-stem and proliferating-quiescent hypotheses predict that the b slope is due to LSC depletion, they differ in their explanation for the initial BCR–ABL decline (a); the early-stem hypothesis attributes a to EPCs, and the proliferating-quiescent hypothesis attributes a to a decline in the proliferating LSCs. Further modeling work and experimental observations may be necessary to distinguish between the 2 models. The implications of this work are that b may be predictive of the curative potential of TKI therapy. This analysis predicts that a steeper b at the time a patient achieves CMR (defined as undetectable BCR–ABL) correlates with a better chance of maintaining a durable response once treatment is discontinued. The model also predicts that, after achieving CMR, patients with a more gradual b should continue treatment for a longer duration before discontinuation. For example, consider 2 patients who achieve CMR at the same time, in which patient 1 has a long-term response with b ¼ 1 per year and patient 2 has a steeper response with b ¼ 2 per year. The model predicts that patient 1 would need to continue therapy for twice as long as patient 2 to have the same likelihood of maintaining a durable response upon discontinuation. Testing of these hypotheses will require an analysis of discontinuation trials in which BCR–ABL time course of the patients is reported from initiation of therapy. The mathematical modeling literature has made different predictions for when a typical patient with CML may be expected to achieve a "cure." Roeder and Glauche (44) estimated that most patients will require 20 years to achieve LSC eradication, whereas Lenaerts and colleagues (21) predicted that the majority of patients will achieve eradication of minimal residual disease within 5 years on TKI therapy. In our view, the discrepancy between current models of LSC dynamics indicates that much is still unknown about the hematopoietic dynamics of leukemia and that further clinical trials will be necessary to understand how a model might provide further insight into discontinuation studies. Because there are numerous models that well describe BCR–ABL dynamics in CML, the ability of a model to fit existing data is not validation of the model but, rather, a OF8 Clin Cancer Res; 17(21) November 1, 2011 demonstration that the model is one potential quantitative hypothesis for describing the known data. When models lead to conflicting hypotheses, additional observations are required. In this work, we have integrated existing models with recent measurements of EPC dynamics. In summary, we modeled the transcript numbers measured in 477 patients in the imatinib arm of the IRIS trial. We found that a biexponential curve best described most of the patient population. The patient response over 7 years is well described with 2 slopes: an a slope corresponding to the rapid initial decrease in BCR–ABL transcript levels after the start of treatment, and the b slope corresponding to the long-term BCR–ABL dynamics. Using recent measurements of the EPC dynamics, in combination with known biology of healthy hematopoiesis, we find that the most likely biological interpretation of the b slope is that it corresponds to the change in the LSC population. We believe that this model is the simplest model that best describes the patient population. This model may eventually be useful in interpreting data with second-generation BCR–ABL inhibitors and quantifying patient progress toward eradication of CML. We are currently evaluating the molecular response dynamics in patients treated with nilotinib, an agent that may be more likely to induce "cure" in patients, based on the faster and deeper molecular responses observed in newly diagnosed patients treated with nilotinib versus imatinib (45). Disclosure of Potential Conflicts of Interest S. Branford received research support and honoraria from Novartis and Bristol-Myers Squibb; J.M. Goldman received honoraria from and participated in speakers’ bureaus for Novartis and Bristol-Myers Squibb; T.P. Hughes received research funding from Novartis and Bristol-Myers Squibb, received honoraria from Novartis, Bristol-Myers Squibb, and Ariad, and participated in speakers’ bureaus for Novartis; J.P. Radich acted as a consultant for and received honoraria from Novartis and Bristol-Myers Squibb, and received research funding from Novartis; and A. Hochhaus received research support from Novartis. The other authors disclosed no potential conflicts of interest. Acknowledgments The authors thank Yen-Lin Chia, Ovidiu Chiparus, Jim Dunyak, Insa Gathmann, Alan Hatfield, Gabriel Helmlinger, Tillmann Krahnke, Jerry Nedelman, Elke Ortmann, and Elisabeth Wehrle for many useful discussions. The authors also thank Erinn Goldman for medical editorial assistance with this article and, finally, Thea Kalebic for initiating and continually supporting the application of modeling and simulation to optimize the treatment of CML. Grant Support Financial support for medical editorial assistance was provided by Novartis Pharmaceuticals Corporation. A. Hochhaus was supported by the Bundesministerium f€ ur Bildung und Forschung (BMBF), Germany, grant no. Haematosys 0315452D. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. Received February 11, 2011; revised July 19, 2011; accepted August 19, 2011; published OnlineFirst September 8, 2011. Clinical Cancer Research Downloaded from clincancerres.aacrjournals.org on June 17, 2017. © 2011 American Association for Cancer Research. Published OnlineFirst September 8, 2011; DOI: 10.1158/1078-0432.CCR-11-0396 BCR–ABL Transcript Dynamics on Imatinib References 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. Shtivelman E, Lifshitz B, Gale RP, Canaani E. Fused transcript of Abl and Bcr genes in chronic myelogenous leukaemia. Nature 1985;315:550–4. Groffen J, Stephenson JR, Heisterkamp N, de Klein A, Bartram CR, Grosveld G. Philadelphia chromosomal breakpoints are clustered within a limited region, Bcr, on chromosome 22. Cell 1984;36:93–9. Deininger M, O'Brien SG, Guilhot F, Goldman JM, Hochhaus A, Hughes TP, et al. International randomized study of interferon vs STI571 (IRIS) 8-year follow up: sustained survival and low risk for progression or events in patients with newly diagnosed chronic myeloid leukemia in chronic phase (CML-CP) treated with imatinib. Blood 2009;114:462. Abstr 1126. Stuart SA, Minami Y, Wang JY. The CML stem cell: evolution of the progenitor. Cell Cycle 2009;8:1338–43. Zhou BB, Zhang H, Damelin M, Geles KG, Grindley JC, Dirks PB. Tumour-initiating cells: challenges and opportunities for anticancer drug discovery. Nat Rev Drug Discov 2009;8:806–23. Graham SM, Jørgensen HG, Allan E, Pearson C, Alcorn MJ, Richmond L, et al. Primitive, quiescent, Philadelphia-positive stem cells from patients with chronic myeloid leukemia are insensitive to STI571 in vitro. Blood 2002;99:319–25. Graham SM, Vass JK, Holyoake TL, Graham GJ. Transcriptional analysis of quiescent and proliferating CD34þ human hemopoietic cells from normal and chronic myeloid leukemia sources. Stem Cells 2007;25:3111–20. Guastafierro S, Falcone U, Celentano M, Coppola M, Ferrara MG, Sica A. Is it possible to discontinue imatinib mesylate therapy in chronic myeloid leukemia patients with undetectable BCR/ABL? A case report and a review of the literature. Leuk Res 2009;33:1079–81. Mauro MJ, Druker BJ, Maziarz RT. Divergent clinical outcome in two CML patients who discontinued imatinib therapy after achieving a molecular remission. Leuk Res 2004;28 Suppl 1:S71–3. Cortes J, O'Brien S, Kantarjian H. Discontinuation of imatinib therapy after achieving a molecular response. Blood 2004;104:2204–5. Ali R, Ozkalemkaş F, Ozçelik T, Ozkocaman V, Ozan U, Kimya Y, et al. Pregnancy under treatment of imatinib and successful labor in a patient with chronic myelogenous leukemia (CML): outcome of discontinuation of imatinib therapy after achieving a molecular remission. Leuk Res 2005;29:971–3. Merante S, Orlandi E, Bernasconi P, Calatroni S, Boni M, Lazzarino M. Outcome of four patients with chronic myeloid leukemia after imatinib mesylate discontinuation. Haematologica 2005;90:979–81. Goh HG, Kim YJ, Kim DW, Kim HJ, Kim SH, Jang SE, et al. Previous best responses can be re-achieved by resumption after imatinib discontinuation in patients with chronic myeloid leukemia: implication for intermittent imatinib therapy. Leuk Lymphoma 2009;50:944–51. a D, Guilhot J, Guilhot F, Huguet F, Nicolini F, et al. Mahon FX, Re Discontinuation of imatinib in patients with chronic myeloid leukaemia who have maintained complete molecular remission for at least 2 years: the prospective, multicentre stop imatinib (STIM) trial. Lancet Oncol 2010;11:1029–35. €secke J, Libra M, Misaghian N, Ligresti G, Steelman LS, Bertrand FE, Ba et al. Targeting the leukemic stem cell: the holy grail of leukemia therapy. Leukemia 2009;23:25–42. Dingli D, Michor F. Successful therapy must eradicate cancer stem cells. Stem Cells 2006;24:2603–10. Michor F, Hughes TP, Iwasa Y, Branford S, Shah NP, Sawyers CL, et al. Dynamics of chronic myeloid leukaemia. Nature 2005;435:1267–70. Komarova NL, Wodarz D. Effect of cellular quiescence on the success of targeted CML therapy. PLoS One 2007;2:e990. Roeder I, Horn M, Glauche I, Hochhaus A, Mueller MC, Loeffler M. Dynamic modeling of imatinib-treated chronic myeloid leukemia: functional insights and clinical implications. Nat Med 2006;12:1181–4. Wodarz D. Heterogeneity in chronic myeloid leukaemia dynamics during imatinib treatment: role of immune responses. Proc Biol Sci 2010;277:1875–80. Lenaerts T, Pacheco JM, Traulsen A, Dingli D. Tyrosine kinase inhibitor therapy can cure chronic myeloid leukemia without hitting leukemic stem cells. Haematologica 2010;95:900–7. www.aacrjournals.org 22. Bottino D, Chia Y, Stein A, Georgieva A, Yu J, Kahn J, et al. Inference of imatinib (IM) effects on leukemic stem cell (SC) compartment via mathematical modeling of IRIS treatment response data [abstract]. J Clin Oncol 2009;27:7056. €ller MC, Hochhaus A, Kim DW, 23. Branford S, Fletcher L, Cross NC, Mu et al. Desirable performance characteristics for BCR–ABL measurement on an international reporting scale to allow consistent interpretation of individual patient response and comparison of response rates between clinical trials. Blood 2008;112:3330–8. 24. Branford S, Hughes TP, Rudzki Z. Monitoring chronic myeloid leukaemia therapy by real-time quantitative PCR in blood is a reliable alternative to bone marrow cytogenetics. Br J Haematol 1999;107: 587–99. €ller MC, Gattermann N, Lahaye T, Deininger MW, Berndt A, Frue25. Mu hauf S, et al. Dynamics of BCR–ABL mRNA expression in first-line therapy of chronic myelogenous leukemia patients with imatinib or interferon alpha/ara-C. Leukemia 2003;17:2392–400. 26. Hughes T, Deininger M, Hochhaus A, Branford S, Radich J, Kaeda J, et al. Monitoring CML patients responding to treatment with tyrosine kinase inhibitors: review and recommendations for harmonizing current methodology for detecting BCR–ABL transcripts and kinase domain mutations and for expressing results. Blood 2006;108:28–37. 27. Branford S, Cross NC, Hochhaus A, Radich J, Saglio G, Kaeda J, et al. Rationale for the recommendations for harmonizing current methodology for detecting BCR–ABL transcripts in patients with chronic myeloid leukaemia. Leukemia 2006;20:1925–30. 28. Branford S. Chronic myeloid leukemia: molecular monitoring in clinical practice. Hematology Am Soc Hematol Educ Program 2007:376–83. €ller MC, Erben P, Saglio G, Gottardi E, Nyvold CG, Schenk T, et al. 29. Mu Harmonization of BCR–ABL mRNA quantification using a uniform multifunctional control plasmid in 37 international laboratories. Leukemia 2008;22:96–102. 30. Druker BJ, Guilhot F, O'Brien SG, Gathmann I, Kantarjian H, Gattermann N, et al. Five-year follow-up of patients receiving imatinib for chronic myeloid leukemia. N Engl J Med 2006;355:2408–17. 31. Hochhaus A, O'Brien SG, Guilhot F, Druker BJ, Branford S, Foroni L, et al. Six-year follow-up of patients receiving imatinib for the firstline treatment of chronic myeloid leukemia. Leukemia 2009;23: 1054–61. 32. Hughes TP, Kaeda J, Branford S, Rudzki Z, Hochhaus A, Hensley ML, et al. Frequency of major molecular responses to imatinib or interferon alfa plus cytarabine in newly diagnosed chronic myeloid leukemia. N Engl J Med 2003;349:1423–32. 33. Zhang T, Grenier S, Nwachukwu B, Wei C, Lipton JH, Kamel-Reid S, et al. Inter-laboratory comparison of chronic myeloid leukemia minimal residual disease monitoring: summary and recommendations. J Mol Diagn 2007;9:421–30. 34. Davidian M, Giltinan DM. Nonlinear models for repeated measurement data: an overview and update. JABES 2003;8:387–419. 35. Sheiner BL, Beal SL. Evaluation of methods for estimating population pharmacokinetic parameters. II. biexponential model and experimental pharmacokinetic data. J Pharmacokinet Biopharm 1981;9:635–51. 36. Beal SL. Ways to fit a PK model with some data below the quantification limit. J Pharmacokinet Pharmacodyn 2001;28:481–504. 37. O'Brien SG, Guilhot F, Larson RA, Gathmann I, Baccarani M, Cervantes F, et al. Imatinib compared with interferon and low-dose cytarabine for newly diagnosed chronic-phase chronic myeloid leukemia. N Engl J Med 2003;348:994–1004. 38. Finch CA, Harker LA, Cook JD. Kinetics of the formed elements of human blood. Blood 1977;50:699–707. 39. Friberg LE, Karlsson MO. Mechanistic models for myelosuppression. Invest New Drugs 2003;21:183–94. 40. Abe A, Minami Y, Hayakawa F, Kitamura K, Nomura Y, Murata M, et al. Retention but significant reduction of BCR–ABL transcript in hematopoietic stem cells in chronic myelogenous leukemia after imatinib therapy. Int J Hematol 2008;88:471–5. Clin Cancer Res; 17(21) November 1, 2011 Downloaded from clincancerres.aacrjournals.org on June 17, 2017. © 2011 American Association for Cancer Research. OF9 Published OnlineFirst September 8, 2011; DOI: 10.1158/1078-0432.CCR-11-0396 Stein et al. 41. Bhatia R, Holtz M, Niu N, Gray R, Snyder DS, Sawyers CL, et al. Persistence of malignant hematopoietic progenitors in chronic myelogenous leukemia patients in complete cytogenetic remission following imatinib mesylate treatment. Blood 2003;101:4701–7. 42. Chen CI, Maecker HT, Lee PP. Development and dynamics of robust Tcell responses to CML under imatinib treatment. Blood 2008;111: 5342–9. 43. Kim PS, Lee PP, Levy D. Dynamics and potential impact of the immune response to chronic myelogenous leukemia. PLoS Comput Biol 2008;4:e1000095. OF10 Clin Cancer Res; 17(21) November 1, 2011 44. Roeder I, Glauche I. Pathogenesis, treatment effects, and resistance dynamics in chronic myeloid leukemia—insights from mathematical model analyses. J Mol Med 2008;86:17–27. 45. Saglio G, Kim DW, Issaragrisil S, le Coutre P, Etienne G, Lobo C, et al. Nilotinib versus imatinib for newly diagnosed chronic myeloid leukemia. N Engl J Med 2010;362:2251–9. 46. Michor F. Quantitative approaches to analyzing imatinib-treated chronic myeloid leukemia. Trends Pharmacol Sci 2007;28:197–9. 47. Michor F. Reply: the long-term response to imatinib treatment of CML. Br J Cancer 2007;96:679–80. Clinical Cancer Research Downloaded from clincancerres.aacrjournals.org on June 17, 2017. © 2011 American Association for Cancer Research. Published OnlineFirst September 8, 2011; DOI: 10.1158/1078-0432.CCR-11-0396 BCR−ABL Transcript Dynamics Support the Hypothesis That Leukemic Stem Cells Are Reduced during Imatinib Treatment Andrew M. Stein, Dean Bottino, Vijay Modur, et al. Clin Cancer Res Published OnlineFirst September 8, 2011. Updated version Supplementary Material E-mail alerts Reprints and Subscriptions Permissions Access the most recent version of this article at: doi:10.1158/1078-0432.CCR-11-0396 Access the most recent supplemental material at: http://clincancerres.aacrjournals.org/content/suppl/2011/09/08/1078-0432.CCR-11-0396.DC1 http://clincancerres.aacrjournals.org/content/suppl/2011/10/26/1078-0432.CCR-11-0396.DC2 Sign up to receive free email-alerts related to this article or journal. To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at [email protected]. To request permission to re-use all or part of this article, contact the AACR Publications Department at [email protected]. Downloaded from clincancerres.aacrjournals.org on June 17, 2017. © 2011 American Association for Cancer Research.