Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Sound localization wikipedia , lookup
Speech perception wikipedia , lookup
Noise-induced hearing loss wikipedia , lookup
Specific language impairment wikipedia , lookup
Audiology and hearing health professionals in developed and developing countries wikipedia , lookup
Olivocochlear system wikipedia , lookup
Sensorineural hearing loss wikipedia , lookup
Lip reading wikipedia , lookup
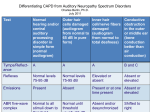
Characteristics of Auditory Neuropathy and Central Auditory Processing Disorder Prepared by Charles Berlin, Ph.D. July 2011 Test Auditory Neuropathy (ANSD) Central Auditory Behavioral Result Processing Disorder Birth History About 30% are very premature. About 35% have histories of jaundice and transfusion. 40% of NICU babies have this but they make up about 15% of the total of ANSD patients. About 10% do NOT need intervention because they have very mild cases Twelve genes now known, the most prevalent of which are Otoferlin, Pejvakin, and Connexins (26 and 30) and MohrTranebjaerg, an x-linked late-onset disorder that includes blindness Anywhere from mildly impaired to totally deaf. Generally unremarkable, but sometimes prematurity ANSD children need to have age-corrected studies of speech and language. CAPD kids are hard if not impossible to diagnose correctly until they can use language and take complex listening tasks. Children with no usable hearing CANNOT BE DIAGNOSED WITH BEHAVIORAL TESTS SUCH AS S.C.A.N. ETC. Electrophysiology is necessary along with MRIs and CAT scans. No known genetic causes. Genetic ANSD patients will not “get better” the way NICU babies or other birth damaged infants might. Again in cases like USHER 1, 2, etc., pure tone audiometry which confirms deafness makes it nearly impossible to make a behavioral diagnosis properly. Almost always normal CAPD children rarely if ever behave as if they are totally deaf unless they have demonstrable Genetics Audiogram Tympanometry Generally Normal Generally normal Middle Ear Muscle Reflexes Almost always absent or elevated Auditory brainstem responses Speech in Noise Never normal Virtually always normal. IF A CHILD IS DIAGNOSED AS HAVING CAPD IN ISOLATION, HE/SHE must have NORMAL REFLEXES. Virtually always normal Very poor Very poor Management Cochlear implants, FM systems, hearing aids (least effective in our sample, Berlin et al. 2010) Fast ForWord, Earobics, and other training programs that modify the speech signal. Difficult to employ if the peripheral audiogram is very poor. temporal lobe lesions. Children with middle ear disease will have abnormal tympanograms that require medical or surgical attention. The reflexes assess the lower brainstem’s integrity along with inner hair cells. CAPD patients should not have elevated middle ear muscle reflex thresholds and should always be between 75 and 95 dB. The site of lesion in ANSD starts at the inner hair cells (Amatuzzi et al. ) can extend to the primary nerve fibers (Starr et al.) This is often why people are (mis-)diagnosed as having CAPD. At worst, CAPD is a diagnosis by exclusion, or hunch; at best, one must always rule out ANSD because the behavioral symptoms are so similar when it comes to haring in noise and educational impact. The literature is quite muddy with respect to CAPD and deaf-blindness.