Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
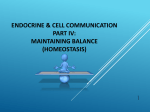
Toxic Bradycardia and Hypotension Alyssa Reed, R1 Thanks to Dr Mark Yarema CASE It is 330 am when the paramedics patch to tell you they are on scene with a man who has a pulse of 45 and SBP of 80 What medical conditions could cause this? Medical Causes of Bradycardia MI Sick Sinus Syndrome Hyperkalemia Hypothermia Increased ICP Vasovagal Physiologic (athletes) CASE CONTINUED… The patient arrives. Vitals are unchanged after 2L N/S and 2 mg of atropine. He is obtunded but breathing spontaneously. His wife says he has a history or atrial fibrillation, angina, hypertension and depression. The paramedics found a lot of pill bottles beside him and suspect an overdose. They left the bottles behind. What medications cause bradycardia? TOXIC BRADYCARDIA Beta Blockers Calcium Channel Blockers Cardiac glycosides (digoxin) Cholinergic agents Clonidine/Imidazolines (alpha2 agonists) Opioids/Sedative Hypnotics Phenylpropanolamine (alpha1 agonists) Sodium channel blockers Can we eliminate any of these based on clinical presentation? TOXIC BRADYCARDIA Beta Blockers Calcium Channel Blockers Cardiac glycosides (digoxin) Cholinergic agents Clonidine/Imidazolines (alpha2 agonists) Opioids/Sedative Hypnotics Phenylpropanolamine (alpha1 agonists) Sodium channel blockers THE “BIG FOUR” Beta Blockers Calcium Channel Blockers Cardiac Glycosides Sodium Channel Blockers Introduction Maybe put in some physiology and table 17.11 page 393 of lilly CASE 40M brought by EMS after an OD. Drug unknown. Pulse is 50 and SBP is 90. Which of the four do you think is most likely responsible? Na Channel Blockers Class IA Antiarrhythmics TCAs • Quinidine Diltiazem/Verapamil • Procainamide Propranolol • Disopyramide Carbamazepine Class IC Antiarrhythmics • Flecainide • Propafenone Cocaine Presentation QRS widening Hypotension Seizures Altered Mental Status Membrane Stabilizing Activity Decreased perfusion Management Sodium Bicarbonate 50ml = 50mEq = 1ampule Indications QRS > 100ms 2 Persistent hypotension despite adequate fluid resus 3 Dysrhythmias Dosing • Bolus 3 amps • 3 amps in a bag of D5W and infuse and 2-3x maintenance 1 Hypertonic Saline CASE A 55M is brought in by the paramedics with a pulse of 40 and SBP of 78. His BG is 18. He is AOx3. He has a history of “heart problems” and no other medical history K 4.0 Which of the “big four” is likely responsible? (see next ECG to help eliminate) Put in ECG that is slow and narrow Beta Blockers Calcium Channel Blockers Vitals Hypotensive Bradycardic Hypotensive Bradycardic Tachycardic Mental Status Depressed Preserved Blood Glucose Low-Normal High Calcium Channel Blockers All block L-type calcium channels Heart* Contractile Tissue • Pacemaker cells Vascular Smooth Muscle* Endocrine (including beta pancreatic cells) Retina Skeletal muscle • 1) Myocyte depolzn triggers opening of LTCC Put in a pic of the channels and depolarization 2) Causes release of stored Ca from SR 3) Contract Calcium Channel Blockers 2 Major Clasess Dihydropyridines • Preferentially block L-type calcium channels in the vasculature • Potent vasodilators with little negative effect upon cardiac contractillity or conduction Non-dihydropyridines • Preferentially block L-type calcium channels in the myocardium • Negative inotropic effects and decrease AV node conduction Q: Why is brady not listed as complication of the dihydropyridines? CCB OD Presentation Hypotension Bradydysrhythmias (or reflex tachycardia) Normal mental status Hyperglycemia disruption of fatty acid metabolism creating relative insulin resistance and decreased release of insulin from β panc cells Pulmonary Edema Heart failure + vasodilation and extravasation Ileus Decreased smooth muscle function in bowel CCB OD Dx No urine or serum test readily available ECG CXR Lytes (including Ca, Mg) Blood Glucose ABG What are some of the ECG findings/rhythms in CCB OD? CCB OD and the ECG Bradysrhythmias • AV block of all degrees • Sinus arrest • AV dissociation • Junctional rhythm • Asystole Reflex Sinus Tach • Nifedipine OD OD General Approach 1. ABCs 2. GI Decontamination • • • Activated charcoal (50G in adult, 1g/kg in peds) Gastric Lavage Whole Bowel Irrigation (polyethylene glycol 2L/hr adults, 500cc/hr peds) 3. Enhanced Elimination • Hemodialysis 4. Antidotes 5. Supportive care CCB OD Mx HYPOTENSION BRADYCARDIA • Fluids • Atropine • Calcium • Calcium • Glucagon • Glucagon • Pressors • Pacer Atropine Given routinely to symptomatic bradycardic patients Often ineffective Adults: 0.5-1 mg IV Q3min to a max of 3mg Peds: 0.02mg/kg IV with a min dose of 0.1mg and a max of 1mg Calcium CALCIUM CHLORIDE CALCIUM GLUCONATE • 10% solution • 10% solution • 1g/10ml • 1g/10ml • 1g = 13.6 mEq • 1g = 4.5 mEq • Central line • Peripheral line • Dose: 1g over 10 min • Dose: 3g (30cc) over (10cc) Q15 to a max of 6 g and can infuse 1-2g/hr if responsive 10 min Glucagon Increases intracellular levels of cAMP • Opens Ca channels Animal models • increase in heart rate • Little effect on MAP Bolus: 5mg over 1-2 min, to max of 15mg (this is diluted in 10cc N/S) Maintenance: infusion of response dose mg/hr Vomiting and aspiration risk Phenol toxicity Glucagon Catecholamine pressors Glucagon Gs Amrinone ATP cAMP Phosphodiesterase AMP Pressors Q: What would be the ideal properties of a pressor in CCB tox? A: Direct-acting agent with +chronotropy, inotropy, and vasoconstrictive effects Q: What would you use? A: Norepinenphrine is initial choice Dopamine not because indirect effects and little alpha Can increase pulmonary edema and ischemic vascular dz and renal failure Insulin and Glucose CJEM 2006 Prediger and Yarema Systematic review of 13 papers 20 cases of CCB OD (17 adult, 3 pediatric) Most effective at treating hypotension (n=15) 3 patients converted to sinus from AV block Dosing and length of treatment varied widely AE: asymptomatic hypoglycemia (n=8),hypokalemia (n=4) Conclusion: HDIG is safe and effective treatment of CCB overdose Insulin and Glucose The heart usually metabolizes free fatty acids but in shock state it needs glucose In CCB OD cardiac glucose uptake is impaired b/c Decreased insulin release (calcium mediated) 2. CCB toxicity induces a state of insulin resistance (myocardium and rest of body) 3. Acidosis and low perfusion limits glycolysis and carbohydrte delivery to the heart 1. Insulin acts as a pressor Improved glucose delivery and uptake to the heart and improving cardiac performance Insulin and Glucose Disrupt state of carbohydrate dependence and insulin resistance Animal models • Improved survival with hyperinsulinemia/euglycemia compared to calcium, pressors and glucagon • Positive inotropic effects Bolus: 0.1U/kg IV of regular insulin Infusion: 0.2-0.5 U/kg/hr Glucose: 25-50 g of dextrose at beginning or can infuse at 0.5 g/kg/hr Other Therapies Phosphodiesterase Inhibitors • Amrinone , milrinone • Increase cAMP by preventing degradation of it by phosphodiesterase enzyme • May exacerbate hypotension • ICU setting with pulmonary artery catheter Sodium Bicarbonate • Prolonged QRS or lactic acidosis • 1amp= 50mEq • Put 3 amps in 1L D5W and infuse and two times maintenance Invasive Mx Transvenous pacing • Does not counteract negative inotropic effects • Successful capture may not correct hypotension Intraaortic balloon pump Cardiopulmonary bypass Summary Block L-type channels • Vascular smooth muscle • Cardiac muscle cells and pacemaker cells Hypotension, brady or tachy, preserved mental status, hyperglycemic Mx • Early WBI • Fluids/atropine • Calcium • Glucagon • Pressors • Insulin and glucose CASE 50F brought in by EMS. Patient is altered. T= 37, P= 50, RR= 12, SBP= 74, O2=90%RA, BG 3.5 Hx of “heart problems” and hypertension Which of the big four do you suspect? Beta Receptors Beta 1 Primarily in the heart Increase 1) heart rate, 2) contractility, and 3) AV conduction Decrease AV node refractoriness Beta 2 Primarily in bronchial and peripheral smooth muscle Also in liver, uterus, heart Vasodilation, bronchodilation, gluconeogenesis, glycogenolysis Beta 3 Adipose tissue and heart Thermogenesis Beta Blockers Structurally resemble isoproterenol (pure β agonist) Competitively inhibit endogenous catecholamines (ex. Epinephrine) at the B-receptor These catecholamines normally bind to the receptor and result in activation of adenyl cyclase, resulting in cAMP cAMP augments: Inotropy (myocardial contraction) 2. Dromotropy (cardiac conduction) 3. Chronotropy (heart rate) 1. How would you expect the patient to present? Clinical Presentation Bradycardia Seizures (esp. Hypotension propranolol) Symptomatic Bronchospasm VT or VF Mild hyperK Unconsciousness Respiratory arrest or insufficiency Hypoglycemia (uncommon in adults) Rosen’s Table 150-8 βB Properties 1. Membrane-Stabilizing Activity (MSA) • • Inhibition of myocardial fast sodium channels Can result in wide QRS and other dysrhythmias 2. Lipophilicity • • High lipid solubility= rapidly cross BBB Cause altered LOC (independent of hypoperfusion) 3. Intrinsic Sympathomimetic Activity (ISA) Partial agonist effect at beta receptor site Cause less bradycardia and hypotension DO NOT completely protect Noncardioselective βB MSA Lipophilic ISA ½ life (hr) Comments Propranolol ++ + - 4 Most deaths Nadolol - - - 10-20 Dialyzable Labetalol + - - 4-6 α blocker too Sotalol - + - 7-18 Class III/II Rosen’s Table 150-3 Cardioselective βB MSE Lipohilic ISA ½ life (hr) Metoprolol - + - 3-4 Atenolol - - - 5-8 Esmolol - - - 0.13 Acebutolol ++ + + 2-4 Rosen’s Table 150-3 Comments Dialyzable QT long βB OD and the ECG Increased PR from decreased conduction velocity down AV node Bradycardia from decreased automaticity within SA node Ventricular tachydysrhythmias with MSA βB Wide QRS with MSA βB QT prolongation with sotalol OD Which beta blocker might cause this dysrhythmia? βB OD Mx HYPOTENSION BRADYCARDIA* • Fluids • Atropine • Glucagon • Glucagon • Epinephrine • Pacemaker • Isoproterenol • Epinephrine • Isoproterenol * Only tx if third degree block or symptomatic Atropine Symptomatic bradycardia only Adults: O.5-1mg IV to a max of 3mg Peds: 0.02mg/kg with a min of 0.1mg and max of 1mg Poor effect on improving bradycardia and hypotension Glucagon Remember glucagon activates adenylate cyclase at a site independent from beta-adrenergic sites • Increases cAMP= increases intracellular Ca= increasing contractility Considered first line (“antidotal”) Dose • 2-5mg (50mcg/kg in peds) diluted in 10cc N/S over 1- 2 min to a max of 15mg • Maintenance: response dose in mg/hr Beta blocker “antidotes” Catecholamine pressors Glucagon Gs Amrinone ATP cAMP Phosphodiesterase AMP Insulin Animal models show promise • Improved cardio and hemodynamic parameters and decreased mortality No definite dosing regimen • Regular insulin infusion starting at 0.1U/kg/hr combined with glucose at 1g/kg/hr • Check glucose levels every 30-60min • Less than in CCB OD (0.2-0.5U/kg/hr after a bolus) Others Calcium • Shown to reverse hypotension in animal and human models • Dosing: see CCB OD section (Calcium chloride vs. gluconate) Pressors • Epinephrine and norepinephrine have both been used • Poor outcomes Isoproterenol • Should be ideal because B1 and B2 agonist effects • However, can worsen hypotension Others Phosphodiesterase Inhibitors • Inhibit breakdown of cAMP by phosphodiesterases • Case reports only • Use only after other therapies have failed Sodium Bicarbonate • Safe adjunct • Use if QRS wide • 1-2mEq/kg IV push Magnesium • Ventricular arrhythmias • Sotalol OD Others Intravenous pacing • Profound bradycardia • Frequently cannot capture • Can increase heart rate without a corresponding increase in perfusion Intraaortic balloon pump • Successful case reports in failed pharmacological tx of propranolol and atenolol OD Hemodialysis • Nadolol, sotalol, atenolol Summary BETA BLOCKER OD 1. GI Decontamination 2. Atropine/Fluids 3. Glucagon 4. Calcium 5. Insulin/Glucose 6. Pressors (with caution) 7. Phosphodiesterase inhibitors 8. Invasive tx CCB OD 1. GI decontamination 2. Atropine/Fluids 3. Calcium 4. Glucagon 5. Insulin/glucose 6. Pressors (with caution) 7. Invasive tx CASE 55M brought in by EMS. Pulse is 45, SBP is 95. Patient complaint of nausea and vomiting for several days and difficulty seeing for the last day. Hx: HTN, Afib Vomiting and PVCs What did he likely take? Cardiac Glycosides Na-K ATPase Inhhibitors Digoxin, Digitoxin, Ouabain, Foxglove, Lilly of the valley, oleander 2 desired effects of Digoxin 1. Improve the contractility of the failing heart • By blocking the Na-K ATPase pump and ultimately increasing intracellular Ca which increases the force of contraction 2. Prolong the refractory period of the AV node in pts with SVT • By enhancing vagal tone and reducing sympathetic activity Clinical Presentation ACUTE Few initial signs and symptoms Cardiac instability HyperK * Usually preserve BP and not significantly hypotensive like βB and CCBs CHRONIC Fatigue Vision • Blurred vision • Color disturbances GI • Abdo pain • Diarrhea • Nausea/Vomiting CNS • Headache • Dizziness • Confusion Diagnosis ECG Electrolytes Serum digoxin level Measure at least 6 hrs after last dose (time needed to reach steady state) False + elevated levels (no SSx) • Pregnant women • Chronic renal failure or hepatobiliary dz False – normal levels (sig SSx) • Foxglove or oleander ingestion Digoxin and the ECG Increased vagal tone. What are common digoxin toxic arrhythmias? Increased automaticity Dig Tox and the ECG NONSPECIFIC PVCs 1st, 2nd (type 1), 3rd degree AV block Sinus bradycardia Sinus tachycardia Sinoatrial block or arrest Afib with slow ventricular response Junctional escape rhythm AV dissociation Ventricular bigeminy and trigeminy VTach/VFib Torsades de pointes Dig Tox and the ECG MORE SPECIFIC Afib with slow, regular ventricular rate (AV dissociation) Nonparoxysmal junctional tachycardia (70-130 bpm) Atrial tachycardia with block (150-200 bpm) Bidirectional VTach Dig Tox and the ECG Very rarely see Mobitz Type II block Afib or Aflutter with rapid ventricular response Unimorphic Vtach AFIB with Slow Ventricular Response Nonparoxysmal Junctional Tachycardia Bidirectional VT Potassium and Dig Toxicity Acute Toxicity • Correlates with hyperkalemia • K level determines prognosis and treatment Chronic Toxicity • K normal or low • Slow rise over time allows kidneys to balance • Patients often also on diuretic which reduce the K level Potassium and acute digoxin toxicity 8 K<5.0, 0% mortality K 5-5.5, 50% mortality K>5.5 100% mortality 7 6 5 4 3 Died Survived Bismuth, C., et al. Hyperkalemia in acute digitalis poisoning: prognostic significance and therapeutic implications. Clin Toxicol 1973; 6:153. Predisposing Factors Advanced age Women Renal Insufficiency Heart Disease • Congenital Heart Dz Electrolyte Imbalance • Hypo or hyper kalemia • Hypomagnesemia • Hypercalcemia Sympathomimetic Drugs Cardiotoxic Coingestants • Ischemic heart Dz • BB • CHF • CCB • Myocarditis • Tricyclic antidepressants Alkalosis Hypothyroidism Drug Interactions • Quinidine, amiodarone • Erythromycin Management of Dig Toxicity GI Decontamination Electrolyte Correction Bradycardias Ventricular Dysrhythmias Fab Fragments GI Decontamination Digoxin is absorbed effectively by activated charcoal Within one hour of ingestion 50g for adults 1g/kg for peds No improvement in outcome has been proven Electrolyte Correction K Hypo: in chronic tox want to replace (goals of 3.5 to 4mEq/L) • Oral repletion preferred • Don’t replace in acute Hyper: in acute tox want to reduce it • Insulin glucose • Beta agonist • Sodium bicarbonate • NOT Calcium Mg • Hypomag often reported • Replace with 2-4g magnesium sulfate Bradycardias Atropine • Reverses dig induced vagal tone • More effective than in other cardiac drug toxicity (acute toxicity) • 0.5mg-1mg to a max of 3mg Q2-3 min Pacing • If fail atropine treatment • Catheter may induce ventricular dysrhythmias • External pacing safer but not as effective Ventricular Dysrhythmias Vagal Maneuvers • NO!!! Can cause asystole and cardiac arrest Phenytoin • Safe • May enhance AV conduction • Load with 10-15mg/kg Infuse at 25-50mg/min Lidocaine • Safe • Load with 1-3mg/kg Infuse at 1-4mg/min Fab Fragments Digibind™ Purified from sheep Rapidly bind to digoxin in the tissues Efflux of intracellular digoxin Further binding of free digoxin Renally excreted Indications for Digibind™ 1. Vetricular dysrhythmias 2. Severe bradycardia unresponsive to atropine 3. Serum K > 5 mEq/L (acute ingestion) 4. Serum digoxin level >10 mmol/L at any time >12.5 mmol/L 6 hours after ingestion 5. Acute Ingestion of > 10mg (4mg peds) 6. Presence of a digoxin-toxic rhythm in the setting of an elevated digoxin level Effectiveness of Digibind Antman, EM, et al. Circulation 1990 N=150 (cases of life-threatening digitalis tox) Results • 80% complete resolution of all signs and symptoms • 10% improved • 10% showed no response • Median time to initial response was 19 min • Time to complete response was 88 min • 54% of cardiac arrest patients survived hospitalization Nonresponders to Digibind 1. Underlying heart disease (that causes some of the manifestations) 2. Too low a dose of Fab 3. Moribund on presentation 4. Co-ingestion of other cardiac toxic drugs Dosing of Digibind Given IV over 30 minutes Unless arrested, then give as a bolus Vials of Fab= (Dig level ng/ml x Mass kg)/ 100 Always round up Example: how many vials would you need for a 70kg woman with a digoxin level of 3 and frequent PVCs? Vials= (3 x 70) / 100 = 2.1 so you would give 3 What if you don’t know the dig level right away??? Dosing of Digibind ACUTE Stable- 5 vials Unstable- 15 vials CHRONIC Stable- 1 vial Unstable- 4 vials *1 vial costs approx 400$ Summary- Acute vs Chronic CHRONIC ACUTE 1. Higher mortality 1. Lower mortality 2. K normal or low 2. K normal or high 3. Ventricular dysrhythmias 3. Bradycardia and AV more common 4. Usually elderly patients 5. Often need Fab fragment therapy 6. Underlying heart dz increases morbidity and mortality block more common 4. Usually younger patients 5. Often do well without Fab fragment therapy 6. Absence of heart dz decreases morbidity and mortality Bradycardia and Hypotension Sodium channel blockers Wide QRS. Rx = bicarbonate Digoxin Blocks, increased automaticity. Rx = digibind. Calcium channel blockers Increased glucose, preserved mental status Rx - Calcium, pressors, insulin / glucose Beta blockers Altered mental status, normal glucose Rx - Glucagon, insulin / glucose, pressors