Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
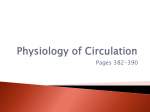
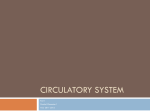
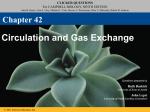
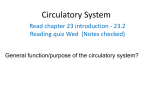
Blood Vessels Part 2 Slides by Barbara Heard and W. Rose. figures from Marieb & Hoehn 9th eds. Portions copyright Pearson Education Monitoring Cardiovascular Performance Vital signs: HR, blood pressure, respiratory rate, body temperature Radial artery routinely used for HR Other locations also work: where arteries are close to body surface – Carotid, femoral, dorsalis pedis, posterior tibial K.A.A.P. Figure 19.12 Body sites where the pulse is most easily palpated. Superficial temporal artery Facial artery Common carotid artery Brachial artery Radial artery Femoral artery Popliteal artery Posterior tibial artery © 2013 Pearson Education, Inc. Dorsalis pedis artery Measuring Blood Pressure • Systemic arterial BP – Measured indirectly by auscultatory method using a sphygmomanometer – Pressure increased in cuff until it exceeds systolic pressure in brachial artery – Pressure released slowly and examiner listens for sounds of Korotkoff with a stethoscope © 2013 Pearson Education, Inc. Measuring Blood Pressure • Systolic pressure, normally less than 120 mm Hg, is pressure when sounds first occur as blood starts to spurt through artery • Diastolic pressure, normally less than 80 mm Hg, is pressure when sounds disappear because artery no longer constricted; blood flowing freely © 2013 Pearson Education, Inc. Alterations in Blood Pressure • Hypertension: high blood pressure Systolic pressure >=140 mmHg or Diastolic pressure >=90 (or both) • Chronic (sustained) hypertension Increased risk of MI (heart attack), heart failure, stroke, peripheral vascular disease… © 2013 Pearson Education, Inc. Primary or Essential Hypertension • Most (90% of) hypertension is “Essential hypertension” • No obvious other cause (such as endocrine disorder, etc.) • Risk factors: family history, diet, obesity, age, diabetes mellitus, stress, smoking • No cure but can be controlled – Restrict salt, fat intake – Increase exercise, lose weight, stop smoking – Antihypertensive drugs © 2013 Pearson Education, Inc. Homeostatic Imbalance: Hypertension • Secondary hypertension less common – Due to identifiable disorders including obstructed renal arteries, kidney disease, and endocrine disorders such as hyperthyroidism and Cushing's syndrome – Treatment focuses on correcting underlying cause © 2013 Pearson Education, Inc. Alterations in Blood Pressure • Hypotension: low blood pressure – Blood pressure below 90/60 mm Hg – Usually not a concern • Only if leads to inadequate blood flow to tissues – Often associated with long life and lack of cardiovascular illness © 2013 Pearson Education, Inc. Homeostatic Imbalance: Hypotension • Orthostatic hypotension: temporary low BP and dizziness when suddenly rising from sitting or reclining position • Chronic hypotension: hint of poor nutrition and warning sign for Addison's disease or hypothyroidism • Acute hypotension: important sign of circulatory shock; threat for surgical patients and those in ICU © 2013 Pearson Education, Inc. Blood Flow Through Body Tissues • Tissue perfusion involved in – Delivery of O2 and nutrients to, and removal of wastes from, tissue cells – Gas exchange (lungs) – Absorption of nutrients (digestive tract) – Urine formation (kidneys) • Rate of flow is precisely right amount to provide proper function © 2013 Pearson Education, Inc. Figure 19.13 Distribution of blood flow at rest and during strenuous exercise. 750 750 Brain 750 Heart 250 12,500 1200 Skeletal muscles 500 Skin Kidneys 1100 Abdomen 1400 1900 Other 600 Total blood flow at rest 5800 ml/min 600 600 400 © 2013 Pearson Education, Inc. Total blood flow during strenuous exercise 17,500 ml/min Velocity of Blood Flow • Changes as travels through systemic circulation • Inversely related to total cross-sectional area • Fastest in aorta; slowest in capillaries; increases in veins • Slow capillary flow allows adequate time for exchange between blood and tissues © 2013 Pearson Education, Inc. Figure 19.14 Blood flow velocity and total cross-sectional area of vessels. Relative crosssectional area of different vessels of the vascular bed 5000 4000 Total area (cm2) of the 3000 vascular 2000 bed 1000 0 Velocity of blood flow (cm/s) © 2013 Pearson Education, Inc. 50 40 30 20 10 0 Autoregulation Automatic adjustment of blood flow to tissues to meet metabolic requirements Controlled intrinsically (i.e. locally) by modifying arteriolar diameter - does not require autonomic nervous system activity Organs regulate their own blood flows by varying resistance of their own arterioles Autoregulation Two types of autoregulation • Metabolic control • Myogenic control Combination of both determines overall response Autoregulation Keeping flow constant when pressure gradient changes. In a rigid pipe: Resistance (R) does not change. The equation Flow = ΔP / R predicts that when pressure changes, flow will change by the same percent as pressure. In an elastic tube: A pressure change causes a diameter change, and hence a resistance change: pressure ↑ ⇒ diameter ↑ ⇒ resistance ↓ As a result, a pressure change will cause a larger flow change than what you’d get in a rigid pipe. In a vascular bed with autoregulation: Flow changes little when the pressure gradient changes. Percent change in flow is smaller than percent change in pressure. Autoregulation Keeping flow constant when pressure gradient changes. Graph shows pressure-flow relation (vertical axis=change in flow, horiz. axis=change in pressure) for rigid pipes (), elastic tubes (), “perfect” autoregulation (), and actual measurements in dogs whose neural reflexes are temporarily blocked (). We expect “passive “ blood vessels to look like . The fact that they look like shows they are not passive – they autoregulate. Coleman, Granger, Guyton 1971 Measurements in animals with neural reflexes blocked Metabolic Autoregulation Vasodilation of arterioles and relaxation of precapillary sphincters occurs in response to – Declining tissue O2 – Substances from metabolically active tissues (H+, K+, adenosine, and prostaglandins) and inflammatory chemicals © 2013 Pearson Education, Inc. Metabolic Autoregulation Effects – Relaxation of vascular smooth muscle if flow is insufficient for demand – Release of NO (powerful vasodilator) by endothelial cells Endothelins released from endothelium are potent vasoconstrictors NO and endothelins balanced unless blood flow inadequate, then NO wins Inflammatory chemicals also cause vasodilation © 2013 Pearson Education, Inc. Myogenic Autoregulation How it seems to work: Pressure ↑ ⇒ tension in vessel wall ↑ ⇒ vascular smooth muscle constricts ⇒ diameter ↓ ⇒ resistance ↑ Therefore, a pressure change causes a resistance change that prevents flow from changing as much as it would have, if resistance had just stayed the same (or worse, if resistance had changed in the way you’d expect for an elastic tube) P.C. Johnson, Circ Res. 1986. Figure 19.15 Intrinsic and extrinsic control of arteriolar smooth muscle in the systemic circulation. Vasodilators Metabolic O2 CO2 H+ K+ • Prostaglandins • Adenosine • Nitric oxide Neuronal Sympathetic tone Hormonal • Atrial natriuretic peptide Extrinsic mechanisms Intrinsic mechanisms (autoregulation) Vasoconstrictors • Metabolic or myogenic controls • Distribute blood flow to individual organs and tissues as needed Myogenic • Stretch © 2013 Pearson Education, Inc. Neuronal Sympathetic tone Metabolic Hormonal • Endothelins • Angiotensin II • Antidiuretic hormone • Epinephrine • Norepinephrine • Neuronal or hormonal controls • Maintain mean arterial pressure (MAP) • Redistribute blood during exercise and thermoregulation Long-term Autoregulation • Occurs when short-term autoregulation cannot meet tissue nutrient requirements • Angiogenesis – Number of vessels to region increases and existing vessels enlarge – Common in heart when coronary vessel occluded, or throughout body in people in high-altitude areas © 2013 Pearson Education, Inc. Blood Flow: Skeletal Muscles • Varies with fiber type and activity – At rest, myogenic and general neural mechanisms predominate - maintain ~ 1L /minute – During muscle activity • Active or exercise hyperemia - blood flow increases in direct proportion to metabolic activity • Local controls override sympathetic vasoconstriction • Muscle blood flow can increase 10 © 2013 Pearson Education, Inc. Blood Flow: Brain • Blood flow to brain constant as neurons intolerant of ischemia; averages 750 ml/min • Metabolic controls – Decreased pH of increased carbon dioxide cause marked vasodilation • Myogenic controls – Decreased MAP causes cerebral vessels to dilate – Increased MAP causes cerebral vessels to constrict © 2013 Pearson Education, Inc. Blood Flow: Brain • Brain vulnerable under extreme systemic pressure changes – MAP below 60 mm Hg can cause syncope (fainting) – MAP above 160 can result in cerebral edema © 2013 Pearson Education, Inc. Blood Flow: Skin • Blood flow through skin – Supplies nutrients to cells (autoregulation in response to O2 need) – Helps regulate body temperature (neurally controlled) – primary function – Provides a blood reservoir (neurally controlled) © 2013 Pearson Education, Inc. Blood Flow: Skin • Blood flow to venous plexuses below skin surface regulates body temperature – Varies from 50 ml/min to 2500 ml/min, depending on body temperature – Controlled by sympathetic nervous system reflexes initiated by temperature receptors and central nervous system © 2013 Pearson Education, Inc. Temperature Regulation • As temperature rises (e.g., heat exposure, fever, vigorous exercise) – Hypothalamic signals reduce vasomotor stimulation of skin vessels – Warm blood flushes into capillary beds – Heat radiates from skin © 2013 Pearson Education, Inc. Temperature Regulation • Sweat also causes vasodilation via bradykinin in perspiration – Bradykinin stimulates NO release • As temperature decreases, blood is shunted to deeper, more vital organs © 2013 Pearson Education, Inc. Blood Flow: Lungs • Pulmonary circuit unusual – Pathway short – Arteries/arterioles more like veins/venules (thin walled, with large lumens) – Arterial resistance and pressure are low (24/10 mm Hg) © 2013 Pearson Education, Inc. Blood Flow: Lungs • Autoregulatory mechanism opposite that in most tissues – Low O2 levels cause vasoconstriction; high levels promote vasodilation • Allows blood flow to O2-rich areas of lung © 2013 Pearson Education, Inc. Blood Flow: Heart • During ventricular systole – Coronary vessels are compressed • Myocardial blood flow ceases • Stored myoglobin supplies sufficient oxygen • During diastole high aortic pressure forces blood through coronary circulation • At rest ~ 250 ml/min; control probably myogenic © 2013 Pearson Education, Inc. Blood Flow: Heart • During strenuous exercise – Coronary vessels dilate in response to local accumulation of vasodilators – Blood flow may increase three to four times • Important–cardiac cells use 65% of O2 delivered so increased blood flow provides more O2 © 2013 Pearson Education, Inc. Blood Flow Through Capillaries • Vasomotion – Slow, intermittent flow – Reflects on/off opening and closing of precapillary sphincters © 2013 Pearson Education, Inc. Capillary Exchange of Respiratory Gases and Nutrients • Diffusion down concentration gradients – O2 and nutrients from blood to tissues – CO2 and metabolic wastes from tissues to blood • Lipid-soluble molecules diffuse directly through endothelial membranes • Water-soluble solutes pass through clefts and fenestrations • Larger molecules, such as proteins, are actively transported in pinocytotic vesicles or caveolae © 2013 Pearson Education, Inc. Figure 19.16 Capillary transport mechanisms. (1 of 2) Pinocytotic vesicles Red blood cell in lumen Endothelial cell Fenestration (pore) Endothelial cell nucleus Basement membrane © 2013 Pearson Education, Inc. Tight junction Intercellular cleft Figure 19.16 Capillary transport mechanisms. (2 of 2) Lumen Caveolae Pinocytotic vesicles Intercellular cleft Endothelial fenestration (pore) Basement membrane 1 Diffusion through membrane (lipid-soluble substances) © 2013 Pearson Education, Inc. 2 Movement through intercellular clefts (watersoluble substances) 4 Transport via vesicles or caveolae (large substances) 3 Movement through fenestrations (water-soluble substances) Fluid Movements: Bulk Flow • Fluid leaves capillaries at arterial end; most returns to blood at venous end – Extremely important in determining relative fluid volumes in blood and interstitial space • Direction and amount of fluid flow depend on two opposing forces: hydrostatic and colloid osmotic pressures © 2013 Pearson Education, Inc. Hydrostatic Pressures • Capillary hydrostatic pressure (HPc) (capillary blood pressure) – Tends to force fluids through capillary walls – Greater at arterial end (35 mm Hg) of bed than at venule end (17 mm Hg) • Interstitial fluid hydrostatic pressure (HPif) – Pressure that would push fluid into vessel – Usually assumed to be zero because of lymphatic vessels © 2013 Pearson Education, Inc. Colloid Osmotic Pressures • Capillary colloid osmotic pressure (oncotic pressure) (OPc) – Created by nondiffusible plasma proteins, which draw water toward themselves – ~26 mm Hg • Interstitial fluid osmotic pressure (OPif) – Low (~1 mm Hg) due to low protein content © 2013 Pearson Education, Inc. Hydrostatic-osmotic Pressure Interactions: Net Filtration Pressure (NFP) • NFP—comprises all forces acting on capillary bed – NFP = (HPc + OPif) – (HPif + OPc) • Net fluid flow out at arterial end • Net fluid flow in at venous end • More leaves than is returned – Excess fluid returned to blood via lymphatic system © 2013 Pearson Education, Inc. Figure 19.17 Bulk fluid flow across capillary walls causes continuous mixing of fluid between the plasma and the interstitial fluid compartments, and maintains the interstitial environment. (1 of 5) The big picture Fluid filters from capillaries at their arteriolar end and flows through the interstitial space. Most is reabsorbed at the venous end. Arteriole Fluid moves through the interstitial space. For all capillary beds, 20 L of fluid is filtered out per day—almost 7 times the total plasma volume! Net filtration pressure (NFP) determines the direction of fluid movement. Two kinds of pressure drive fluid flow: Hydrostatic pressure (HP) • Due to fluid pressing against a boundary • HP “pushes” fluid across the boundary • In blood vessels, is due to blood pressure Osmotic pressure (OP) • Due to nondiffusible solutes that cannot cross the boundary • OP “pulls” fluid across the boundary • In blood vessels, is due to plasma proteins Piston Boundary “Pushes” Solute molecules (proteins) 17 L of fluid per day is reabsorbed into the capillaries at the venous end. Boundary “Pulls” Venule © 2013 Pearson Education, Inc. About 3 L per day of fluid (and any leaked proteins) are removed by the lymphatic system (see Chapter 20). Lymphatic capillary Figure 19.17 Bulk fluid flow across capillary walls causes continuous mixing of fluid between the plasma and the interstitial fluid compartments, and maintains the interstitial environment. (3 of 5) Net filtration pressure (NFP) determines the direction of fluid movement. Two kinds of pressure drive fluid flow: Hydrostatic pressure (HP) Osmotic pressure (OP) • Due to fluid pressing against a boundary • HP “pushes” fluid across the boundary • In blood vessels, is due to blood pressure • Due to nondiffusible solutes that cannot cross the boundary • OP “pulls” fluid across the boundary • In blood vessels, is due to plasma proteins Piston Solute molecules (proteins) Boundary “Pushes” © 2013 Pearson Education, Inc. “Pulls” Boundary Figure 19.17 Bulk fluid flow across capillary walls causes continuous mixing of fluid between the plasma and the interstitial fluid compartments, and maintains the interstitial environment. (4 of 5) How do the pressures drive fluid flow across a capillary? Net filtration occurs at the arteriolar end of a capillary. Capillary Hydrostatic pressure in capillary “pushes” fluid out of capillary. Osmotic pressure in capillary “pulls” fluid into capillary. Boundary (capillary wall) HPc = 35 mm Hg OPc = 26 mm Hg HPif = 0 mm Hg OPif = 1 mm Hg NFP = 10 mm Hg © 2013 Pearson Education, Inc. Interstitial fluid Hydrostatic pressure in interstitial fluid “pushes” fluid into capillary. Osmotic pressure in interstitial fluid “pulls” fluid out of capillary. To determine the pressure driving the fluid out of the capillary at any given point, we calculate the net filtration pressure (NFP)––the outward pressures (HPc and OPif) minus the inward pressures (HPif and OPc). So, NFP = (HPc + OPif) – (HPif + OPc) = (35 + 1) – (0 + 26) = 10 mm Hg (net outward pressure) As a result, fluid moves from the capillary into the interstitial space. Figure 19.17 Bulk fluid flow across capillary walls causes continuous mixing of fluid between the plasma and the interstitial fluid compartments, and maintains the interstitial environment. (5 of 5) Net reabsorption occurs at the venous end of a capillary. Boundary (capillary wall) Capillary Interstitial fluid Hydrostatic pressure in capillary HPc = 17 mm Hg “pushes” fluid out of capillary. The pressure has dropped because of resistance encountered along the capillaries. Osmotic pressure in capillary “pulls” fluid into capillary. OPc = 26 mm Hg HPif = 0 mm Hg Hydrostatic pressure in interstitial fluid “pushes” fluid into capillary. OPif = 1 mm Hg Osmotic pressure in interstitial fluid “pulls” fluid out of capillary. NFP= –8 mm Hg © 2013 Pearson Education, Inc. Again, we calculate the NFP: NFP = (HPc + OPif) – (HPif + OPc) = (17 + 1) – (0 + 26) = –8 mm Hg (net inward pressure) Notice that the NFP at the venous end is a negative number. This means that reabsorption, not filtration, is occurring and so fluid moves from the interstitial space into the capillary. Circulatory Shock • Any condition in which – Blood vessels inadequately filled – Blood cannot circulate normally • Results in inadequate blood flow to meet tissue needs © 2013 Pearson Education, Inc. Circulatory Shock • Hypovolemic shock: results from largescale blood loss • Vascular shock: results from extreme vasodilation and decreased peripheral resistance • Cardiogenic shock results when an inefficient heart cannot sustain adequate circulation © 2013 Pearson Education, Inc. Figure 19.18 Events and signs of hypovolemic shock. Acute bleeding (or other events that reduce blood volume) leads to: 1. Inadequate tissue perfusion resulting in O2 and nutrients to cells Initial stimulus Physiological response Signs and symptoms Result 2. Anaerobic metabolism by cells, so lactic acid accumulates 3. Movement of interstitial fluid into blood, so tissues dehydrate Chemoreceptors activated (by in blood pH) Baroreceptor firing reduced (by blood volume and pressure) Hypothalamus activated (by blood pressure) Brain Minor effect Major effect Respiratory centers activated Cardioacceleratory and vasomotor centers activated Heart rate Sympathetic nervous system activated ADH released Neurons depressed by pH Intense vasoconstriction (only heart and brain spared) Central nervous system depressed Kidneys Renal blood flow Adrenal cortex Renin released Angiotensin II produced in blood Aldosterone released Rate and depth of breathing CO2 blown off; blood pH rises © 2013 Pearson Education, Inc. Tachycardia; weak, thready pulse Kidneys retain salt and water Skin becomes cold, clammy, and cyanotic Blood pressure maintained; if fluid volume continues to decrease, BP ultimately drops. BP is a late sign. Water retention Urine output Thirst Restlessness (early sign) Coma (late sign) Circulatory Pathways: Blood Vessels of the Body • Two main circulations – Pulmonary circulation: short loop that runs from heart to lungs and back to heart – Systemic circulation: long loop to all parts of body and back to heart © 2013 Pearson Education, Inc. Figure 19.19a Pulmonary circulation. Pulmonary capillaries of the R. lung R. pulmonary artery Pulmonary capillaries of the L. lung L. pulmonary artery To systemic circulation Pulmonary trunk R. pulmonary veins From systemic circulation LA RA L. pulmonary veins RV © 2013 Pearson Education, Inc. Schematic flowchart. LV Figure 19.19 Pulmonary circulation. Pulmonary capillaries of the R. lung Pulmonary capillaries of the L. lung R. pulmonary L. pulmonary artery artery To systemic circulation Pulmonary trunk R. pulmonary veins From systemic circulation RA LA RV LV L. pulmonary veins Schematic flowchart. Left pulmonary artery Air-filled alveolus of lung Aortic arch Pulmonary trunk Right pulmonary artery Three lobar arteries to right lung Pulmonary capillary Gas exchange Two lobar arteries to left lung Pulmonary veins Pulmonary veins Right atrium Left atrium Right ventricle Left ventricle Illustration. The pulmonary arterial system is shown in blue to indicate that the blood it carries is oxygen-poor. The pulmonary venous drainage is shown in red to indicate that the blood it transports is oxygen-rich. © 2013 Pearson Education, Inc. Figure 19.20 Schematic flowchart showing an overview of the systemic circulation. Common carotid arteries to head and subclavian arteries to upper limbs Capillary beds of head and upper limbs Superior vena cava Aortic arch Aorta RA LA RV LV Azygos system Venous drainage Inferior vena cava Thoracic aorta Arterial blood Capillary beds of mediastinal structures and thorax walls Diaphragm Abdominal aorta Inferior vena cava © 2013 Pearson Education, Inc. Capillary beds of digestive viscera, spleen, pancreas, kidneys Capillary beds of gonads, pelvis, and lower limbs Differences Between Arteries and Veins Arteries Veins Delivery Blood pumped into single systemic artery—the aorta Blood returns via superior and inferior venae cavae and the coronary sinus Location Deep, and protected by tissues Both deep and superficial Pathways Fairly distinct Numerous interconnections Supply/drainage Predictable supply Usually similar to arteries, except dural sinuses and hepatic portal circulation © 2013 Pearson Education, Inc.