Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
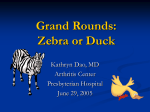
Current practice Ann Biol Clin 2014; 72 (2): 245-8 Knee brown tumor revealing a primary hyperparathyroidism: a case report Copyright © 2017 John Libbey Eurotext. Téléchargé par un robot venant de 88.99.165.207 le 17/06/2017. Tumeur brune du genou révélant une hyperparathyroïdie primitive : à propos d’un cas Aoulia Dekaken1 Adel Gouri2 Ahmed Aimen Bentorki1 Amina Yakhlef3 1 Department of internal medicine and cardiology, El Okbi Hospital, Guelma, Algeria <[email protected]> 2 Laboratory of medical biochemistry, IBN Zohr Hospital, Guelma, Algeria Abstract. Primary hyperparathyroidism is a common endocrine disorder, asymptomatic and diagnosed through a fortuitous hypercalcemia. Brown tumors are exceptional but severe hyperparathyroidism bone complications. We report in this paper an original observation of hyperparathyroidism due to a parathyroid adenoma presenting as a brown tumor. A 28 year-old girl admitted for a bone tumor of the knee, the blood test shows hypercalcemia with hyperparathyroidism, bone biopsy revealed giant cell lesions characteristic of brown tumors. Key words: hyperparathyroidism, brown tumor, giant-cell tumor 3 Department of hematology, IBN Zohr Hospital, Guelma, Algeria doi:10.1684/abc.2014.0934 Article received November 07, 2013, accepted November 12, 2013 Résumé. L’hyperparathyroïdie primitive est une endocrinopathie fréquente, le plus souvent asymptomatique et diagnostiquée à l’occasion d’une hypercalcémie de découverte fortuite. Les tumeurs brunes sont des complications osseuses exceptionnelles mais sévères de l’hyperparathyroïdie. Nous rapportons ici une découverte originale d’une hyperparathyroïdie due à un adénome parathyroïdien devant une tumeur brune. Il s’agit d’une femme âgée de 28 ans admise pour une tumeur osseuse du genou, l’examen biologique montre une hypercalcémie avec une hyperparathyroïdie, la biopsie osseuse révèle des lésions osseuses à cellule géantes caractéristiques des tumeurs brunes. Mots clés : hyperparathyroïdie, tumeur brune, tumeur à cellule géante Primary hyperparathyroidism (PHP) is a common endocrine disorder characterized by an excessive secretion of parathyroid hormone (PTH) and consequent hypercalcaemia [1]. The frequency of bone disease has been reported to be around 10-15%. Brown tumor is a rare aspect of its manifestations (2 -3%) and is exceptionally revealing of the disease [2-4]. Brown tumor is not neoplastic bone lesion caused by rapid osteoclastic activity due to hyperparathyroidism (HPT) resulting in a locally destructive phenomenon. In regions where bone loss is rapid, hemorrhage, hemosiderin deposition, and vascularized fibrous tissue replace the normal bone contents, resulting in a reddish-brown appearance [5]. Common sites of brown tumor are the ribs, clavicle, tibia, femur and pelvic girdle. We report an unusual case in which primary hyperparathyroidism was diagnosed upon investigation of knee bone manifestations caused by brown tumor. We also summarize several critical radiological and clinical points that are easily missed and should be kept in mind. Case report A 28-year-old woman married and mother of four children was admitted at the internal medicine department exploring a bone tumor discovered through radiographs. The patient had a history of pain in the left knee for several months prompted radiographs of the knees, which showed lytic lesions (figure 1). Here medical history was unremarkable. At admission, mild asthenia and polydipsia-polyuria syndrome were noted. Mechanical diffuse pain, lower extremity motor weakness and arthritis of the left knee were the only musculoskeletal abnormalities. No other significant clinical abnormality was observed. To cite this article: Dekaken A, Gouri A, Bentorki AA, Yakhlef A. Knee brown tumor revealed primary hyperparathyroidism: a case report. Ann Biol Clin 2014; 72(2): 245-8 doi:10.1684/abc.2014.0934 245 Copyright © 2017 John Libbey Eurotext. Téléchargé par un robot venant de 88.99.165.207 le 17/06/2017. Current practice B. Plain radiograph of femur llustrate abnormal bony architecture in lateral femoral condyle. A. Plain radiograph of knee joint llustrate abnormal bony architecture in patella and tibial tuberosity. Figure 1. Radiographs of the left knee. A. Plain radiograph of knee joint (illustrate abnormal bony architecture in patella and tibial tuberosity). B. Plain radiograph of femur (Illustrate abnormal bony architecture in lateral femoral condyle). Laboratory analysis showed an elevated serum calcium level of 3.04 mmol/L (reference range, 2.15-2.50 mmol/L) and a low serum phosphate level of 0.63 mmol/L (reference range: 0.77-1.32 mg/L), and normal tests for inflammation. Urinary phosphate excretion was increased to 26 mmol/24h (reference range: 10 à 20 mmol/24h) and urinary calcium excretion to 10 mmol/24 h (reference range, 3.5 à 7.5 mmol/24h).The serum alkaline phosphatase level was 890 IU/L (reference range, 50-240 IU/L). Subsequent testing revealed normal renal function tests and a high intact PTH level of 137 pmol/L (reference range: 1.2-5.8 pmol/L), confirming primary hyperparathyroidism. Both liver and thyroid function were normal, serology for viral hepatitis B and C was negative (table 1). The radiographs of the left knee showed the previously noted lytic lesions, as well as articular chondrocalcinosis, which were subsequently found to be diffuse. The parathyroid scintigraphy (Tc99 m sestamibi) clearly locates a parathyroid adenoma (30 × 16 mm) in the lower pole of the right lobe of the thyroid gland. Computed tomography (CT) scan of the left knee disclosed three osteolytic lesions (lateral femoral condyle, patella and tibial tuberosity). 246 Table 1. Biological data on admission. Laboratory exam Hematocrit (%) Erythrocyte sedimentation rate (mm) Albumin (g/L) Fasting blood sugar (mmol/L) Total cholesterol (mmol/L) Triglycerides (mmol/L) Total bilirubin (mol/L) Aspartate aminotransferase (UI/L) Alanine aminotransferase (UI/L) Alkaline phosphatase (UI/L) Lactate dehydrogenase Serum calcium (mmol/L) Serum phosphate (mmol/L) Urinary calcium (mmol/24 h) Urinary phosphate (mmol/24 h) Creatinine (mol/L) Urea (mmol/L) Parathyroid hormone (pmol/L) Thyroid-stimulating hormone (mIU/L) Free triiodothyronine (pmol/L) Free thyroxine (pmol/L) Result (reference ranges) 34% (31-36) 15 (<20) 42 (35-50) 5,6 (3.3-6.1) 4,6 (3.4-6.4) 1.2 (0.4-1.9) 7 (1-12) 21 (5-45) 16 (5-45) 890 (50-240) 320 (230-460) 3.03 (2.1-2.6) 0.63 (0.80-1.61) 10 (3.5-7.5) 26 (10-20) 68 (53-97) 5.20 (2.49-7.49) 137 (1.2-5.8) 1.58 (0.5-4.70) 4.23 (3.5-6.5) 15.12 (10-23) Ann Biol Clin, vol. 72, n◦ 2, mars-avril 2014 Copyright © 2017 John Libbey Eurotext. Téléchargé par un robot venant de 88.99.165.207 le 17/06/2017. Knee brown tumor and hyperparathyroidism To arrive at conclusive diagnosis, pathological analysis was performed. Biopsy specimens were obtained from different zones of the lesion and at different depths. Histopathological studies revealed the presence of a giant cell granuloma with microscopic features suggest hyperparathyroidism. The envisaged diagnosis was primary hyperparathyroidism with brown tumor on the above of laboratory data and characteristic histopathologic findings. Subtotal parathyroidectomia was performed and improvement in the patient’s clinical condition and radiological findings was marked in few months. tests including PTH level will differentiate primary hyperparathyroidism from other giant cell lesions which have similar histological appearances such as giant cell granuloma, aneurysmal bone cyst, cherubism, and giant cell tumor [11]. The management of a brown tumor depends on the severity of the lesion present and treatment of hyperparathyroidism is the first step. Parathyroidectomy is the treatment of choice, various studies have demonstrated regression of skeletal and normalization of the biochemical aspects of the disease promptly [12, 13]. Conclusion Discussion Primary hyperparathyroidism is an endocrine disease that results from autonomous overproduction of the parathyroid hormone; it is the third most common endocrine disorder after diabetes and thyroid disorder [6, 7]. This case report illustrates the classic but rarely inaugural bone manifestations of primary hyperparathyroidism. Due to the improved laboratory methods and clinical practice in the last 2 decades, most of the recent cases of primary hyperparathyroidism are diagnosed early and asymptomatically. This makes advanced disease with bone lesions extremely rare these days. Only 2% of all cases of primary hyperparathyroidism occur below the age of 30 years at the time of diagnosis [8]. The patient reported here is in this rare group because she was only 28 years old at the time of diagnosis and the extent of her disease suggested that it had been present for some time. Increased levels of serum calcium and parathyroid hormones and reduced levels of serum phosphate as well as increased urinary levels of phosphates and calcium observed in this patient were sufficient to diagnose primary hyperparathyroidism. Ultrasound, CT scan, or technetium scan techniques can be used also to detect the diseased parathyroid gland. Brown tumors represent a serious complication of advanced hyperparathyroidism with a frequency of 3-4% in primary hyperparathyroidism [9]. It affects usually young people especially females with varying degrees of aggressiveness and risks of recurrence. The usual sites of these lesions are the ribs, clavicles, pelvic girdle and facial bones and the presentation may be a pathological fracture [10]. The lower limb is rarely affected. In our case the tumor is involving the left knee articulation; lateral femoral condyle, patella and tibial tuberosity. The diagnosis of a brown tumor is the result of the sum of the medical history of patients with clinical, radiographic, laboratory findings and histological examination. Incisional biopsy will show a giant cell lesion, and only biochemical Ann Biol Clin, vol. 72, n◦ 2, mars-avril 2014 This case should attract the attention of clinical practitioner that brown tumor should be kept in mind during daily practice and in the case of hypercalcemia and radiographic evidence of multiple lytic lesion, primary hyperparathyroidism should always be kept in differential diagnosis and should be looked into once more common causes. Conflicts of interest: none. References 1. Al Zahrani A, Levine MA. Primary hyperparathyroidism. Lancet 1997 ; 349 : 1233-8. 2. Silverburg SJ, Bilezikian JP. Evaluation and management of primary hyperparathyroidism. J Clin Endocrinol Metab 1996 ; 81 : 2036-40. 3. Al-Gahtany M, Cusimano M, Singer W, Bilbao J, Kovacs K, Marotta T. Brown tumors of the skull base: case report and review of the literature. J Neurosurg 2003 ; 98 : 417-20. 4. Emin AH, Suoglu Y, Demir D, Karatay MC. Normocalcemic hyperparathyroidism presented with mandibular brown tumor: report of a case. Auris Nasus Larynx 2004 ; 31 : 299-304. 5. Al-Gahtany M, Cusimano M, Singer W, Bilbao J, Kovacs K, Marotta T. Brown tumors of the skull base: case report and review of the literature. J Neurosurg 2003 ; 98 : 417-20. 6. Jouan A, Zabraniecki L, Vincent V, Poix E, Fournie B. An unusual presentation of primary hyperparathyroidism: severe hypercalcemia and multiple brown tumors. Joint Bone Spine 2008 ; 75 : 209-11. 7. Kukora JS, Zeiger MA, Clark OH, Grant CS, Hodgson SF, Irvin III GL, et al. The American association of clinical endocrinologist and The American association of endocrine surgeons position statement on the diagnosis and management of primary hyperparathyroidism. Endocr Pract 2005 ; 11 : 49-54. 8. Mundy GR, Cove DH, Fisken R. Primary hyperparathyroidism; changes in the pattern of clinical presentation. Lancet 1980 ; 1 : 1317-20. 9. Di Daniele N, Condò S, Ferrannini M, Bertoli M, Rovella V, Di Renzo L, et al. Brown tumour in a patient with secondary hyperparathyroidism resistant to medical therapy: case report on successful treatment after subtotal parathyroidectomy. Int J Endocrinol 2009 ; 2009 : 827-52. 247 Current practice 12. Scott SN, Graham SM, Sato Y, Robinson RA. Brown tumor of the palate in a patient with primary hyperparathyroidism. Ann Otol Rhinol Laryngol 1999 ; 108 : 91-4. 11. Daniels JS. Primary hyperparathyroidism presenting as a palatal brown tumor. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004 ; 98 : 409-13. 13. Smith BR, Fowler CB, Svane TJ. Primary hyperparathyroidism presenting as a “peripheral” giant cell granuloma. J Oral Maxillofac Surg 1988 ; 46 : 65-9. Copyright © 2017 John Libbey Eurotext. Téléchargé par un robot venant de 88.99.165.207 le 17/06/2017. 10. Goshen O, Aviel-Ronen S, Dori S, Talmi YP. Brown tumour of hyperparathyroidism in the mandible associated with atypical parathyroid adenoma. J Laryngol Otol 2000 ; 114 : 302-4. 248 Ann Biol Clin, vol. 72, n◦ 2, mars-avril 2014