Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
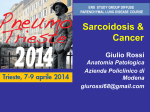
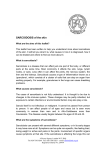
CUTANEOUS SARCOIDOSIS Professor Svyatenko T.V. Dnepropetrovsk Medical Academy, Ukraine Center Dermatology and Cosmetology, Dnepropetrovsk, Ukraine Introductions • Sarcoidosis is a multisystem disease that may involve almost any organ system; therefore, it results in various clinical manifestations. • Cutaneous sarcoidosis occurs in up to one third of patients with systemic sarcoidosis. • Recognition of cutaneous lesions is important because they provide a visible clue to the diagnosis and are an easily accessible source of tissue for histologic examination. • Because lesions can exhibit many different morphologies, cutaneous sarcoidosis is known as one of the “great imitators” in dermatology. Specific manifestations include papules, plaques, lupus pernio, scar sarcoidosis, and rare morphologies such as alopecia, ulcers, hypopigmented patches, and ichthyosis. • Most authors divide lesions of cutaneous sarcoidosis into nonspecific and specific types. Although nonspecific lesions occur in association with systemic sarcoidosis, no granulomas are found on biopsy. Specific lesions display noncaseating granulomas on biopsy • Correctly diagnosing sarcoidosis may be a challenge. Unfortunately, no single test can prove the diagnosis. Patients are diagnosed with sarcoidosis when a compatible clinical or radiologic picture is present, along with histologic evidence of noncaseating granulomas, and when other potential causes, such as infections, are excluded • The treatment of cutaneous sarcoidosis is often frustrating, because lesions may be refractory to treatment or may recur following successful treatment. For localized involvement, topical or intralesional steroids are used. Physicians frequently attempt to use superpotent topical steroids because of their occasional effectiveness. However, these steroids often do not adequately penetrate the skin lesion. Intralesional steroids (e.g., triamcinolone acetonide [Kenalog] in a dosage of 5 mg per mL) are typically more effective, with injections repeated at two- to three-week intervals. • Systemic agents are reserved for widespread, progressive lesions or those that impair function. Systemic glucocorticoids are the most effective agents. They are commonly used at slow, tapering dosages, starting at 20 to 40 mg of oral prednisone daily for four to six weeks. However, there are many drawbacks to this therapy • Many other medications may be used in refractory cases, including such agents as hydroxychloroquine (Plaquenil), methotrexate (Rheumatrex), and thalidomide (Thalomid). • Although randomized, controlled trials are lacking, multiple anecdotal reports suggest the efficacy of these agents. RAJANI KATTA Cutaneous Sarcoidosis: A Dermatologic Masquerader // Am Fam Physician. 2002 ,15;65(8):15811585. CASE № 1. CUTANEOUS SARCOIDOSIS • • • • • • • • 49-year-old male patient, Caucasian Reason for visit skin rash in the area of the upper third of the back slightly itching after exercise in the summer time. Medical history: according to the patient, the rash appeared all of a sudden 2 years ago, with no pain or severe itching. No triggering accidents can be recalled. The process progresses slowly. He repeatedly contacted dermatologists and was treated with the diagnosis: multiple warts? Lichen planus? Atopic dermatitis? – without any effects, also after administration of the local and oral corticosteroids therapy a positive effect was observed for a short period of time. On the medical examination no physical complaints were made. Patient also has a history of atopic dermatitis when was a child, androgenetic hair loss. The parents and close relatives are healthy. Job is not associated with negative factors. During the examination patient physical condition was satisfactory. Pathological skin process is localized on the upper back. Rush is represented by single knots, up to 2 - 5 mm in diameter, multiple scattered and confluent lesions up to 3 cm in diameter, fused into plaques, the colour red and pink, pink stagnant, with telangiectasias, soft-elastic consistency, the surface smooth and shiny. On diascopy symptom of "dust", the phenomenon of "cape". Blood test results: normal range Punch biopsy was provided Histological investigation showed epidermis without changes, multiple epithelioid - cell granulomas are determined in papillary and reticular dermis with the presence of single giant polynuclear cells. Granulomas have clear boundaries, with the presence of single lymphocytes around some of them. When painting on Alcian blue PAS + cells of fungi have been identified. The basement membrane is within norm. No dermal mucin. • Sarcoidosis is one of the most common granulomatosis. While there is a steady gradual increase in the frequency of this disease. An important feature is the presence of nosology many similarities with tuberculosis, lymphoproliferative and other cancers , various autoimmune diseases. In sarcoidosis often affects many organs, in this regard, the ill person may apply to the primary physicians of different specialties: dermatologist, ophthalmologist, neurologist, surgeon, oncologist. CASE № 2. SARCOIDOSIS COMBINED WITH SKIN LESIONS • 46-year-old male patient, Caucasian • Reason for visit: - skin lesions since age 34 • Medical history: – No personal history of any skin diseases previously, otherwise in good general health. – For the last 34 years from the first manifestation of skin lesions, the patient consulted various doctors – Patient was treated for lichen planus, lichen simplex chronicus Vidal, psoriasis – Laboratory findings were within normal range – Skin biopsy was performed. Histological investigation showed productive chronic inflammation with the formation of epithelioid cell granulomas, the presence of multinucleated giant cells Pirogov-Langhans. Information of common status Spiral computed tomography of the thoracic cavity : multiple foci of 1-2 mm d in both lungs, increased pulmonary pattern, the expansion of the lung roots mediastinal lymphadenopathy. According to ultrosound, peripheral lymph nodes: generalized hyperplasia of the peripheral lymph nodes, splenomegaly. CASE № 2. SARCOIDOSIS COMBINED WITH SKIN LESIONS • 76-year-old male patient, Caucasian • Reason for visit: - skin lesions since age 72 • Medical history: – No personal history of any skin diseases previously, otherwise in good general health. – For the last 72 years from the first manifestation of skin lesions, the patient consulted various doctors – Patient was treated for lichen planus? lymphoma? – Laboratory findings were within normal range – Skin biopsy was performed. Information of common status • Spiral computed tomography of the thoracic cavity : multiple foci of 3-4 mm d in both lungs, increased pulmonary pattern, the expansion of the lung roots mediastinal lymphadenopathy. Spiral computed tomography of the lumbar spine spondyloarthrosis with disc protrusion, diffuse osteoporosis • According to ultrosound, peripheral lymph nodes: generalized hyperplasia of the peripheral lymph nodes, splenomegaly. According to ultrosound - prostatitis • Histological investigation showed productive chronic inflammation with the formation of epithelioid cell granulomas, the presence of multinucleated giant cells Pirogov-Langhans. • Results immunohistochemistry - granulomatous inflammation with the presence of giant cells of Pirogov-Langhans, sarcoidosis CONCLUSION • 1. In our opinion, the case described introduce certain interest in the daily practice of a physician - clinician. • 2. This condition is rare and difficult to diagnose. In this case, the punch - biopsy followed by histological examination of biopsy is an important diagnostic tool to verify the diagnosis of skin sarcoidosis. • 3. With correct diagnosis and proper management, most patients with sarcoidosis continue to lead a normal life. Thank you for attention!