Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
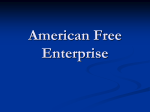
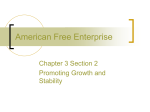
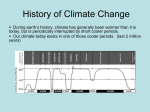
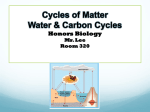
Human Reproduction vol.12 no.12 pp.2607–2613, 1997 Preimplantation hormonal differences between the conception and non-conception menstrual cycles of 32 normal women D.D.Baird1,7, A.J.Wilcox1, C.R.Weinberg2, F.Kamel1, D.R.McConnaughey3, P.I.Musey4 and D.C.Collins5,6 1Epidemiology Branch and 2Statistics and Biomathematics Branch, National Institute of Environmental Health Sciences, Research Triangle Park, NC 27709, 3Westat Inc., Research Triangle Park, NC 27709, 4Department of Biology, Clark-Atlanta University, Atlanta, GA 30314 and 5Veteran’s Administration Medical Center and Emory University School of Medicine, Decatur, GA 30329, USA 6Present address: Veteran’s Administration Medical Center, Lexington, KY 40511, USA 7To whom correspondence should be addressed We compared daily urinary concentrations of oestrogen and progesterone metabolites in paired menstrual cycles (conception and non-conception) from 32 women. Volunteers with no known fertility problems were enrolled in the study at the time they began trying to become pregnant. They collected first-morning urine specimens and kept daily records of menstrual bleeding and sexual intercourse for 6 months or until they became clinically pregnant. Intercourse in non-conception cycles was close to the time of ovulation so that failure to conceive was caused by factors other than poorly timed intercourse. Compared with non-conception cycles, conception cycles had a steeper early luteal rise in progesterone and higher mid-luteal oestrogen and progesterone concentrations. These hormonal characteristics may be markers of better quality cycles, but because all these differences were in the luteal phase, we cannot rule out the possibility that the preimplantation embryo had stimulated early increases in steroid production. We propose an analysis strategy that could help support or refute the importance of preimplantation embryonic signalling, but our small sample size limits our own conclusions about this mechanism. Key words: fertility/oestrogen/progesterone/unassisted conception in fertile women. If a successful pregnancy is conceived in a given menstrual cycle, then that cycle must have been hormonally adequate. However, if no recognized pregnancy occurs, even with well-timed intercourse, inadequate hormonal conditions may have interfered with fertilization, early development or implantation. Few data are available on conception cycles from normal women free of exogenous ovarian stimulation. Lenton et al. (1982) reported data from 26 conception cycles, but 22 were from infertility patients, 12 of whom were taking fertility drugs. Several other publications report measurements from small samples of women (Branch et al., 1980; Coutts, 1985; Lenton et al., 1991) or from a small part of the cycle (Irianni et al., 1992). Two studies provide most of the available data. Stewart et al. (1993) reported serum oestrogen and progesterone concentrations from 14 natural conception cycles. These cycles showed higher luteal oestrogen and progesterone concentrations compared with non-conception cycles. Lipson and Ellison (1996) reported salivary oestrogen and progesterone concentrations in 17 conception cycles. These cycles did not differ from non-conception cycles in progesterone, but conception cycles had higher oestrogen throughout, especially during the mid-follicular phase. The purpose of this study was to characterize hormonal patterns associated with successful conception in a larger sample of natural cycles. We compared daily concentrations of urinary oestrogen and progesterone metabolites in paired conception and non-conception cycles from 32 women who conceived within 6 months of stopping contraception. In addition, we considered whether hormonal differences between conception and non-conception cycles after the time of fertilization represented an early response of the ovary to some signal from the preimplantation conceptus, or whether such differences reflected a better quality ovarian cycle more able to support pregnancy. Materials and methods Introduction Amounts of ovarian oestrogen and progesterone production vary from woman to woman. Variability also occurs from menstrual cycle to menstrual cycle within individual women. Certain extreme hormonal conditions reflect impaired fertility, such as the low luteal progesterone production seen in lactating women (Diaz et al., 1992). It is not clear to what degree the variability from cycle to cycle in non-lactating women might influence the likelihood of successful pregnancy. One way to study this is to compare conception and non-conception cycles © European Society for Human Reproduction and Embryology Women in our sample were participants in a larger study in which pregnancies were identified at the first detectable rise in urinary human chorionic gonadotrophin (HCG), measured by a highly sensitive immunoradiometric assay. The methods employed have been described in detail elsewhere (Wilcox et al., 1988). Briefly, volunteers enrolled in the study at or before the time they stopped using contraception with the intention of becoming pregnant. Women were excluded from the study if they had any chronic diseases or known fertility problems, but there were no exclusions based on the length or regularity of their menstrual cycles. Volunteers collected firstmorning urine specimens each day until they became clinically pregnant or for 6 months if no clinical pregnancy ensued. Each 2607 D.D.Baird et al. morning, participants recorded menstrual bleeding and whether or not they had had sexual intercourse in the previous 24 h. First-morning urine specimens were assayed for oestrone-3-glucuronide (E1G) and pregnanediol-3-glucuronide (PdG) by direct radioimmunoassay procedures using highly specific male rabbit antisera raised against PdG–bovine serum albumin (BSA) and E1G–BSA respectively (Wright et al., 1978; Samarajeewa et al., 1979). Both antisera had no cross-reactions to any other urinary steroid conjugates, except for oestrone sulphate which showed 3.7% cross-reaction with E1G antiserum. However, each antiserum showed significant crossreaction with its respective unconjugated steroid, pregnanediol and oestrone. In general, urinary steroids are excreted in the conjugated form primarily as glucuronides, with unconjugated steroids accounting for 3–9% (Eren et al., 1967). While unconjugated oestrone is found in urine, unconjugated pregnanediol is not known to be excreted. Daily urine specimens were assayed in duplicate or triplicate at 1000and 2000-fold dilutions, thus nullifying interference caused by other steroids. Intra-and interassay coefficients of variation were 5 and 6% for E1G, and 9 and 11% for PdG respectively. Because specimens for a given woman were analysed in the same assay, only the intraassay variability was relevant. Geometric means of daily replicates were divided by the respective daily creatinine concentration to correct for variations in the dilution of the urine specimen. Menstrual cycles were defined by bleeding days, with the first bleeding day taken as the first day of the cycle. We estimated the day of ovulation for each cycle (designated luteal day 0) using the ratio of the urinary steroid metabolites. This method takes advantage of the drop in oestrogen and rise in progesterone that occurs at around the time of ovulation. The oestrogen:progesterone ratio drops steeply as the follicle luteinizes, and remains low through the luteal phase of an ovulatory cycle. This method was proposed by Baker et al. (1980), modified by Royston (1983), and further refined and validated with urinary luteinizing hormone (LH) measurements by Baird et al. (1991). As a marker of ovulation, it appears to have as little measurement error as plasma LH (Baird et al., 1995). Figure 1 shows an example of hormonal and intercourse data for the paired menstrual cycles from one woman. In each cycle E1G rises to a peak just prior to luteal day 0, and PdG rises in the luteal phase. The conception cycle shows the rapid rise of HCG beginning on luteal day 8. The sample of women used in our analysis was selected as follows. In the larger study, 130 of 221 participants conceived a singleton live birth. Of these, 84 women were in the study for at least one menstrual cycle before conceiving. Hormone assays were run on all available daily urine specimens for 65 of these women. Twelve women were missing ù7 days of hormone data in one of their paired cycles, leaving 53 women with adequate hormone data. Frequency and timing of sexual intercourse varied among menstrual cycles, and conception failed in some cycles simply because there was no intercourse at around the time of ovulation. To include these non-conception cycles, which were potentially hormonally adequate, would reduce our ability to identify endocrine patterns associated with successful conception. We avoided this problem by excluding non-conception cycles with poorly timed sexual intercourse. We used a method of estimating the likelihood of conception for various patterns of sexual intercourse at around the time of ovulation (Weinberg et al., 1994) and included only non-conception cycles with very favourable timing of intercourse, i.e. cycles with intercourse reported for the estimated day of ovulation or the day before. Of the 53 women with adequate hormone data, 21 lacked a nonconception cycle with well-timed intercourse. This left 32 women with paired conception and non-conception cycles. When a woman had more than one eligible non-conception cycle, the one with the 2608 Figure 1. An example of the hormonal and intercourse data for the paired non-conception and conception cycles from a single woman. The shaded bars show days of menstrual bleeding. The top panel shows daily creatinine-corrected concentrations of oestrone-3glucuronide (E1G) and pregnanediol-3-glucuronide (PdG). The second panel shows the ratio of E1G to PdG. Note the vertical dotted line showing luteal day 0 (the estimated day of ovulation), when the ratio dropped precipitously. The next panel shows days of sexual intercourse. The final panel presents concentrations of human chorionic gonadotrophin (HCG) showing a rapid rise in the luteal phase of the conception cycle. most favourable intercourse pattern was chosen. This strategy was designed to optimize our ability to detect hormonal patterns that characterize subfertile menstrual cycles. We plotted the daily steroid metabolite concentrations for conception and non-conception cycles, centred on luteal day 0, to compare differences in hormonal profiles. SE for each day’s values were calculated based on within-woman differences (on a logarithmic scale), thus avoiding any effects of subject-to-subject heterogeneity. That is, for each day of the cycle, we calculated the difference between the corresponding values in the two cycles from the same woman and averaged these differences across women. The SE of this mean difference for each day is comparable with the measure of variability used in a paired t-test. Formal statistical testing of hormone differences between conception and non-conception cycles was conducted with a set of preselected summary variables. This strategy limited the multiple comparisons problem that arises when hormonal measurements are compared daily. In this study we focused on preimplantation hormone patterns because postimplantation patterns are likely to reflect ovarian response to the conceptus. Thus, data are presented for ovarian hormones in the follicular phase and in the luteal phase up to the time of implantation, specifically through luteal day 6 (one woman showed her first elevated HCG on luteal day 6, while HCG was first seen on luteal day ù8 for the other 31 women in the sample). Definitions of summary variables for E1G, PdG and the E1G:PdG ratio are shown in Table I. Conception versus non-conception menstrual cycle hormonal differences Table I. Definitions of summary variables used to test for differences between hormone patterns in conception and non-conception cycles Summary variable Oestrone-3-glucuronide (E1G) Early follicular E1G Mid-follicular E1G Peak E1G Definition Geometric mean of E1G for first 6 days of menstrual cycle Geometric mean of E1G for the interval starting on day 5 of the cycle and ending 3 days before luteal day 0 (the estimated day of ovulation) Geometric mean of E1G for 3 days, centred on the highest mid-cycle E1G (the highest E1G concentration in a 16-day window ending on luteal day 3) Slope of 3 days of E1G, ending on the day before the highest mid-cycle concentration Geometric mean of E1G for luteal days 1–4 Geometric mean of E1G for luteal days 5 and 6 Rate of E1G rise Early luteal E1G Mid-luteal E1G Pregnanediol-3-glucuronide (PdG) Early follicular PdG Geometric mean of PdG during the first 6 days of the menstrual cycle Mid-follicular PdG Geometric mean of PdG for the interval starting on day 5 of the cycle and ending 3 days before luteal day 0 Early luteal PdG rise Slope of PdG for luteal days 1–5 Mid-luteal PdG Geometric mean of PdG for luteal day 5 and 6 Ratio (E1G:PdG) Ratio descent The 3-day slope of the ratio values around the estimated day of ovulation [For each cycle, slopes of days –1, 0, 1 and 0, 1, 2 relative to luteal day 0 were calculated, and the more negative (steeper) of the two was chosen to reflect the rapidity of the mid-cycle transition to the primarily progesterone-producing corpus luteum] Mid-luteal ratio Ratio of mid-luteal E1G and mid-luteal PdG The variables were calculated as mean concentrations or rates of change over specified intervals in the cycle. We subtracted the value of each summary variable in the non-conception cycle from the value in the conception cycle for the same woman. These differences were tested for statistical significance (α 5 0.05) using Wilcoxon’s signedrank test (Hollander and Wolfe, 1973). Results Demographic and menstrual cycle characteristics of the 32 women in our sample are shown in Table II. They ranged in age from 23 to 39 years, with a mean of 29 years. All but one of the women were Caucasian, and 91% had better than a high school education. In all, 10 of the women had never been pregnant before. The length of the non-conception menstrual cycle varied from 25 to 39 days, with an average of 30 days. In these characteristics the women were similar to the total sample of 221 women from the larger study. The time to achieve a pregnancy averaged four menstrual cycles. The length of the follicular phase varied from 9 to 33 days and was similar in the conception and non-conception cycles within women (correlation coefficient 5 0.50 for the pairs). Non-conception cycles were not more likely to have very short or very long follicular phases (Figure 2), nor was the average paired difference in follicular phase length between conception and non-conception cycles significantly different from zero. The hormonal profiles for the conception and non-conception cycles were similar during the follicular phase (Figure 3). However, in the luteal phase, conception cycles showed somewhat higher concentrations of both E1G and PdG. Examining our a-priori summary measures, there was a significantly steeper early luteal rise in PdG and higher mid-luteal E1G and PdG concentrations in conception cycles (Table III). In addition, the falling slope of the ratio of E1G:PdG (ratio descent) at the time of ovulation was steeper (more negative) in conception cycles. About two-thirds of the pairs had higher E1G concentrations in the conception cycles, and about two-thirds had higher PdG concentrations, but these were not the same two-thirds. A Table II. Demographic and menstrual cycle characteristics of the 32 women with both non-conception and conception cycles Number (%) Age (years) 20–24 3 (9) 25–29 16 (50) 30–34 10 (31) 35–39 3 (9) Prior pregnancies (n) 0 10 (31) 1 12 (38) 2 8 (25) ù3 2 (6) Smoking status Never 19 (59) Past 10 (31) Current 3 (9) Menstrual cycle length (non-conception cycle) (days) 25–26 3 (9) 27–28 13 (41) 29–30 3 (9) 31–32 8 (25) ù33 5 (16) Number of menstrual cycles to conception (n) 2 4 (12) 3 9 (28) 4 6 (19) 5 8 (25) ù6 5 (16) First day of human chorionic gonadotrophin rise (conception cycle) Luteal day 6 1 (3) Luteal day 7 0 (0) Luteal day 8 7 (23) Luteal day 9 10 (32) Luteal day 10 8 (26) Luteal day 11 4 (13) Luteal day 12 1 (3) higher mid-luteal E1G concentration was not closely associated with a higher mid-luteal PdG concentration, a stronger rise in PdG or a steeper ratio descent (Spearman r , 0.15 and P . 0.40 for all three Spearman correlations between difference variables). However, the differences between conception and non-conception cycles for the two progesterone measures were 2609 D.D.Baird et al. Figure 2. The distribution of follicular phase lengths in nonconception (top panel) and conception cycles (bottom panel) from 32 women. highly correlated (r 5 0.68) and they were weakly correlated with the difference in ratio descent (r 5 –0.20 and –0.24 for Spearman correlations with differences in the mid-luteal PdG and the early luteal PdG rise respectively). Non-conception cycles did not tend to have short luteal phases. Only three of the 32 luteal phases were ,12 days in length, and these did not differ much in the concentration of mid-luteal PdG from their respective conception cycles (mean of 2.7 versus 3.0 µg/ mg creatinine). The higher luteal hormone concentration in conception cycles is open to two alternative interpretations: (i) higher luteal hormone concentrations reflect an inherently better quality cycle for conception, or (ii) the early conceptus can stimulate hormone production. To pursue this question, we expanded our analysis to examine the hormone patterns from a subset of the women we had previously excluded. Of the 20 women who failed to have well-timed sexual intercourse during their non-conception cycle, we chose the eight pairs with relatively poorly timed intercourse in the nonconception cycle. The closest intercourse was ù3 days before the estimated day of ovulation, so the probability of conception was low, even if the cycle was adequate in other ways (Wilcox et al., 1995). The timing of the rise in HCG for the group of eight conceptions showed the same distribution as that for the group of 32, and all eight pregnancies led to full-term births. We postulated that if the higher luteal hormonal concentrations we had observed in the 32 pairs were a result of stimulation from the embryo, then the same hormonal differences should be apparent in these eight pairs as well. On the other hand, if the higher luteal hormone concentrations we saw in conception cycles from the 32 women reflect inherently better quality cycles, we would expect the differences between conception and non-conception cycles to be blunted in the group of eight. This is because many of the eight cycles would be expected 2610 Figure 3. Daily geometric means of oestrone-3-glucuronide (E1G; top panel) and pregnanediol-3-glucuronide (PdG; lower panel) for the paired conception (s) and non-conception (d) cycles from 32 women whose non-conception cycles had well-timed sexual intercourse. Data are centred on luteal day 0, the estimated day of ovulation (vertical dotted line). The SEs (shown by a single dotted line for each day) are based on within-woman differences between the two cycles, i.e. the difference between the corresponding daily values in the two cycles for each woman is calculated, these differences are averaged across women and the SE of the resultant mean difference is determined. to be hormonally adequate but to have failed just because of poorly timed intercourse, whereas the group of 32 were selected to include non-conception cycles which failed for some reason other than poorly timed intercourse. Figure 4 shows the daily profiles of oestrogen and progesterone metabolites in the paired cycles from the group of eight women. In contrast to the original 32 paired cycles, the luteal progesterone metabolite profiles in conception and nonconception cycles appeared similar, and the luteal oestrogen profiles appeared higher in the conception cycles only on luteal day 6. However, as in the previously described 32 pairs, the analysis of the mid-luteal E1G variable tended to be somewhat higher in the conception cycles (Table IV). Six of eight Conception versus non-conception menstrual cycle hormonal differences Table III. Testing for differences in oestrone-3-glucuronide (E1G) and pregnanediol-3-glucuronide (PdG) between 32 paired conception and nonconception cycles (non-conception cycles had sexual intercourse close to estimated day of ovulation so that poor timing of intercourse was unlikely to account for the failure to conceive) Summary variable Oestrone-3-glucuronide (E1G) Early follicular E1G Mid-follicular E1G Peak E1G Rate of E1G rise Early luteal E1G Mid-luteal E1G Pregnanediol-3-glucuronide Early follicular PdG Mid-follicular PdG Early luteal PdG rise Mid-luteal PdG Ratio (E1G/PdG) Ratio descent Mid-luteal ratio n Differencea (SE) P valueb 29 31 30 30 29 31 1.79 1.04 4.51 0.31 4.24 7.13 (1.33) (1.70) (3.99) (2.10) (2.51) (2.44) 0.27 0.37 0.36 0.58 0.39 ,0.01 29 31 31 31 0.05 0.01 0.21 0.60 (0.07) (0.02) (0.09) (0.32) 0.99 0.55 ,0.01 0.04 –11.58 (5.77) 0.72 (2.67) 0.08 0.72 32 31 aThe value for the non-conception cycle was subtracted from the value for the conception cycle. bP values were based on the Wilcoxon signed-rank procedure. conception cycles had higher mid-luteal E1G concentrations than the respective non-conception cycle, but the difference was not statistically significant in this small group of eight pairs. Discussion To characterize hormonal patterns predictive of conception, we excluded from our initial comparisons non-conception cycles that were likely to have failed due to poorly timed sexual intercourse. Conception cycles in the group of 32 women with well-timed intercourse in their non-conception cycles showed a significantly stronger early luteal rise in PdG and higher mid-luteal E1G and PdG concentrations compared with non-conception cycles from the same women. Conception cycles also tended to have a more rapid mid-cycle transition from follicular production of oestrogen to luteal production of progesterone (i.e. a more rapid luteinization reflected in a steeper descent of the E1G:PdG ratio), but this difference was not statistically significant. No differences were found in preovulatory concentrations of urinary oestrogen and progesterone metabolites. These differences cannot be explained by errors in our estimated day of ovulation. The E1G peak occurred on the day before our estimated day of ovulation in approximately half of both conception and non-conception cycles, and the remaining distribution of the number of days between the E1G peak and our estimated day of ovulation was nearly identical for conception and non-conception cycles. Nor can these differences be explained by changes over time, a concern because the non-conception cycle always preceded the conception cycle for each participant. When non-conception cycles from early in participation were compared with non-conception cycles late in participation for the 80 women in the North Carolina Early Pregnancy Study with such data, none of the observed differences between conception and non-conception cycles were seen. Figure 4. Daily geometric means of oestrone-3-glucuronide (E1G; top panel) and pregnanediol-3-glucuronide (PdG; lower panel) for paired conception (s) and non-conception (d) cycles from eight women whose non-conception cycle had poorly timed sexual intercourse. Data are centred on luteal day 0, the estimated day of ovulation (vertical dotted line). The SEs (shown by a single dotted line for each day) are based on within-woman differences between the two cycles, i.e. the difference between the corresponding daily values in the two cycles for each woman is calculated, these differences are averaged across women and the SE of the resultant mean difference is determined. The hormonal patterns associated with conception in our urine-based data are remarkably similar to those reported by Stewart et al. (1993) based on plasma oestrogen and progesterone measures. As in our study, the women in their study had no known fertility problems and were trying to conceive. Furthermore, the non-conception cycles were similarly selected for well-timed intercourse [Stewart et al. (1993) studied unsuccessful artificial insemination cycles during which inseminations were clinically timed to coincide with ovulation]. Our results differ somewhat from those reported by Lipson and Ellison (1996) for salivary oestrogen and progesterone concentrations in 17 conception cycles. They found no differences in progesterone concentrations, and higher oestrogen 2611 D.D.Baird et al. Table IV. Testing for differences in luteal oestrone-3-glucuronide (E1G) and pregnanediol-3-glucuronide (PdG) between eight paired conception and nonconception cycles (non-conception cycles had poorly timed sexual intercourse so that poor timing of intercourse might account for the failure to conceive) Summary variable Oestrone-3-glucuronide (E1G) Early luteal E1G Mid-luteal E1G Pregnanediol-3-glucuronide (PdG) Early luteal PdG rise Mid-luteal PdG Ratio (E1G/PdG) Ratio descent Mid-luteal ratio n Differencea (SE) P valueb 8 8 0.38 (2.17) 8.25 (6.76) 0.84 0.25 8 8 –0.08 (0.13) –0.14 (0.42) 0.95 0.84 8 8 3.52 (13.43) 0.51 (1.64) 0.64 0.74 aThe value for the non-conception cycle was subtracted from the value for the conception cycle. bP values were based on the Wilcoxon signed-rank procedure. throughout the conception cycle, especially at the time of midfollicular development. Stewart et al. (1993) argued that the higher hormone concentrations in conception cycles are probably a response of the ovary to a preimplantation embryonic signal, which they suggested could be early HCG secretion at concentrations too low to be detected in peripheral blood or urine. Preimplantation embryonic HCG production has been reported (Lopata and Hay, 1989), and tubal tissue expresses HCG receptors that could be responsive to early preimplantation signals (Lei et al., 1993). If the differences seen by Stewart et al. (1993) and also reported here were due to the influence of the conceptus, then we should see similarly higher hormone concentrations in conception cycles whether or not sexual intercourse was well timed in the paired non-conception cycles. Therefore we examined eight pairs with poorly timed intercourse in the nonconception cycle (chosen to optimize the number of hormonally adequate cycles among the non-conception cycles as these cycles may have failed just because of poorly timed intercourse). Among the eight cycles we found no evidence of higher luteal progesterone concentrations in the conception cycles. There was still a suggestion of higher mid-luteal oestrogen concentrations, though the difference was not statistically significant in this small sample. Our progesterone data are more consistent with the hypothesis that higher luteal progesterone concentrations in conception cycles reflect inherently better quality cycles that enhance the likelihood of conception, rather than the hypothesis that signals from the early embryo stimulate enhanced progesterone production by the ovary. The findings of more rapid luteinization and higher mid-luteal progesterone concentrations are consistent with the well-known need for luteal progesterone to prepare the oestrogen-primed endometrium for implantation (Li et al., 1991). Basal body temperature data also support an association between slow luteinization, reflected in a slow temperature rise, and subfertile cycles (Ishimaru et al., 1992). It may also be that the higher progesterone metabolite concentrations associated with conception in our data are not of direct importance for fertility, but rather are markers of a healthy 2612 egg (Jones, 1990) and well-functioning hormonal regulation. Lower progesterone concentrations in the luteal phase have been observed in women with unexplained infertility and may be secondary to temporary luteal cyst formation (Coutts, 1985; Hamilton et al., 1990) or failure of the follicle to rupture, despite an LH surge (Kugu et al., 1991). None of the women in our analysis was clinically infertile, but fertile women may also have occasional low-fertility cycles with impaired luteinization and a lower mid-luteal progesterone concentration. Higher mid-luteal oestrogen metabolite concentrations were strongly related to conception in the group of 32 women selected for well-timed intercourse in their non-conception cycles, and a fairly similar pattern was seen in the group of eight with poorly timed intercourse in the non-conception cycles. So the possibility that the preimplantation embryo can stimulate increased mid-luteal oestrogen production cannot be ruled out. The importance of luteal oestrogen for endometrial preparation and implantation in humans and other primates is controversial (Moudgal and Ravindranath, 1989; Moudgal, 1991; Ghosh et al., 1994; Yoshinaga, 1994; Younis et al., 1994; de Ziegler, 1995; Edgar, 1995; Ghosh and Sengupta, 1995), but may be critical in suppressing gonadotrophin concentrations and thus suppressing the development of the next cohort of follicles (Zeleznik et al., 1987; Nippoldt et al., 1989; de Ziegler et al., 1992). Whether this suppression is important for successful implantation and early development is unclear. In summary, we observed evidence of more rapid luteinization and higher luteal oestrogen and progesterone concentrations in conception cycles compared with non-conception cycles that were selected to include hormonally inadequate cycles (sexual intercourse was well timed but no pregnancy ensued). Higher fertility associated with rapid luteinization and high progesterone production is not surprising, but any benefit associated with elevated luteal oestrogen requires further investigations. Although we described an analysis designed to support or refute the importance of preimplantation embryonic signalling as a cause for higher luteal hormone concentrations in conception cycles, our sample size was insufficient to provide convincing evidence on either side. Preimplantation embryo signalling could not be ruled out. Acknowledgements Joy Pierce managed the field study of women attempting pregnancy and, assisted by Francis Patterson and Irene Gunter, managed urine storage and shipment. Robin Randall, Michelle Mason-Woodard and Robin King conducted laboratory assays. Drs Bill Lasley, James Kesner, Elizabeth Lenton, Sioban Harlow, Gary Hodgen, Ronald Gray, Beth Gladen and Walter Rogan reviewed an earlier draft of this manuscript. References Baird, D.D., Weinberg, C.R., Wilcox, A.J. et al. (1991) Using the ratio of urinary oestrogen and progesterone metabolites to estimate day of ovulation. Stat. Med., 10, 255–266. Baird, D.D., McConnaughey, D.R., Weinberg, C.R. et al. (1995) Application of a method for estimating day of ovulation using urinary estrogen and progesterone metabolites. Epidemiology, 6, 547–550. Conception versus non-conception menstrual cycle hormonal differences Baker, T.S., Jennison, K. and Kellie, A.E. (1980) A possible method for the detection of ovulation and the determination of the duration of the fertile period. J. Steroid Biochem., 12, 411–415. Branch, C.M., Collins, P.O., Kilpatrick, M.J. et al. (1980) The effect of conception on the concentration of urinary oestrone-3-glucuronide, LH/ hCG and pregnanediol-3α-glucuronide. Acta Endocrinol., 93, 228–233. Coutts, J.R.T. (1985) The abnormal luteal phase. In Jeffcoate, S.L. (ed.), The Luteal Phase, John Wiley, London, UK, pp. 101–114. de Ziegler, D. (1995) Hormonal control of endometrial receptivity. Hum. Reprod., 10, 4–7. de Ziegler, D., Bergeron, C., Cornel, C. et al. (1992) Effects of luteal estradiol on the secretory transformation of human endometrium and plasma gonadotropins. J. Clin. Endocrinol. Metab., 74, 322–331. Diaz, S., Cardenas, H., Brandeis, A. et al. (1992) Relative contributions of anovulation and luteal phase defect to the reduced pregnancy rate of breastfeeding women. Fertil. Steril., 58, 498–503. Edgar, D.H. (1995) Oestrogen and human implantation. Hum. Reprod., 10, 2–4. Eren, S., Reynolds, G.H., Turner, M.E. et al. (1967) Estrogen metabolism in the human II. J. Clin. Endocrinol., 27, 819–827. Ghosh, D. and Sengupta, J. (1995) Endometrial receptivity for implantation: another look at the issue of peri-implantation oestrogen. Hum. Reprod., 10, 1–2. Ghosh, D., De, P. and Sengupta, J. (1994) Luteal phase ovarian oestrogen is not essential for implantation and maintenance of pregnancy from surrogate embryo transfer in the rhesus monkey. Hum. Reprod., 9, 629–637. Hamilton, M.P.R., Fleming, R., Coutts, J.R.T. et al. (1990) Luteal cysts and unexplained infertility: biochemical and ultrasonic evaluation. Fertil. Steril., 54, 32–37. Hollander, M. and Wolfe, D.A. (1973) Nonparametric Statistical Methods. John Wiley, New York, NY, USA. Irianni, F.M., Veeck, L.L., Toner, J.P. et al. (1992) Influence of number of pre-embryos transferred, progesterone level and oestradiol/progesterone ratio at thaw on pregnancy results during placement of cryopreserved preembryos in natural cycles. Hum. Reprod., 7, 797–800. Ishimaru, T., Mahmud, N., Kawano, M. et al. (1992) Sporadic appearance of luteal-phase defect in prospective assessment. Horm. Res., 37 (Suppl. 1), 32–36. Jones, G.S. (1990) Corpus luteum: composition and function. Fertil. Steril., 54, 21–26. Kugu, K., Taketani, Y., Kohda, K. and Mizuno, M. (1991) Exaggerated prolactin response to thyrotropin-releasing hormone in infertile women with the luteinized unruptured follicle syndrome. Arch. Gynecol. Obstet., 249, 27–31. Lei, Z.M., Toth, P., Rao, Ch.V. et al. (1993) Novel coexpression of human chorionic gonadotropin (hCG)/human luteinizing hormone receptors and their ligand hCG in human Fallopian tubes. J. Clin. Endocrinol. Metab., 77, 863–872. Lenton, E.A., Sulaiman, R., Sobowale, O. et al. (1982) The human menstrual cycle: plasma concentrations of prolactin, LH, FSH, oestradiol and progesterone in conceiving and non-conceiving women. J. Reprod. Fertil., 65, 131–139. Lenton, E.A., de Kretser, D.M., Woodward, A.J. et al. (1991) Inhibin concentrations throughout the menstrual cycles of normal, infertile, and older women compared with those during spontaneous conception cycles. J. Clin. Endocrinol. Metab., 73, 1180–1190. Li, T.C., Warren, M.A., Dockery, P. et al. (1991) Human endometrial morphology around the time of implantation in natural and artificial cycles. J. Reprod. Fertil., 92, 543–554. Lipson, S.F. and Ellison, P.T. (1996) Comparison of salivary steroid profiles in naturally occurring conception and non-conception cycles. Hum. Reprod., 11, 2090–2096. Lopata, A. and Hay, D.L. (1989) The surplus human embryo: its potential for growth, blastulation, hatching, and human chorionic gonadotropin production in culture. Fertil. Steril., 51, 984–991. Moudgal, N.R. (1991) On the requirement for estrogen for establishing pregnancy in the non-human primate. In Strauss, J.F., III and Lyttle, C.R. (eds.), Uterine and Embryonic Factors in Early Pregnancy. Plenum Press, New York, NY, USA, pp. 13–19. Moudgal, N.R. and Ravindranath, N. (1989) Requirement for estrogen in implantation and post implantation survival of blastocyst in the bonnet monkey. In Yoshinaga, K. and Mori, T. (eds.), Development of Preimplantation Embryos and their Environment. Alan R.Liss, New York, NY, USA, pp. 277–288. Nippoldt, T.B., Reame, N.E., Kelch, R.P. et al. (1989) The roles of estradiol and progesterone in decreasing luteinizing hormone pulse frequency in the luteal phase of the menstrual cycle. J. Clin. Endocrinol. Metab., 69, 67–76. Royston, J.P. (1983) Statistical approaches to the prediction and detection of ovulation: detecting the signal among the noise. In Jeffcoate, S.L. (ed.), Ovulation: Methods for its Prediction and Detection. John Wiley, New York, NY, USA, pp. 19–32. Samarajeewa, P., Cooley, G. and Kellie, A.E. (1979) The radioimmunoassay of pregnanediol-3α-glucuronide. J. Steroid Biochem., 11, 1165–1171. Stewart, D.R., Overstreet, J.W., Nakajima, S.T. et al. (1993) Enhanced ovarian steroid secretion before implantation in early human pregnancy. J. Clin. Endocrinol. Metab., 76, 1470–1476. Weinberg, C.R., Gladen, B.C. and Wilcox, A.J. (1994) Models relating the timing of intercourse to the probability of conception and the sex of the baby. Biometrics, 50, 358–367. Wilcox, A.J., Weinberg, C.R., O’Connor, J.F. et al. (1988) Incidence of early loss of pregnancy. N. Engl. J. Med., 319, 189–194. Wilcox, A.J., Weinberg, C.R. and Baird, D.D. (1995) Timing of sexual intercourse in relation to ovulation: effects on the probability of conception, survival of the pregnancy, and sex of the baby. N. Engl. J. Med., 333, 1517–1521. Wright, K., Collins, D.C., Musey, P.I. et al. (1978) Direct radioimmunoassay of specific urinary estrogen glucosiduronates in normal men and nonpregnant women. Steroids, 31, 407–426. Yoshinaga, K. (1994) Endocrinology of implantation. In Tulchinsky, D. and Little, A.B. (eds.), Maternal–Fetal Endocrinology. W.B. Saunders, Philadelphia, PA, USA, pp. 336–349. Younis, J.S., Ezra, Y., Sherman, Y. et al. (1994) The effect of estradiol depletion during the luteal phase on endometrial development. Fertil. Steril., 62, 103–107. Zeleznik, A.J., Hutchison, J.S. and Schuler, H.M. (1987) Passive immunization with anti-oestradiol antibodies during the luteal phase of the menstrual cycle potentiates the perimenstrual rise in serum gonadotrophin concentrations and stimulates follicular growth in the cynomolgus monkey (Macaca fascicularis). J. Reprod. Fertil., 80, 403–410. Received on August 11, 1997; accepted on September 24, 1997 2613