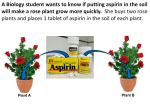
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
CLINICAL CHEMISTRY, Vol. 19, No. 4, (1973) 361-365 ToxicologicalFindingsin Fatal Poisonings ArthurJ. McBay Anyone who must decide whether the amount of toxic substance present in a specimen is sufficient to indicate that the substance may have been the cause of death is aware of the difficulty of finding information to guide that decision. Opinions are given concerning therapeutic and toxic concentrations in human tissues for most of the common drug and chemical poisons. These include alcohols, amitriptyline, amphetamine, arsenic, barbiturates, boron, bromides, carbon monoxide, chloral hydrate, chlordiazepoxide, cyanide, diazepam, diphenylhydantoin, ethchlorvynol, fluoride, glutethimide, heroin (morphine), imipramine, lead, LSD, marihuana, meperidine, meprobamate, methadone, methamphetamine, methaqualone, nicotine, nortriptyline, orphenadrine, paraldehyde, pentazoci ne, phenothiazines, propoxyphene, quinine, salicylates, and strychnine. Interpretation of the results of toxicological examinations is not easy. The reference material on which such decisions must be founded is not always readily accessible. The opinions and case studies must be treated as such, because there are many problems connected with obtaining an adequate and thorough investigation of even fatal poisonings. Some of these problems include: insufficient history of the individual; presence of multiple toxic agents; inadequate or improperly obtained and preserved samples; samples obtained from an embalmed body; no autopsy; autopsy performed but a “general unknown” determination requested when signs and symptoms could lead to a more narrowly directed search; the finding of a small amount of some agent and attributing death to this because no other cause of death could be found (cause of death may not be established in some cases even after exhaustive investigation, e.g., “crib deaths”). With fatalities it cannot be too strongly emphasized that an autopsy is not only desired but essential if death by poisoning is to be established. It may be that the amount of alcohol or the amount of carbon monoxide present is all that is desired to determine if either of these had affected the individual. In the absence of an autopsy or an enlightening medical history, it is difficult to determine how the amount of a specific drug in a person might be interpreted. From the Office of the Chief Medical Examiner, North Carolina State Board of Health; and the School of Pharmacy and the Department of Pathology, School of Medicine, University of North Carolina, Chapel Hill, N. C. 27514. Received Oct. 25, 1972; accepted Jan. 16, 1973. With all toxic agents, individual variances will have a profound effect on the interpretation of drug concentrations. Many drugs cause irreversible damage when their concentration in the blood is high but, because the person does not die immediately, the concentration at the time of death may be much lower. Death may result when two or more drugs are each present in sublethal amounts. The types of analyses that may be performed and the specimens that are desired for analysis vary from laboratory to laboratory, depending upon the expertise of the analysts, the availability of equipment, and the workload of the laboratory. Drugs that may be determined when present in lethal amounts may be infinitely more difficult or impossible to find in therapeutic amounts. Liver tissue and large volumes of blood may be obtained from the dead whereas in the living only urine or a small amount of blood may be available. An earlier paper dealt with chemical findings in poisonings (1). The present paper gives the latest information available, which usually has been obtained by virtue of advances in methodology. The opinions I offer are based on present information. As more information becomes available, it is certain that some of the opinions will have to be changed. Ethanol (Ethyl Alcohol) Impairment from ethanol may be detected by special measurements when the concentration is as low as 500 mg/liter of blood. Everyone’s judgment is impaired by the time the concentration reaches 1 g/ liter (0.10%). Intoxication occurs at about 2 g/liter. Stupor occurs at about 3 g/liter, and coma and death at concentrations greater than 4 to 5 g/liter. The blood ethanol concentration must be about 5 g/liter to be considered the cause of death, but an individual may not die until the concentration is as low as 2 g/liter if it takes 10 to 12 hours to succumb. Although the concentration of alcohol in the blood will not change materially after death, in the living it will decrease by about 100 to 200 mg/liter per hour. Lower concentrations of alcohol may be very significant when sublethal amounts of other drugs are present also. The fatal dose of ethanol is between 500 and 1000 ml of 100-proof liquor (50% ethanol), ingested in an hour or two. Although the figure varies with individual tolerance, weight, and experience, it generally takes at least 180 ml of 100-proof CLINICAL CHEMISTRY, Vol. 19, No. 4, 1973 361 liquor ingested in a short period to produce an ethanol concentration of 1 g/liter. Most people appear to be drunk at levels of 1.5 to 2.5 g/liter, a level attained by rapidly ingesting about 250 to 450 ml of 100-proof liquor. An excellent reference on alcohol is available (2). Methanol (Methyl Alcohol) In cases of fatal poisonings, concentrations of methanol in blood generally exceed 1 g/liter (3). The toxic dose of methanol varies greatly because it depends on the amount of ethanol in the body that may have to be preferentially metabolized instead of methyl alcohol. Ethanol serves as an antidote for methanol. Methanol may be found in the blood for several days after poisoning. When methanol is detected, a test for formaldehyde should be made. If formaldehyde is found, contamination with embalming fluid or tissue fixative should be suspected. Formaldehyde solutions usually contain 10 to 15 ml of methanol per 100 ml, as a preservative. Isopropanol (Isopropyl Alcohol) Isopropyl alcohol, which is present in many sampies of rubbing alcohol, may be intentionally or accidentally ingested. When isopropanol is found in blood, its metabolite, acetone, should be present also. Concentrations of 1 g/liter of blood or more have been found in fatal poisonings (4). The fatal dose is about 250 ml. Isopropanol is occasionally present in embalming fluid. Paraldehyde Findings of 500 mg of paraldehyde per liter of blood indicate fatal poisoning (5). Lower concentrations are hazardous when ethanol is present. Paraldehyde, which decomposes to acetic acid, may produce serious metabolic acidosis. Doses of about 30 ml or less have been the evident cause of fatalities. Intramuscular injection of 10 ml of the drug produced a concentration as high as 77 mg/liter of plasma, and therapeutic doses gave concentrations ranging from 34 to 150 mg/liter of blood (5). Carbon Monoxide Everyone has a small amount of carbon monoxide his blood. This is usually less than 5% of the saturation concentration. Heavy smokers and those in certain occupations may reach about 10% saturation. The effects of continuous exposure to these low concentrations is not known. Healthy individuals should survive blood saturations of 40% for a minute or of 20% for a week. Those with circulatory or respiratory diseases could die from such exposures. Those fatally exposed to the fumes of an internal combustion engine usually have blood saturations of 60% or more. It is possible to be found dead as a result of a fire and not have significantly increased concentrations of carbon monoxide in the blood. A person may have a high level of carbon monoxide and not appear in 362 CLINICAL CHEMISTRY, Vol. 19, No. 4, 1973 “pink.” The blood in a dead body neither absorbs nor loses carbon monoxide. Barbiturates Oral doses of 600 mg of barbiturates produced the following average maximum (per liter) concentrations in the blood: pentobarbital, 3.3 mg; secobarbital, 4.8 mg; amobarbital, 9.6 mg; butabarbital, 14 mg; and phenobarbital, 23 mg (6). To determine the significance of the concentration of a barbiturate it is necessary to know whether the barbiturate is slow-acting or rapid-acting and whether the person is tolerant or not. In a study (7) of deaths attributed to the barbiturates, most samples had the following ranges of barbiturate concentration: Bar biturates alone mg/liter Secobarbital Pentobarbital Amobarbital Butabarbital Phenobarbital of blood 15-24 15-44 10-24 10-24 30-54 10-29 15-19 10-54 15-29 30-39 105-134 20-44 Amo- and Secobarbital Barbiturate plus ethanol When the blood contained more than 1 g of ethanol per liter, as little as 5 mg of barbiturates per liter of blood was considered sufficient to be the cause of death. About 12 100-mg doses of a rapid-acting barbiturate may be sufficient to cause death. But only 600 mg may cause death when the blood contains about 1.5 g of alcohol per liter. Glutethimide (‘Doriden,” Ciba) A single therapeutic oral dose of 1 g of glutethimide has produced a blood concentration of about 7 mg/liter. Serious intoxication will follow the absorption of 10 g or more of the drug. Deaths have been attributed to concentrations of 30 mg/liter of blood. If a patient survives for several days after a toxic dose, the concentration in blood will decline so that a postmortem concentration of 10 mg/liter, which is in the therapeutic range, may indicate poisoning (8). Ethchlorvynol (“Placidyl ,“ Abbott) Oral ingestion of 200 mg of ethchlorvynol produces blood concentrations less than 2 mg/liter and urinary concentrations less than 1 mg/liter (5). Concentrations greater than 20 mg/liter of blood or 20 mg/kg of liver have been considered sufficient for the drug to be considered the cause of death. Meprobamate Oral doses of 400 and 1200 mg of meprobamate produced blood concentrations of 5 and 15 mg/liter (9). Fatal concentrations in the blood are usually greater than 50 mg/liter and in the liver greater than 100 mg/kg (5). Chloral Hydrate After oral ingestion of 1 g of chloral hydrate, its concentration in blood reached a maximum of 1.5 mg of trichlorethanol per liter; no chloral hydrate was detected (10). The amounts of chloral hydrate usually reported in poisonings are greater than 10 mg of chloral hydrate per liter of blood. blood concentration of about 50 to 100 mg per liter. Arthritic patients taking 10 to 12 g every 24 hours have concentrations as high as 400 mg/liter of blood. Concentrations greater than 250 mg/liter indicate intoxication. Death may occur many hours after concentrations as high as 1 g/liter in the blood have produced their damage; the level at the time of death may be much lower (16). Phenothiazines Hospitalized patients who survived treatment for overdosages of phenothiazines had concentrations of 1 to 2 mg of chlorpromazine, trifluoperazine, promazine, or prochlorperazine, and 2 to 5 mg of thioridazme per liter of serum (11). Deaths have been attributed to phenothiazines in cases where concentrations in blood were less than 5 mg/liter when the liver contained at least 50 mg of the drug per kilogram wet weight. Sudden deaths after the administration of therapeutic amounts of phenothiazines, particularly thioridazine, have been reported (12). It is expected that the concentrations of drug in the blood and liver would be lower than those stated above for poisonings. Diphenylhydantoin (“Dilantin,” Parke, Davis) Therapeutic doses of 600 mg of diphenylhydantoin produce maximum concentration in blood of 10 mg/ liter (6). Concentrations greater than 70 mg/liter or 100 mg/kg of liver have been found in fatal poisonings. Orphenadrine Blood containing at least 4 mg of orphenadrine per liter and liver containing more than 20 mg/kg were considered sufficient evidence that the drug caused death (13). Chlordiazepoxide (“Librium,” Roche) Chlordiazepoxide is a rather safe drug. The documented cases in which this drug has been blamed for deaths appear to be those where it has been present with another drug that it might potentiate. Cases have been reported in which up to 1 g was ingested without producing coma (14). Oral doses of 150 mg/ day produce concentrations in plasma of less than 10 mg/liter; 400 to 600 mg per day produces concentrations up to 40 mg/liter. Concentrations as high as 40 mg/liter do not result in deep coma. Diazepam (“Valium,” Roche) This benzodiazepine, like chlordiazepoxide, has a very low toxicity. The blood concentrations of diazepam are very low. Oral doses of 10 mg may produce concentrations in blood of about 0.2 mg/liter, and when 150 to 200 mg is taken the level may reach 2 mg/liter (15). Salicylates (Acetylsalicylic Methyl Salicylate) A therapeutic Acid, dose of 1 g of aspirin will produce a Morphine-Heroin-Quinine Heroin is converted to morphine in the body. Most methods of determining heroin hydrolyze the drug to morphine. Since much of the material sold as heroin contains relatively large amounts of quinine, finding small amounts of quinine in biological specimens suggests the abuse of heroin. One hour after intravenous injection of a single 10-mg intravenous dose of morphine by adults, serum morphine concentration is about 0.1 mg/liter, decreasing to less than 10 zg/ liter in about four to eight hours (17). The urine of heroin addicts contains an average of 22 mg of total morphine per liter (18). In fatal poisonings, morphine concentrations of 20 to 200 zg/liter have been found (19). Liver should contain 0.1 to 1.0 mg of total morphine per kilogram. Morphine persists in much greater concentrations for 24 or more hours in urine or bile, so these specimens may serve as useful screening samples. It is thought that morphine should be demonstrated in blood to certify sudden death because of “intravenous narcotism.” In fatal quinine intoxication relatively large amounts are found. The blood may contain more than 10 mg of quinine per liter, the liver more than 50 mg/kg. Deaths have been related to heroin when no evidence of quinine was found in the body. Methadone Robinson reported a series of 11 deaths related to methadone, in the significant cases the concentrations were 0.2 to 3 mg per liter of blood and 2 to 50 mg per kg of liver (20). Propoxyphene (“Darvon,” Lilly) Drug concentrations reached a maximum of 0.2 mg/liter of plasma in 1 h after a 195-mg oral dose and 0.3 mg/liter in 30 mm after a 50-mg intravenous dose (21). The concentration in plasma reached a maximum of 0.3 mg/liter after administration of 13 oral doses of 65 mg of the propoxyphene hydrochloride or 100 mg of the newer propoxyphene napsylate (22). In fatal poisonings, concentrations of at least 2 mg/liter of blood and 30 mg/kg of liver are attained. Pentazocine (“Talwiri,” Winthrop) Therapeutic oral, intravenous, and intramuscular doses produce conc?ntrations of about 150 g of pentazocine per liter of blood (23). In a death attributed to pentazocine, 5 mg/liter was found in the blood and 45 mg/kg was found in hydrolyzed liver. CLINICAL CHEMISTRY, Vol. 19, No. 4, 1973 363 Meperidine (“Demerol,” Winthrop) Intramuscular injections of 100 mg of meperidine produced concentrations of 1 mg/liter of serum (24). Blood containing 10 mg/liter and liver containing 10 mg/kg have been considered sufficient evidence of cause of death. Amphetamine and Methamphetamine No amphetamine was found in the plasma of a subject taking 30 mg of dextroamphetamine daily (25). Concentrations of amphetamine reported in cases of fatal poisoning are (per liter or kilogram): 0.5 mg for blood, 4 mg for urine, and 0.3 mg for liver. For methamphetamine the corresponding figures are, respectively: 0.6, 0.1, and 0.7 mg. These concentrations were attained after intravenous administration. Concentrations of 40 mg/liter in blood and greater than that in organs were associated with a fatal oral ingestion (26). Methaqualone In human subjects, this drug attained a concentration of 2 mg per liter of plasma in 30 minutes after a single 250-mg oral dose (27). In fatal poisonings the blood concentration usually exceeds 5 mg per liter, the concentration in liver 40 mg per kilogram. Amitriptyline and Nortriptyline after chronic poisoning. Urine containing more than 1 mg of arsenic per liter is indicative of poisoning. Concentrations above 5 mg/kg in the liver are significant. Analysis of fingernails is unhelpful in the living-the distal portions will not contain arsenic unless it had been given many months previously. Hair rarely constitutes a good sample in the living because such a large quantity of the entire length of hair is required. Lead Urines from normal individuals contain 0 to 0.1 mg of lead per liter (median, about 0.03). Normal blood specimens contain 0 to 1 mg of lead per liter [median, about 0.2 (33)]. Urine containing more than 0.1 mg of lead per liter or more than 10 mg of oaminolevulinic acid per liter indicates exposure to lead (34). Concentrations of more than 2 mg of lead per liter of blood and concentrations over 10 mg of lead per kg of liver have been found in fatal poisonings. Normal livers have less than 5 mg of lead per kg. Cyanide Detectable amounts of cyanide in blood indicate poisoning. Concentrations of about 10 mg/liter of blood are found in poisoning (35). Fluorine Adults receiving 25 to 75 mg of nortriptyline orally three times a day for four to seven days had drug concentrations of 30 to 160 gig/liter of plasma (28). In autopsy cases involving these drugs the concentrations in the blood were between 0 and 11 mg of amitriptyline, and between 8 and 26 mg of nortriptyline per liter. The liver contained more than 50 mg of drug per kilogram (29). Normal blood contains 0.01 to 0.1 mg of fluorine per liter. Concentrations greater than 3 mg of fluorine per liter of blood have been found in poisonings (36). The liver appears to have about half as high a concentration as the blood. Normal urines have mean concentrations of the order of 0.3 to 0.4 mg per liter. Imipramine Boron-Boric (“Tofranil,” Geigy) Acid-Borates Patients receiving 150 to 300 mg per day had drug concentrations 0.1 to 0.6 mg per liter (30). In fatal cases the blood contained at least 2 mg/liter, the liver 10 mg/kg (31). Blood boron “normals” are in the range of 0 to 0.8 mg per liter. More than 40 mg of boron per liter of blood suggests boron poisoning. Nicotine Blood concentrations of 1 g of bromide per liter are significant. The normal bromide concentration in human blood is reportedly 1.5 to 50 mg bromine per liter (37). Smoker’s blood should contain less than 0.3 mg of nicotine per liter. Concentrations greater than 5 mg/liter are found in blood and 10 mg/kg in liver in cases of fatal poisoning (32). Strychnine Any strychnine found is significant, because it is now rarely used medicinally. The blood will usually contain more than 2 mg/liter, the liver more than 4 mg/kg in poisonings (32). Arsenic Urine is the best specimen from the living for quantitating this poison because abnormally high amounts of arsenic persist in the urine for about a week after acute poisoning and up to about a month 364 CLINICAL CHEMISTRY. Vol. 19, No.4, 1973 Bromides Marihuana (Cannabis) Cannabinoids in plasma averaged 70 ag/liter after the subjects smoked two marihuana cigarettes containing either 11 or 22 mg of tetrahydrocannabinol (38). Cannabinols may be detected in the saliva and urine of smokers, and on their hands. Methods for measuring marihuana (and LSD) are very new and are not routinely available. LSD (Lysergic acid diethylamide) A radioimmunoassay tion of LSD in urine method for the determinahas been presented. Human subjects who received 0.2 mg and 0.3 mg oral doses had concentrations between 5 and 50 izg/liter in urine (39). The most significant findings in drowning deaths are the discovery of sand, mud, plants and other material in the airways and lungs. Differences between the blood of the right and left heart, such as in the amounts of chlorides and in the specific gravities, are not usually significant in fresh-water drownings, and only occasionally significant in salt-water drownings. Many times these findings are the reverse of what is expected. The finding of diatoms after the wet digestion of tissue may be of significance (40). References 1. McBay, A. J., Chemical findings Med. 274, 1257 (1966). 2. Alcohol and the Impaired Driver, Association, 1970. 3. Stratton, F., Determination in poisonings. Chicago, of methanol New American in body Engl. J. Medical fluids. Amer. alcohol (Rub- J. Clin. Pat hot. 25, 1071 (1955). 4. Adelson, L., Fatal bing alcohol). AmerJ. intoxication with isopropyl Clin. Pathol. 38, 144 (1962). 5. Maes, R., Hodnett, N., Landesman, H., et al., The gas chromatographic determination of selected sedatives (ethchlorvynol, paraldehyde, meprobamate, carisoprodol) in biological material. J. Forensic Sci. 14, 235 (1969). 6. Parker, K. D., Elliott, H. W., Wright, J. A., et al., Blood and urine concentrations of subjects receiving barbiturates, meprobamate, glutethimide or diphenylhydantoin. Clin Toxicot. 3, 131 (1970). G., McGarry, E., and Daigle, J., Toxicological for fatalities due to carbon monoxide J. Forensic Sci. 17, 640 (1972). and barbiturates data in Ontario. 8. Algeri, E. J., and Katsas, G. G., Toxicology of glutethimide. J. Sci. 5, 217 (1960). 9. Finkle, B., The identification, quantitative determination, and distribution of meprobamate, glutethimide in biological material. J. Forensic Sci. 12, 509(1967). 10. Kaplan, H. L., Forney, R. B., Hughes, F. W., and Jam, N. C., Chloral hydrate and alcohol metabolism in human subjects. J. Forensic Sci. 12, 295 (1967). 11. Tompsett, S. L., The spectrofluorimetric determination of phenothiazine drugs in blood serum. Acta Pharmacol. Toxicol. 26, 298(1968). 12. Leestma, J. E., and Koenig, K. L., Sudden deaths and phenothiazines. Arch. Gen. Psychiat. 18, 137 (1968). 13. Clarke, E. G. C., Isolation and Identification of Drugs, The Pharmaceutical Press, London, 1969, p436. 14. Gjerris, F., Poisoning with chlordiazepoxide. Dan. Med. Bull. 13, 170(1966). 15. DeSilva, J. A., Koechlin, B. H., and Boden, G., Blood level distribution patterns of diazepam and its major metabolite in man.J. Pharm. Sci. 55, 692(1966). 16. Done, A. K., Salicylate intoxication. Pediatrics 26,800(1960). Forensic 17. Spector, man. Science 19. McBay, A. J., and Turk, R. F., Heroin Deaths. Bull. mt. Ass. Toxicol., June 1972, p 12. 20. Robinson, A. E., and Williams, F. M., The distribution of methadone in man. J. Pharm. Pharmacol. 23, 353 (1971). 21. Wolen, R. L., Gruber, C. M., Kiplinger, G. F., and Scholz, N. E., Concentration of propoxyphene in human plasma following oral, intramuscular, and intravenous administration. Toxicol. Appl. Pharmacol. 19, 480 (1971). Forensic Drownings 7. Cimbura, 18. Payte, J. T., Wallace, J. E., and Blum, K., Acid hydrolysis: A requisite for morphine detection in urine. Reported to the Committee on Problems of Drug Dependence, February 1971. S., and Vesell, 174, 421 (1971). E. S., Disposition of morphine in 22. Wolen, R. L., Gruber, C. M., Kiplinger, G. F., and Scholz, N. E., Concentration of propoxyphene in human plasma following repeated oral doses. Toxicol. Appi. Pharrnacol. 19, 493 (1971). 23. Berkowitz, B. A., Asling, J. H., Schnider, S. M., and Leong Way, E., Relationship of pentazocine plasma levels to pharmacological activity in man. Clin. Pharmacol. Ther. 10, 320(1969). 24. Fochtman, F. W., and Winek, C. L., Therapeutic serum concentrations of meperidine. J. Forensic Sci. 14, 213 (1969). 25. Beckett, A. H., and Rowland, M., Urinary excretion kinetics of amphetamine in man. J. Pharm. Pharmacol. 17, 628(1965). 26. Cravey, R. H., and Reed, D., Intravenous amphetamine poisoning report of three cases. ,J. Forensic Sci. Soc. 10, 109 (1970). 27. Berry, D. J., Gas chromatographic determination of methaqualone at therapeutic levels in human plasma. J. Chromatogr. 42,39 (1969). 28. Asberg, It., Cronholm, B., Syoqvist, F. and Tuck, D., Relationship between plasma level and therapeutic effect of nortriptyline. Brit. Med. J. 3, 331 (1971). 29. Bonnichsen, B., Maehly, A. C., autopsy cases involving amitriptyline Med. 67, 190(1970). 30. Curry, and Skold, G., A report on and nortriptyline. J. Legal A. S., Seven fatal cases involving 16, 265 (1964). imipramine in man. J. Pharm. Pharmacol. 31. Fatteh, A., Blanke, 32. Registry Amer. Acad. R., and Mann, G. T., Death from imipra- J. Forensic Sci. 13, 124 (1968). mine poisoning. of Human Toxicology Reports, Forensic Sci., 1968-70 inclusive. Toxicology Section, 33. Goldwater, L. J., and Hoover, A. W., An international study of “normal” levels of lead in blood and urine. Arch. Environ. Health 15, 60(1967). 34. Blanksma, L. A., Sachs, H. K., Murray, E. F., and O’Connell, M. J., Failure of the urinary delta-aminolevulinic acid test to detect pediatric lead poisoning. Amer. J. Clin. Pathol. 53, 956 (1970). 35. Curry, A. S., Poison Detection in Human Organs. 2nd ed., Charles C Thomas, Springfield, 111., 1969, p 48. 36. Gettler, A. 0., and Ellerbrook, L., Toxicology of fluorides. Amer. J. Med. Sci. 197, 625 (1939). 37. Stewart, C. P., and Stolman, A., Toxicology, H, Academic Press, New York, N. Y., 1961, p 797. 38. Dott, A. B., Effect of marihuana ulated passing task. DHEW Pubi. 10. on risk acceptance in a simNo. (HSM) 72-10010, 1972, p 39. Taunton-Rigby, A., Sher, S. E., and Kelley, P. R., Radioimmunoassay for L.S.D. and its detection in human biological fluids. Presented at 6th. Int. Mtg. of Forensic Sciences, Edinburgh, 1972. 40. Neidhart, D. A., and Greendyke, R. M., The significance of diatom demonstration in the diagnosis of death by drowning. Amer. J. Clin. Pat hot. 48, 377 (1967). CLINICAL CHEMISTRY, Vol. 19, No. 4, 1973 365