Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
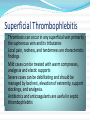
Thrombophlebitis Formation of a venous clot depends on the presence of of at least of one of Virchow’s triad factors -venous stasis -injury to vessel wall -hypercoagulable state SIGNS AND SYMPTOMS pain in the part of the body affected skin redness or inflammation (not always present) swelling (edema) of the extremities (ankle and foot). CAUSES Thrombophlebitis is related to a thrombus in the vein. Risk factors include prolonged sitting and disorders related to blood clotting Specific disorders associated with thrombophlebitis include superficial thrombophlebitis (affects veins near the skin surface) and deep venous thrombosis (affects deeper, larger veins) Clinical risk factors for deep vein thrombosis Trauma, travel Obesity, obstetrics Hypercoagulable, Surgery, smoking hormone replacement Recreational drugs(IV drugs) Old (age >60y) Malignancy Immobilization Birth control, blood group A Sickness Pathophysiology Most common cause of hereditary hemophilia is factor V Leiden Thrombi usually form at the venous cusps of deep veins where altered or static blood flow causes clot formation Alternatively, clots form from intimal defects Clots are composed from fibrin, red cells and platelets and cause partial/complete obstruction of vein Pathophysiology Postphlebitic syndrome (PPS) may develop after the resolution of a DVT PPS is due valvular incompetence, persistent outflow obstruction and abnormal microcirculation. Superficial Thrombophlebitis Thrombosis can occur in any superficial vein primarily the saphenous vein and its tributaries Local pain, redness, and tenderness are characteristic findings. Mild cases can be treated with warm compresses, analgesia and elastic supports Severe cases can be debilitating and should be managed by bed rest, elevation of extremity, support stockings, and analgesia. Antibiotics and anticoagulants are useful in septic thrombophlebitis Deep Vein Thrombosis Clinical exam is unreliable for detection or exclusion of a DVT Pain, redness, swelling, and warmth are present in less than half the patients with confirmed DVT. Pain in calf with dorsiflexion of ankle with the leg straight (Homan’s sign) is unreliable Deep Vein Thrombosis the leg is white due to arterial spasm secondary to massive iliofemoral thrombosis, often mistaken for arterial occlusion. PPS can be difficult to differentiate from recurrent DVT due to pain, swelling and ulceration of the skin. Up to to one third of the patients with DVT can develop PPS. Deep Vein Thrombosis-Diagnosis All patients with any signs or symptoms suggestive DVT should undergo an objective diagnostic evaluation Venography was the historical “gold standard” for detection of DVT with 100% sensitivity and specificity but it is invasive and can cause contrast-related reactions, phlebitis and DVT . Axillary and Subclavian Vein thrombosis 2-4% of DVTs occur in axillary or subclavian vein Risks include recent central venous catheters or pacemakers, IV drug use, malignancy, hypercoagulable states and excessive or unusual exercise, chronic compression(cervical rib, scalene or web) Treatment includes anticoagulation alone or preceded by thrombolysis. Pelvic Vein Thrombosis Usually it’s an extension of a clot from the femoral vein. An isolated pelvic vein thrombosis is rare and can be a complication in the postpartum period, after pelvic surgery or trauma. Septic pelvic vein thrombophlebitis is a lifethreatening condition after post-partum endometritis and is usually diagnosed with CT or MRI. COMPLICATIONS The most serious complication occurs when the blood clot dislodges, traveling through the heart and occluding the dense capillarynetwork of the lungs; this is a pulmonary embolism which can be potentially life threatening Treatment Bed rest, leg elevation and elastic stockings are of unproven benefit in the management of DVT. Aggressive anticoagulation will prevent extension of the clot. Early ambulation after adequate anticoagulation is a safe approach Primary objective of treating DVT is the prevention of pulmonary embolus Treatment Medications analgesics (pain medications) anticoagulants e.g warfarin or heparin to prevent new clot formation thrombolytics to dissolve an existing clot such as intravenous streptokinase. nonsteroidal anti-inflammatory medications (NSAIDS) such as ibuprofen to reduce pain and inflammation antibiotics (if infection is present) selection will usually depend with the causative agent. Support stockings and wraps to reduce discomfort Treatment In pregnant pt who cannot have heparin, danaproid should be used. Warfarin is contraindicated in pregnancy, active bleeding, recent major surgery (thoracoabdominal, nervous system, spine, eye) The patient may be advised to do the following Elevate the affected area to reduce swelling. Keep pressure off of the area to reduce pain and decrease the risk of further damage. Apply moist heat to reduce inflammation and pain. Surgical removal, stripping, or bypass of the vein is rarely needed but may be recommended in some situations. NAME : JAFER ALI GROUP: 317