Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
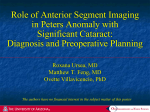
COVER STORY ONLINE SURVEY How Valuable Is Anterior Segment Imaging? Imaging devices are useful for further screening after first-line diagnostic assessment. BY SHAN LIN, MD T he primary value of anterior segment imaging in glaucoma care is for the detection and quantification of angle closure. Angle-closure glaucoma (ACG) is a major cause of blindness worldwide.1 It should be distinguished from open-angle glaucoma, because the treatment algorithms for each disease differ significantly, with potentially devastating results for patients in whom angle closure is not identified. The prevalence of ACG is especially high among Asians1: in China, ACG is the leading cause of bilateral blindness.2 That said, although ACG and the anatomic risk factors for this disease are most often identified in Asians,3-7 the prevalence of this disease is not insignificant in whites.8 Even as the role of anterior segment imaging in glaucoma care grows, many glaucoma specialists are questioning if it is imperative to have such a device in the office, especially if gonioscopy is the gold standard for assessing closed angles. GONIOSCOPY Gonioscopy has many advantages, including rapidity of use, low to no expense, the ability to distinguish synechial from appositional closure, a 360º view, and a direct view of the angle recess. Unfortunately, gonioscopy is also subjective and thus has a lot of variability.9 Moreover, the technique is uncomfortable for both the patient and the surgeon. It is generally accepted that inadvertent compression during gonioscopy with Figure 1. An ultrasound biomicroscopy (UBM) image showing a narrow angle secondary to plateau iris anatomy. Note the large, anteriorly positioned ciliary process causing angle narrowing. a Zeiss-style lens may lead to artifactual opening of the angle and erroneous grading by the examiner. Perhaps the greatest limitation of gonioscopy is its lack of use. The examination is not performed in most glaucoma cases,10 possibly because many physicians feel that the assessment of the Van Herick grading is sufficient to determine occludability of the angle. The approach’s correlation with gonioscopy, although good, SEPTEMBER/OCTOBER 2014 GLAUCOMA TODAY 53 COVER STORY resolution can be up to 5 µm with Fourier-domain OCT (FD-OCT). The Visante OCT (Carl Zeiss Meditec) is a time-domain OCT device that scans the anterior segment, generating images that extend from limbus to limbus. FD-OCT units intended for posterior segment imaging are increasingly evolving to include anterior segment imaging. Compared to traditional time-domain AS-OCT devices, FD-OCT units have shorter wavelengths (typically 800-840 nm) and are less able to penetrate the angle recess. Although limbus-tolimbus scans are possible, the top of Figure 2. An anterior segment OCT (AS-OCT) image showing mild to moderate the cornea is usually removed from pupillary block causing narrowing of the angles. Note the anterior bowing of the image, because there is a limited the iris. depth of imaging. A new swept source FD-OCT device is not perfect, however, and there is a high probability (Casia SS-1000; Tomey Corporation) of missing clinically significant cases when only the Van can rapidly obtain high-resolution scans with threeHerick method is used.11 Also, peripheral anterior syndimensional reconstruction of the anterior segment. echiae or vertical quadrants cannot be viewed with this Using a 1,310-nm light source, similar to the Visante technique. OCT, the Casia SS-1000 can penetrate the angle recess. Approval of the device by the FDA is pending. ULTRASOUND BIOMICROSCOPY Downsides of OCT include a relatively high cost and Ultrasound biomicroscopy (UBM) is a relatively lowan inability to image deep to uveal tissues, including cost imaging technology that typically ranges from 25 to the iris. 75 MHz and has a resolution of about 50 µm (Figure 1). Traditional UBM involves the placement of an eyecup OTHER MODALITIES and a coupling solution for transmission of the echogenic Other modalities for imaging the anterior segment signal while the patient is supine. More recent advances include the Scanning Peripheral Anterior Chamber include containment of the coupling solution within a Depth Analyzer (model SM-70; Takagi Seiko) and the condom tip or plastic tip that is placed directly on the EyeCam (Clarity Medical Systems). Although the former ocular surface. UBM captures cross-sectional images is a noncontact device and is relatively inexpensive, it has of the anterior segment, typically to a depth of 5 mm. poor resolution and often provides poor visualization of Compared to optically based devices, UBM has the the angle recess. The EyeCam uses the RetCam (Clarity advantage of penetrating the iris and imaging the ciliary Medical Systems) to allow gonioscopy-like imaging of processes, important for distinguishing the anatomy of the angle. It requires direct contact with the eye using a the plateau iris from other causes of narrow or closed coupling agent. angles (Figure 2). Disadvantages of UBM include the need for a skilled CLINICAL RECOMMENDATIONS technician, the potential for corneal abrasion or discomIn my opinion, slit-lamp examination and gonioscopy fort due to its contact nature, the possibility of ocular are still the first line of diagnostic assessment for angle compression if the contact tip is used, and the difference closure. If found to have narrow or closed angles, my in anatomy related to supine positioning for the eyecup patients undergo AS-OCT for further screening. I also approach. order AS-OCT imaging to determine if the angle has opened adequately after a laser peripheral iridotomy. I OPTICAL COHERENCE TOMOGRAPHY may request UBM when I suspect plateau iris, iris cysts, a AS-OCT obtains a high-resolution cross-section of tumor, or other secondary causes of angle closure. the anterior segment without touching the eye. The (Continued on page 58) 54 GLAUCOMA TODAY SEPTEMBER/OCTOBER 2014 COVER STORY (Continued from page 54) Weigh in on this topic now! https://www.surveymonkey.com/s/GToday25 1. Do you currently use anterior segment imaging in your practice? Yes No 2. Are you considering purchasing a device to image the anterior segment? Yes No CONCLUSION Anterior segment imaging is an important facet of glaucoma care. The various devices have their own pros and cons, and the decision to use these modalities depends on their cost, technicians’ expertise, and medical professionals’ clinical preferences. n Shan Lin, MD, is a professor of clinical ophthalmology and the director of the Glaucoma Service, Department of Ophthalmology, University of California, San Francisco. He has a research relationship with Carl Zeiss Meditec. Dr. Lin may be reached at (415) 514-0952; [email protected]. 1. Tham YC, Li X, Wong TY, et al. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. In press. 2. Foster PJ, Johnson GJ. Glaucoma in China: how big is the problem? Br J Ophthalmol. 2001;85(11):1277-1282. 3. Wang D, Huang G, He M, et al. Comparison of anterior ocular segment biometry features and related factors among American Caucasians, American Chinese, and Mainland Chinese. Clin Experiment Ophthalmol. 2012;40(6):542-549. 4. Wang D, Qi M, He M, et al. Ethnic difference of the anterior chamber area and volume and its association with angle width. Invest Ophthalmol Vis Sci. 2012;53(6):3139-3144. 5. Wang D, He M, Wu L, et al. Differences in iris structural measurements among American Caucasians, American Chinese, and Mainland Chinese. Clin Experiment Ophthalmol. 2012;40(2):162-169. 6. Wang D, He Mingguang, Wu Lingling, et al. Dark-light change of iris parameters and related factors among American Caucasians, American Chinese, and Mainland Chinese. Curr Eye Res. 2012;37(7):599-605. 7. Wang D, Chiu C, He M, et al. Differences in baseline dark and the dark-to-light changes in anterior chamber angle parameters in whites and ethnic Chinese. Invest Ophthalmol Vis Sci. 2011;52(13):9404-9410. 8. Day AC, Baio G, Gazzard G, et al. The prevalence of primary angle closure glaucoma in European derived populations: a systematic review. Br J Ophthalmol. 2012;96(9):1162-1167. 9. Congdon NG, Spaeth GL, Augsburger J, et al. A proposed simple method for measurement in the anterior chamber angle: biometric gonioscopy. Ophthalmology. 1999;106(11):2161-2167. 10. Hertzog LH, Albrecht KG, LaBree L, Lee PP. Glaucoma care and conformance with preferred practice patterns. Examination of the private, community-based ophthalmologist. Ophthalmology. 1996;103(7):1009-1013. 11. Park SB, Sung KR, Kang SY, et al. Assessment of narrow angles by gonioscopy, Van Herick method and anterior segment optical coherence tomography. Jpn J Ophthalmol. 2011;55(4):343-350. CONTACT US Send us your thoughts via e-mail to [email protected]. 58 GLAUCOMA TODAY SEPTEMBER/OCTOBER 2014