Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
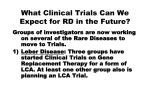
What is the retina and the macula? The retina is tissue that lines the back of the eye and is analogous with film in a camera. Within the retina are photoreceptors, which are light reactive cells that send a signal to the brain, allowing us to visually perceive the world around us. There are two types of photoreceptors, rods and cones. Of the two, only cones are able to detect color and give us the ability to distinguish separate colors. The highest concentration of cones is found within the macula and becomes sparser towards the periphery, or outer portion of the retina. Anatomically, the macula is located in the middle of the retina and is where the eye naturally focuses the light onto. It is from the macula that we get our clear, detailed, central field of vision for both distance and reading What is the choroid and RPE? Another important tissue involved in age-related macular degeneration is the choroid and the retinal pigment epithelial (RPE). The choroid is a thin blood vessel containing layer of connective tissue that is between the retina and the outer, white portion of the eye. It is responsible for supplying oxygen and nutrients to the photoreceptors in the retina. The layer that separates the retina and choroid is called the retinal pigment epithelial. It is responsible for destroying used photoreceptors and transporting waste from portions of the retina to the choroidal blood vessels. In macular degeneration, changes that can be seen occur in the RPE. What is Macular Degeneration and What Causes it? Age-related Macular Degeneration (AMD) is a condition affecting people over the age of 50 and is the leading cause of blindness in people over the age of 65. Damage to the macula in AMD occurs due to oxidative stress (oxygen free-radical molecules) and inflammation. Free radicals are created throughout life, typically from energy creation by cells and exposure to the sun, and are usually taken care of by antioxidants in the body. As the body ages, the choroid, RPE and retina become less efficient, allowing free radicals to build up in the retina. These free radicals cause damage (which leads to chronic inflammation) in the RPE and in turn the RPE becomes even less efficient. Since the RPE acts as the “pump” for the eye, digesting and excreting used up photoreceptors to the choroid, damage to this layer causes waste to build up under the retina. As this process occurs, yellow spots, known as drusen, form under the retina. “Hard drusen” form first and have a small, well defined shape. Hard drusen in the retina is not a sign of macular degeneration but rather is a part of the normal aging process (around 98.8% of those over the age of 49 have some small hard drusens). Studies have shown that a few small hard drusen is not a risk factor for developing AMD. In some cases, the RPE continues to degrade under hard drusen, causing waste material to “pool.” When this occurs, “soft drusen”, which are larger and less well defined then hard drusen, form. The presence of soft drusen is a high risk factor for developing AMD and once several medium sized soft drusen form, a diagnosis of macular degeneration is made. Sometimes fluid can build up under soft drusen, which leads to a pigment epithelial detachment (PED). A PED alone does not indicate wet AMD; however the risk of developing wet AMD is higher in patients who have one or more PED’s. It is important to get a fluorescein angiography and indocyanine green angiography to evaluate a PED. What are the risk factors for developing Age-related Macular Degeneration? Several risk factors that have been strongly correlated with the development of macular degeneration and/or the severity of macular degeneration include: Confluent soft drusen Having a family history of AMD (the gene coding for Complement Factor H has been shown to be associated with the development of AMD) Having blue or light colored eyes Smoking Long-term unprotected exposure to the sun. Other possible risk factors may include: Hypertension (high blood pressure) High cholesterol Having a diet high in fat Intermediate dry AMD with multiple soft drusen OCT image of a small pigment epithelial detachment What is Dry Macular Degeneration? Around 85% of patients with macular degeneration have the dry form and most people never progress beyond this stage. Dry macular degeneration is characterized by multiple, medium to larger sized soft drusens within the macula. There are three stages of dry AMD: early, intermediate and advanced. The early stage of AMD is characterized by only a small number (less than 20) of moderate size drusen and patients may or may not notice any vision changes. The intermediate stage of AMD is characterized either by numerous (over 20) moderate sized soft drusen or several large drusen. It is at the intermediate stage of AMD that most people notice changes in their vision. This change can be noticed on an Amsler Grid. As AMD progresses into the advanced stage, large areas of damaged tissue called geographic atrophy form, causing central blind spots, an in-ability to read or even legal blindness. What are the Symptoms of Dry Age-related Macular Degeneration? Common symptoms of Dry Macular Degeneration include: Straight lines appear wavy or there are blank spots in the lines when checked on a grid Increased blurriness while reading which is not correctable by glasses Increasing difficulty adapting to low light levels. For example, patient in clinic told us, “when walking into a dimly lit room from outside, it takes longer than it used to for my eyes to adapt.” Colors don’t look as bright or vivid. Need to constantly increase light levels when reading or performing close work. Gradual increase in over-all haziness covering your vision. Blurred or blind spot in the center of your visual field combined with a profound drop in the sharpness (acuity) of your central vision DIAGNOSING AMD When AMD is suspected, several tests are done to confirm the diagnosis and to determine if it is dry or wet. Optical Coherence Tomography scans are taken on all suspected and established AMD patients. If wet AMD is suspected, the doctor may order a fluorescein angiography and/or an indocyanine green angiography. Each of these tests has a specific role in the diagnosis and management of AMD. OCT scans: Optical Coherence Tomography (OCT) is the best way to image the retina and quantitatively track changes that occur. We use a Carl Zeiss Stratus Spectral Domain OCT, which is one of the highest quality machines available on the market today. The OCT uses a harmless scanning laser to take around 65,000 images of the retina (a 6mm x 6mm area, with the fovea at the center) within a 3-5 second period and creates a high definition image of the different layers. The OCT is able to detect very small changes within the retina (up to 5μm, which is 0.000196 inches) and with the ability to compare scans from different visits, any new developments can be seen by the doctor . Each eye will normally have 2 scans and the procedure will take a total of 2-5 minutes. One of the biggest limitations of an OCT is that since photos are taken over a short period of time, leakage activity from a CNV cannot be determined. Fluorescein Angiography (FA): When Wet AMD is suspected, or if you are at high risk of developing wet AMD, the doctor will order a fluorescein angiography (FA). This test is done in our clinic and you will not need to go to a separate testing facility to have it done. In order to perform the angiogram, the doctor will inject (using a very small butterfly needle) a mild vegetable based dye into one of your arm veins and the technician will take several pictures of your retina using a blue light over a 10 minute period. The dye is used to “light up” the arteries and veins of the retina and to detect any leakage and the rate of leakage that might be emanating from choroidal neovascularization. Both dry and wet AMD have specific patterns and will help the doctor make the correct diagnosis. Your doctor will explain the pictures to you in detail. One of the limitations of a fluorescein angiography is that the blue light used for imaging the retina is unable to penetrate the RPE significantly enough to image the choroid. Indocyanine Green Angiography (ICG-A): Though not done as often as FA imaging, ICG-A is usually performed in conjunction with fluorescein angiography. This type of imaging allows the doctor to evaluate the vasculature in the choroid by using infrared light, which is better able to penetrate the RPE than the blue light used in fluorescein angiography. ICG-A is an important diagnostic tool in detecting CNV’s that may otherwise have been missed by other imaging techniques. Several studies have shown that ICG-A was able to detect CNV’s in over 10% of suspicious cases which showed only dry AMD changes on fluorescein angiography or OCT. ICG-A is also a useful tool in the management of wet AMD. Over 85% of wet AMD cases have areas of poorly defined leakage on fluorescein angiography; however on ICG-A, a “hot spot” defining exactly where the leakage is coming from can usually be discovered. By tracking changes on ICG-A, the physician can better determine how a choroidal neovascular network is responding to treatment. C Fluorescein Angiography of dry AMD showing no leakage. Indocyanine green showing choroidal vasculature Treatments for Dry Age-related Macular Degeneration Currently there is no cure for AMD or treatment to reverse the damage due to AMD. For patients with intermediate to advanced dry AMD, eye vitamins can be effective in slowing the progression of the disease. AREDS eye vitamins (discussed below) is the only supplement shown in large clinical trials to be effective, however there are other trials with different formulas currently underway. AREDS Vitamin supplement A large study called the Age-Related Eye Disease Study (AREDS) demonstrated that eye vitamins reduced the risk of intermediate AMD progressing to advanced AMD by about 25%. The study also showed that patients with advanced AMD who used the eye vitamins were less likely to have severe vision loss. Eye vitamins consist of high doses of several natural antioxidents which helps prevent oxidative damage to the RPE. Below is a chart that compares the major eye vitamins available which use the AREDS formula. Though there are other types of eye vitamins available on the market, the AREDS formula is the only one shown in studies to be effective and are currently considered the standard of care. All the eye vitamins listed below are available over-the-counter. Name Company # /day Vitamin A* Vitamin C Vitamin E Zinc Copper Lutein** Alcon 2 28,640 IU 452 mg 400 IU 69.6 mg 1.6 mg 0 Alcon 2 6,600 IU 400 mg 150 IU 60 mg 4 mg 4 mg Ocuvite (smokers) Baush & Lomb 1 0 150 mg 30 IU 9 mg 1 mg 6 mg Preservision Preservision w/ Lutein (smokers) Baush & Lomb 2 28,640 IU 452 mg 400 IU 69.6 mg 1.6 mg 0 Baush & Lomb 2 0 452 mg 400 IU 69.6 mg 1.6 mg 10 mg I-Caps I-Caps w/ Lutein and Zeaxanthin (smokers) *Vitamin A is not recommended for smokers. ** Lutein is recommended for smokers. AREDS 2 vitamin supplement study This study, which is currently underway, is assessing the benefit of several changes to the formulation of the original ARED formula. This study still has many years to go, however what we learn from the study may redefine how we approach the treatment of dry AMD. Below is a description of these changes: Beta Carotene (Vitamin A): The use of vitamin A is not recommended for smokers and some studies have shown that it may not be beneficial to non-smokers. Some researchers have recommended that vitamin A be taken out of eye vitamins due to the possibility of chronic vitamin A toxicity. The AREDS 2 study is comparing supplements with and without vitamin A to determine if its use in eye vitamins is still warranted. Lutein and Zeaxanthin: Lutein and Zeaxanthin are natural chemicals found in the fovea and are important antioxidants that protect the eye. Research has shown that patients with AMD have low levels of both these chemicals. However we are not sure whether lower amounts of Lutein and Zeaxanthin is a result from or a cause of AMD. The AREDS 2 study is comparing the effectiveness of formulas with and without Lutein and Zeaxanthin. Some supplements currently available on the market offer Lutein and Zeaxanthin as a part of their formula. Omega-3: A large epidemiological study showed that the people who consumed fish had lower incidents of macular degeneration than those who rarely consumed fish. Another study showed that participants who reported the highest intake of Omega-3 (usually through supplements) were 30% less likely to develop advanced stages of AMD compared to those who had lower intakes of Omega3. Though Omega-3 seems to be a promising addition, the AREDS 2 study is evaluating its effectiveness against AMD. Aspirin and AMD There have been reports stating that use of aspirin is “causing” AMD in America. Though there have been a few reported cases of spontaneous conversion of dry AMD to wet AMD in people who were taking aspirin, the largest study performed to date on AMD (the AREDS study) showed no association between the formation of wet AMD and aspirin use. In-fact, the AREDS study showed that long-term use of aspirin actually decreased the incident of wet AMD. Also, daily aspirin use in conjunction with Omega-3 intake was more protective against wet AMD then either alone. If there are no contra-indications against the use of aspirin, taking 325 mg per day may be beneficial. Vitamin B and Folic Acid An observational study that followed 5,000 women over the age of 40 for 7 years showed that an intake of vitamin B6 (50mg/day), vitamin B12 (1mg/day) and folic acid (2.5mg/day) may reduce the risk of developing AMD by 35-40%. The study was actually done to determine the effects of vitamin B and folic acid on the risk of heart disease, however during the study, vitamin B and folic acid were found to have an effect on AMD. To date there have been no other studies to support the evidence and no large studies evaluating the effect of Vitamin B and folic acid specifically on AMD. Saturated Fat and Trans Fat It has been known for a long time that diet high in fat increases the risk of developing AMD. Recently, reports have been published specifically showing that higher intakes of saturated fat and trans fat responsible for the higher incidents of AMD. This could be explained by recent reports in the field of internal medicine showing that fat increases inflammation through-out the body. Since AMD has an inflammatory component, having higher inflammation through-out the body is like adding fuel to the fire. Diet and AMD What you eat is important. Studies have been published showing that patients who scored higher on the Alternate Healthy Eating Index (AHEI) had significantly reduced odds of developing AMD compared to those who scored low on the AHEI. The AHEI was developed by Harvard’s School of Public Health and Nutrition and has been shown in several studies to be more effective against chronic diseases than the government’s current food pyramid. An outline of the AHEI and practical guidelines can be found at http://www.hsph.harvard.edu/nutritionsource/what-should-you-eat/pyramid/ Dry AMD treatments in the future Dry AMD has taken the spot light in the Retina community and several new treatments are in the works. There are three main focuses of these new treatments: medications to preserve photoreceptors and the RPE, medications to prevent injury from oxidative stress and medications to suppress inflammation. Medication to preserve photoreceptors and the RPE: There are several medications in clinical trials right now that function to preserve the photoreceptors and RPE. Most of these medications are intended for patients with advanced dry AMD who have geographic atrophy. NT-501 is being developed by a company called Neurotech and is the only medication under this category that is being co-sponsered by the National Eye Institute. It is currently in stage 2 clinical trials and we will continue to follow-up on its progress. Medications to prevent injury from oxidative stress: AREDS 2 (see above) is a continuation of the first AREDS study, but with slight variations in the formulation. The added nutrients work to further “soak up” free radicals that damage the RPE and as a way to further decrease inflammation. Since clinical trials have recently begun, it will be several years before data becomes available. Medications to Suppress Inflammation: Since inflammation is a major component of AMD, a majority of medications being developed target this process. Some of these medications can be used to prevent the progression of AMD in patients with only drusen (early and moderate stage AMD). Glatiramer acetate (Copaxone) is a medication used for Multiple Sclerosis by acting as an immunomodulator (suppresses portions of the immune system). Copaxone down regulates a type of immune system cell called cytokines, which is one of the primary cells that cause inflammation in AMD. More trials are necessary to show the efficacy of this treatment. Final Thoughts on Dry AMD Though there is currently no cure for AMD and no way to completely prevent it from developing, it is still important to reduce or eliminate the associated risk factors and visit your retina specialists regularly for checkups. Treatments for dry AMD in the future will most likely take on a multi-faceted approach, both focusing on controlling the risk factors leading to advanced AMD and taking medications that target the underlying causes of AMD.