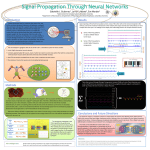
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Copyright 1997 by The Genmtological Society of America Journal ofGenmtologv: BIOLOGICAL SCIENCES 1997. Vol. 52A. No. s! B26O-B266 Effectiveness of Individualized Aerobic Training at the Ventilatory Threshold in the Elderly Claudine Fabre, Janick Masse-Biron, Said Ahmaidi, Brigitte Adam, and Christian Prefaut Laboratory of Interaction Physiology, Hopital A. de Villeneuve, Montpellier, France. This study was designed to specify whether an individualized training program at the ventilatory threshold in elderly subjects produces greater training adaptations than a standardized training program performed at 50% of heart rate reserve. Sixteen subjects participated in the study. Maximal exercise tests were performed on a treadmill before and after the training program. Eight subjects trained at the ventilatory threshold (ITG) and eight trained at 50% of heart rate reserve (STG). The mean training heart rate was 129 ± 14.2 bpm and 115 ± 7.9 bpm in the individualized training group (ITG) and the standardized training group (STG), respectively. The maximal O2 uptake (VOiinax) was improved significantly by 20% in ITG (within group p < .05), whereas no significant improvement was noted in STG. The improvement in ITG compared to the nonsignificant change in STG was significant (p < .05). In addition, submaximal ventilation and heart rate were more decreased in ITG than STG. We conclude that for elderly people an individualized training program at the level of the ventilatory threshold is significantly more effective in terms of V02max and submaximal cardiorespiratory adaptations. E NDURANCE training has been shown to be an effective method for improving both physical fitness and health in elderly subjects (Pollock et al., 1976; Shepard, 1988). For decades, the training prescriptions have been based on percentages of maximal oxygen uptake (% V0 2 max), maximal heart rate (% HRmax), or heart rate reserve (% HRr) (Malher et al., 1986). However, Katch et al. (1978), studying normal healthy elderly subjects, and Vallet et al. (1997), studying elderly chronic obstructive pulmonary disease (COPD) patients, showed that at a preselected % HRmax, individual subjects may exercise above or below their anaerobic threshold and thus exhibit dissimilar responses. Thus, these nonindividualized methods, based on the relative-percent concept, make it difficult to evaluate a given individual's exercise stress. The heart rate recorded at the ventilatory threshold (VT), described by Wasserman et al. (1973), may be a better basis for activity prescription than an arbitrary relative-percent for at least three reasons. First, VT takes into account a specific level of metabolic stress, resulting in more homogeneous responses to training than an arbitrary percentage of V02max or HR. Second, VT differs among people as a function of age, gender, physical fitness, health, etc., in such a way that training at the VT is in fact individualized. Third, because VT marks the breakpoint in ventilation, we can expect, from a ventilatory point of view, a good compliance with the training program — particularly because it has been observed that VT occurs at the same load level as the dyspnea threshold (Quantin et al., 1996). We have used individualized training programs at the VT in asthmatic children and COPD patients and obtained very good results (Varray et al., 1991; Ahmaidi et al., 1993; Vallet et al., 1997). This study was designed to determine whether, in elderly subjects, an individualized training program (ITG) at the ventilatory threshold leads to greater training responses than standardized training programs (STG) performed at B260 50% of heart rate reserve (50% HRr). Indeed, the American College of Sports Medicine (1978) recommends a training heart rate of 50 to 85% of heart rate reserve. The training heart rate at 50% HRr was chosen because the elderly subjects were sedentary and had a poor level of conditioning. METHOD Subjects. —Twenty-five retirees, 8 men and 17 women, recruited from the Universite de la Culture Permanente in Nimes, France, expressed interest in a vigorous walking program to improve functional capacity and aerobic fitness. Before admittance to the study, all subjects were evaluated for their cardiorespiratory health. Subjects having abnormal spirometric data, abnormal 12-lead electrocardiograms (ECG), a supine blood pressure greater than 165/100 mmHg, ST segment depression, or significant arrhythmias during exercise testing were excluded from the study. Three subjects were excluded because of heart disease as shown by the medical history and physical examination; thus, 22 subjects initially participated in the study. However, of the original 22 subjects, only 16 completed their training program so that the study ended with each group composed of eight subjects. Two participants (one in ITG and one in STG) developed medical problems unrelated to training, three (two in ITG and one in STG) did not complete the required number of training sessions, and another subject (STG) developed an inadequate rise in systolic blood pressure at the final examination (T3). These six subjects were dropped from the analysis. Subjects who were on medication for hypertension, rheumatism, or depression at the time of the first examination maintained the same therapeutic regimen throughout the study. The subjects (aged 64 ± 6.8 years, range 53-74) had active life styles, but none had performed any regular physical training for several years. Their activities — utility TRAINING AT THE VENTILATORY THRESHOLD walking, gardening, and mild indoor gymnastics — continued throughout the training program. Participants were, however, discouraged from performing other vigorous activities during the 12-week program. The anthropometric characteristics and initial cardiorespiratory values are given in Tables 1 and 3. After the procedures were explained in detail, all subjects provided written consent. Spirometry. — The maximum expiratory flow curves were recorded on a digital spirometer (Datalink Pulmochart, Marne la Vallee, France) in order to record the forced expiratory volume in one second (FEV,). In addition, we calculated maximal voluntary ventilation (MVV = FEVi X 35; Gandevia and Hugh-Gions, 1957) and the ratio of maximal exercise ventilation to MVV (% MVV). Physical measures. — Oxygen consumption (VO2) was determined using an open circuit technique. The subjects breathed through a rubber mouthpiece attached to a oneway valve (Warren E. Collins, Braintree, MA) with low resistance and small dead space (90 ml). Inspiratory airflow was measured continuously during exercise through a pneumotachograph (Fleich no. 3) and a pressure transducer (MP45, Validyne Engineering Corp., Worthridge, CA) with a measuring range of ± 2 cm H2O. The pneumotachograph was placed on the inspiratory tubing in order to avoid problems due to water vapor. The calibration of the flow module was accomplished by introducing a calibrated volume of air at several flow rates. Expired gases were sampled in a mixing chamber (5-1) through a flexible hose dried with CaCl2 and analyzed for O2 with a polarographic analyzer (Godard Capnographe, Statham, Netherlands) and for CO2 with an infrared analyzer (Godard Rapox, Statham, Netherlands). Each gas analyzer was calibrated before and after each test according to a standard certified commercial gas preparation. The inspiratory air flows and the fraction of expired O2 (FeO2) and CO2 (FeCO2) were measured and computed from the last 10 breath cycles of every minute. Averages were established for minute ventilation (VE l.min~' BTBS [body temperature pressure saturated]), VO2 (l.min"1 STPD [standard temperature pressure dry]), CO2 production (VCO2 l.min-1 STPD), respiratory ratio (R), and ventilatory equivalents for O2 (VE/VO2) and CO2 (VE/VCO2). During the test each subject's electrocardiogram was followed continuously on a cardioscope (Diascope, Simonsen and Weel, Copenhagen, Denmark). Electrodes were placed in the CM5 lead position. The heart rate was also assessed with a cardiofrequency meter (Sportester PE 3000, Polar Electro, Kemple, Finland). The arterial pressure was continuously recorded on a tensionmeter (Quinton Q 3000, Seattle, WA). The maximal oxygen pulse (VO2max/HRmax) was expressed in ml.bpnr1. Maximal exercise test. — The test was performed on a motor-driven treadmill (Gymrol 1800, Roche la Moliere, France). VO2 was determined using a modified Balke and Ware (1959) protocol. The speed of the treadmill was individualized from the value of heart rate at rest plus 25 bpm and remained fixed during testing. During the determination of treadmill speed the subjects familiarized themselves B261 with the test procedures. The grade after 3 min of warm-up was increased by 1.25% every minute until exhaustion. The observation of three of the four following criteria was necessary to assume that the subjects had reached their V0 2 max: (J) stability of VO2 in spite of the increase in work load; (2) stability of HR at a value close to the theoretical maximal HR, i.e., 210-.65 X age ± 10; (3) R > 1.10; and (4) the inability of the subject to maintain the walking speed. Before and after each test the accuracy of the treadmill speed was verified by a stopwatch recording of 15 treadmill belt revolutions. After completion of the exercise test, the VT was determined for each subject by using the V-slope method of Beaver et al. (1986). This method involves the analysis of the behavior of VCO2 as a function of VO2 and assumes that the threshold corresponds to the break in the linear VCO2-VO2 relationship; indeed, this threshold is also called the gas exchange threshold (GET) (Patessio et al., 1993). The reading was effected independently by two experienced investigators. In the rare case of discordance, the criteria of Wasserman et al. (1973) were used to reach a consensus or to eliminate the subject. In this study a consensus was always reached. The difference observed between the two investigators did not exceed 3%. Protocol. — The subjects were tested before training (TO) and after a 3-month aerobic training period (T3) (physical, clinical, and spirometric examination and maximal exercise testing). After the first test, the subjects were randomized into two groups (each n = 8), and training heart rate (HRt) was determined. The standardized training group (STG) trained at the standard level of 50% heart rate reserve (HRt 50%) equal to 50% X (HRmax - HRrest) + HRrest. The individualized training group (ITG) trained at the heart rate corresponding to the gas exchange threshold (HRt GET). The two groups showed no significant differences concerning age, sex, weight, height (Table 1), HRt GET, HRt 50% (Table 2), initial V02max (Table 3) and life style. The subjects did not know which method had been used to determine their training heart rate. Training program. — The training program consisted of interval walking to HRt intensity twice a week on an outdoor running track under the supervision of study personnel. The principle of interval training is to alternate between periods of exercise at the target heart rate and active recovery. An example of a training session can be seen in Figure 1. Each session differed in order to maintain high motivation, e.g., in Session 1 the exercise was presented as 400 m X 8; in Session 2, 800 m X 4, etc. However, total time spent at the target heart rate was slowly increased over sessions as subjects progressed with a concomitant reduction in recovery time. All sessions were preceded by a 10-min warm-up (stretching and self-massage) and ended with a 10-min cooldown (stretching and relaxation). The interval walking durations progressively increased so that by the end of the training period, subjects were exercising for one full hour. A work technique (respiratory movements in coordination with walking rhythm, stride length, velocity, etc.) was proposed at each session. During training, HRt was continuously recorded by means of a cardiofrequency meter (Sportester PE 3000, Polar FABRE ETAL. B262 Table 1. Anthropometric Characteristics of Standardized Training Group (STG) and Individualized Training Group (ITG) Subjects, n Age, years Sex Height, cm Body mass, kg STG 1 2 3 4 5 6 7 8 Mean ± SD 63 67 64 57 74 71 62 53 63.9 ± 6.8 F F M F F M M F 149 152 173 159 145 175 164 144 157.6+ 12.2 46 48 75 56 41 84 73 47 58.7 ±16.4 ITG 1 2 3 4 5 6 7 8 Mean ± SD 65 65 64 57 63 69 57 63 62.9 ± 3.9 F M F F F M M F 148 182 155 166 157 180 179 161 166 ± 13 59 103 62 48 46 84 87 59 68.5 ± 20.6 n.s. n.s. Differences between groups n.s. Note: n.s. = not significant. Electro, Kemple, Finland). The accuracy of this monitor was established by comparing its results with the pulse rate monitored with actual ECG recordings during exercise on the treadmill. The cardiofrequency meter was set in such a way that subjects could exercise within ± 5 bpm of prescribed intensity. An alarm sounded when the HR of the subject was out of the preselected range. After each session, the HRt was checked from the generated HR curves (Figure 1). Walking/running tests were periodically performed on a 400 m running track to measure the. walking speed at HRt; this was done to assess the modifications in submaximal performance. The first test (Test 1) was conducted after one month of training, the time deemed necessary for the subjects to achieve a stable HRt. The second test (Test 2) was performed at the end of the 3-month training period. The HRt was monitored with data from the Sportester, and the speed was measured in km.h"1. Statistical analysis. — The data collected on entry were compared for homogeneity, HRt at GET and HRt 50% between the two groups using an unpaired Student's /-test. The walking speed at HRt measured before and after training was analyzed by an unpaired Mest on the mean differences. An analysis of variance (ANOVA), with group as a between-subject factor and time a within-subject factor, was performed on variables at rest, and at submaximal and maximal intensities. When the ANOVA F ratio was significant (p < .05), we tested for significant differences in terms of between-group and within-group effects and Group by Time interaction. Table 2. Values of Heart Rate (bpm) Used for Training Intensities Subjects, n STG 1 2 3 4 5 6 7 8 M±SD ITG 1 2 3 4 5 6 7 8 M±SD HRmax HR rest HR GET 50% HRr HRGET % HRmax 50% HRr % HR max 154 162 145 165 150 150 160 180 158 ±9.6 80 68 52 68 65 83 90 58 70 ±13 133 125 100 122 131 137 135 134 127 ±12.2 117 115 99 117 108 117 125 120 115 ±7.9 86 77 69 73 87 91 84 74 80 ± 7.9 76 71 68 71 72 78 78 66 73 ±4.5 176 140 160 156 155 178 152 183 162 ± 15 65 71 72 80 70 144 108 134 130 135 128 110 146 129 ±14.2*** 120 105 116 118 113 81 77 83 83 87 72 72 81 79 ±5.6 68 75 72 75 72 65 78 80 73 ± 6.2 122 115 132 118 ±7.9 68 75 72 72 ±2.8 Notes: HR = heart rate; HR GET = HR corresponding to the gas exchange threshold; 50% HRr = 50% of HR reserve; HR GET % HRmax = value of HR GET in % HRmax; 50% HR % HRmax = value of 50% HRr in % HRmax; STG = standardized training group; ITG = individualized training group. ***/; < .001 between HR GET and 50% HRr. TRAINING AT THE VENTILATORY Table 3. Cardiorespiratory Responses to Maximal Exercise and at the Gas Exchange Threshold Before (TO) and After 3 Months of Training (T3); Means ± SD STG ITG p-value of Interaction , l.mirr TO T3 1.50 ± 0.53 1.59 ± 0.56 V02max, ml.kg '.min 1 TO T3 25.45 ± 6.79 26.87 ± 3.96 HRmax, bpm TO T3 158 ± 9.60 157 ± 11.31 Peak O2 pulse, ml.bear' TO T3 16± 0.02 17± 0.01 1.77 ± 0.79 2.11 ± 0.96** 25.42 ± 5.65 30.63 ± 8.48* <.O5 162 ± 15 162 ± 8.48 n.s. 16± 0.01 20 ± 0.02* n.s. VO2 at GET, ml.kg-'.minTO T3 15.37 ± 3.68 17.36 ± 2.57* 14.84 ± 3.68 18.96 ± 2.69* n.s. GET, % VO2max TO T3 61.10 ± 11.88 67.50 ± 7.64 60.50 ± 16.4 63.70 ± 13.01 n.s. 127 ± 12.2 126 ± 8.48 129 ± 14.2 136 ± 11.31 n.s. HR GET, bpm T3 B263 expressed as ± SD. In addition, the 95% confidence interval is given when helpful. The limit for statistical significance was always set at p < .05. RESULTS Clinical adaptation to training. — Adherence to the <.O5 1 TO THRESHOLD Notes: STG = standardized training group; ITG = individualized training group; VO2max = maximal O2 uptake; HRmax = maximal heart rate; GET = gas exchange threshold; HR GET = heart rate at GET; n.s. = not significant. *p < .05; **p < .01, within group comparison. Time (minutes) Figure 1. Example of interval walking program of ITG subject no. 3. This shows the HR during a training session. Hit = 138 bpm. The exercise sequences lasted one minute, each followed by one minute of recovery. This was repeated three times (a) and followed by exercise sequences of 2 minutes with the same recovery, three times (b); and then by 4-minute sequences, also with one-minute recoveries (c). The session finished with two exercise sequences of 10 minutes with a 3-minute recovery between them (d). The VE and HR kinetics for each subject were calculated as a function of VO2 using a logarithmic equation of the relation between these parameters and VO2. The values of VE and HR were calculated before and after training at 60%, 80%, and 100% of pretraining V02max. The values are reported as means. Dispersion around mean values is training programs for the subjects was very good. There were no injuries or untoward events associated with the walking program. The mean of HRt in STG was 115 ± 7.9 bpm (range 99-125). The mean of HRt in ITG was 129 ± 14.2 bpm (range 108-144). Therefore, HRt at GET was significantly higher (p between groups < .001). Moreover, HRt was much more variable in the ITG than in the STG group (Table 2). After 4 weeks of training, it was necessary for the following subjects — 3, 4, 6 of STG and 5, 7, 8 of ITG — to alternate walking and jogging in order to train at the exact HRt. At Test 1 of the 400 m running track test, the walking speed at HRt was 5.91 km.h-1 (range 4.2-6.8) in STG and 6.07 km.h"1 (range 4.2-7) in ITG. At Test 2, the walking speed at HRt was 6.02 km.h-1 (range 4.2-6.8) in STG and 6.62 km.rr1 (range 5-7.5) in ITG. The change in walking speed at HRt (Test 2 - Test 1) was significantly higher in ITG (0.6 ± 0.08) than in STG (0.1 ± 0.10 km.h-1), with significant differences between groups (p < .01). Responses at rest. — Before training, the mean HR in ITG was 70 ± 13; after training, it was reduced, though not significantly, to 68.7 ± 10.6. In STG, HR was 73 ± 6.2 and after 3 months of training it was reduced, again not significantly, to 71.8 ± 8.8. Responses to maximal exercise. — Concerning the V0 2 max, we noted a greater adaptation after training in ITG compared to STG, demonstrated by the significant Group by Time interaction (p < .05). The significant improvement in V02max was 20% in ITG (p < .05), whereas no significant change appeared in V0 2 max for STG (Table 3). For this variable, the 95% confidence interval (CI) of differences between T3-T0 was -.07 to .25 l.min-' for STG and .11 to .57 l.min-' for ITG. The HRmax was not statistically different between the two groups initially, and it remained unchanged after training. We observed a significant increase in maximal O2 pulse in ITG after training (p within group < .05); there was no significant change in STG, and the Group by Time interaction was not significant (Table 3). The VEmax of both ITG and STG was increased as a function of time during training (p within each group < .01); thus, the differences between the two groups were not significant (Table 4). Furthermore, for both groups, no differences were observed in maximal VE/VO2 and MVV (Table 4). At T3 the % MVV was increased in ITG (p within group < .05) (Table 4). Responses to submaximal exercise. — VO2 at the GET was increased in both groups (p within each group < .05) as a function of training, but the difference between the two groups was not significant (Table 3). We assessed VE and HR for the same absolute VO2 B264 FABRE ETAL. Table 4. Ventilatory Responses to Maximal Exercise Before (TO) and After (T3) Training; Means ± SD /j = 8 ITG n=8 p-value of Interaction VEmax, l.miir1 BTPS TO T3 53.6 ± 17.2 55.8 ±16.1** 59.9 ± 11.9 72.9 ± 12.8** n.s. VE/VO2 TO T3 30.9 ± 6.8 31.1 ± 5.6 26.7 ± 6.5 28.0 ± 4.5 n.s. MVV TO T3 76.3 ± 24 75.7 ± 24.3 83.9 ±16.9 73.2 ±28 n.s. %MVV TO T3 72.6 ±21.2 74.8 ± 12.4 69.6 ± 28 81.9 ±25.7* n.s. STG Notes: STG = standardized training group; ITG = individualized training group; VEmax = maximal minute ventilation; VE/VO2 = ventilatory equivalent for Oy, MVV = maximal voluntary ventilation; % MVV = percentage of MVV; n.s. = not significant. *p <.O5; **p < .01, within group comparison. Table 5. Reductions With Training in Ventilation and Heart Rate STG n=8 ITG i VE l.min"1 HR bpm VE l.min"1 HR bpm -2.0 ± 3.7 n.s. - 6 ± 5.6 p<.05 -8.3 ± 9.6 - 1 4 ± 11 .3 80% -0.3 ±5.1 n.s. - 5 ± 11.3 n.s. -7.5 ±11.9 n.s. -14± 14 .1 p < .05 100% -4.9 ± 13 n.s. - 4 ± 5.6 n.s. -12.1 ± 18.1 n.s. -14± 11 .3 p<.0\ %V0 2 maxatTO 60% p<.05 p<.0\ Notes: STG = standardized training group; ITG = individualized training group; TO = before training; T3 = 3 months after training; VE = minute ventilation; HR = heart rate; % VO2max = percentage of the maximal oxygen uptake; n.s. = not significant. Values ± SD represent changes in VE and HR from TO to T3, measured at 60, 80, and 100% of the initial V0 2 max(V0 2 maxatTO). (60%, 80%, and 100% of pretraining VO2max) by the delta values between TO and T3. For these levels, the modifications were slight and not significant in STG except for HR at 60% of V02max, which was decreased by 6 ± 5.6 bpm (p within group < .05). In ITG, the decrease in VE was marked and significant at 60% of VO2max (35% reduction in VE, p within group < .05). The HR in ITG was systematically decreased at 60%, 80%, and 100% of V02max, for/? within group < .01,/? < .05, and/? < .01, respectively (Table 5). Individualized training at 50% heart rate reserve. — In three subjects of ITG, the HRt GET was, in fact, at 50% of their heart rate reserve (subjects 2, 6, and 7). In two subjects of STG, HRt 50% was at the level of HRt GET (subjects 3 and 4). Therefore, in five subjects, the training was conducted at a HRt GET which was, in fact, at 50% of heart rate reserve (113.6 ± 11.3 bpm vs 116.6 ± 9.4 bpm). In these five subjects, VO2max increased from 2.29 ± 0.73 l.min 1 at TO to 2.51 ± 1.00 l.min 1 at T3, an increase of 10%. DISCUSSION This study indicates that an individualized training program at the ventilatory threshold (determined in terms of gas exchange threshold) is very well tolerated by the sedentary elderly even if it is conducted at a higher heart rate than a standardized program at the level of 50% of heart rate reserve. Because it is conducted at a higher intensity, the individualized program is significantly more effective than the standardized program in terms of improving V02max and submaximal cardiorespiratory adaptations. The training intensity was not readjusted at midpoint in the program. Indeed, it is possible that GET would have increased and HR would have decreased. However, the decrease in resting HR was not significant after training, and Vallet et al. (1994) showed that HR at GET after one and two months of aerobic training was not modified in spite of an increase in GET in COPD patients. Therefore, we assume that the effect of this absence of readjusted training intensity was minor. In the literature, there are no cardiorespiratory differences reported at rest (VO2, HR, VE) between young sedentary and older sedentary people (De Vries and Adams, 1972; Heath et al., 1981; Levy et al., 1993); however, differences have been noted during exercise. VE and ventilatory equivalent for O2 (VE/VO2) are greater in older sedentary subjects compared to young subjects (De Vries and Adams, 1972) for all work levels. Inbar et al. (1994) demonstrated that for an intensity below 50% of VO2, aging did not influence the cardiorespiratory responses to exercise, but that after this load it did. The variables studied by Inbar et al. (1994) were VCO2, HR, O2 pulse, VE, Vt, and f. By aerobic training at a standardized intensity, elderly subjects can reduce hyperventilation and VE/VO2 during submaximal exercise and increase their GET (Yerg et al., 1985; Makrides et al., 1990; Poulin et al., 1992). The present study showed that with an individualized training program the adaptations of these different variables are better than with a standardized intensity during the same period of training. This phenomenon was also observed in COPD patients who followed either an individualized program at the GET or a standardized training program (Vallet et al., 1997). It is well known that endurance exercise training in elderly persons can elicit sizable increases in V02max, as it does in younger individuals (Seals et al., 1984; Hagberg et al., 1989; Makrides et al., 1990). The improvement in V02max as reported in the literature has ranged from 7 to 38% (Sidney and Shepard, 1978; Badenhop et al., 1983; Seals et al., 1984; Thomas et al., 1985; Yerg et al., 1985; Blumenthal et al., 1989; Hagberg et al., 1989; Makrides et al., 1990; Masse-Biron et al., 1990; Blumenthal et al., 1991), and this emphasizes the need to optimize the training programs. The discrepancies observed may be due to differences in duration, intensity, or frequency of training. Since the late 1980s it has been recognized that prolonged endurance exercise training can elicit substantial cardiores- TRAINING AT THE VENTILATORY THRESHOLD piratory adaptations even in men and women in their 70s (Hagberg et al., 1989). The exact role of intensity, however, is not yet well understood. Preselected percentages of V02max, HRmax, and HRr are usually used to determine the intensity, although as early as 1978, Katch et al. showed that at a preselected percentage of HRmax, subjects may exercise above or below their GET. During work at 80% HRmax, for example, half of their subjects remained below their GET and exhibited fewer training responses. Therefore, programs using prescriptions based on the relativepercent concept may create multiple training stimuli among the participants, which in turn results in a wide range of improvement in cardiorespiratory and metabolic functions (Dwnyer and Bybee, 1983). This observation suggests that an exercise intensity based on the relative-percent concept may have limited usefulness in ensuring that a desired level of metabolic stress is attained for all subjects. The assumed relation of GET to fuel use and lactate accumulation indicates that its use in training prescriptions may define a better metabolic level and more precise training stimuli. Moreover, individualization of training intensity can maximize compliance to the training program. To our knowledge, exercise in the elderly has been prescribed on the basis of anaerobic threshold only in three studies. However, in the first investigation, Belman and Gaesser (1991) did not train their subjects at the level of lactate threshold but at an intensity above this threshold. Takeshima et al. (1993) trained elderly subjects at the anaerobic threshold and showed an improvement in V02max of about 10%. Last, the exercise intensity was also at the anaerobic threshold in the study of Motoyama et al. (1995), but no cardiorespiratory parameters were studied. We chose to compare individualized training at the GET to a standardized training program performed at 50% of heart rate reserve. Indeed, the American College of Sports Medicine (1978) recommends a general range of training intensities from 50-85% of heart rate reserve, but insists on the importance of starting sedentary subjects at 50% of HRr, which is usually done (Badenhop et al., 1983; Seals et al., 1984; Yerg et al., 1985; Blumenthal et al., 1991; Levy et al., 1993). As the GET in our study was at 60% HRr, we in fact compared training programs at two levels of intensity in sedentary elderly subjects, the highest intensity being also based on the principle of individualization. Whatever the training intensity, training programs were clinically very well tolerated, and subjects of both groups expressed the same enthusiasm for the various exercise components. Previous studies have generally shown that in the elderly, high-intensity training elicits greater increases in aerobic capacity than low-intensity training (Sidney and Shepard, 1978; Seals et al., 1984; Makrides et al., 1990; MasseBiron et al., 1990). According to these studies, the difference in the improvement in V0 2 max that we recorded between the two groups was first due to the difference in training intensity. Whether the specific metabolic level and the individualization of training enhanced the improvement of V02max in ITG is difficult to assess in our study. However, in those five subjects in whom GET was at 50% of HRr, the improvement in V02max was 10% (versus 6% in B265 the entire 50% HRt group), suggesting that individualized training is more effective; this finding must be confirmed by further studies. The 20% increase in VO2max observed in the ITG group is in the middle range of improvements for this parameter, as reported by previous studies (Sidney and Shepard, 1978; Yerg et al., 1985; Hagberg et al., 1989; Masse-Biron et al., 1990). The STG group, on the contrary, corresponded to a low-intensity training group with a slight, but nonsignificant, change in V02max (6%). The 95% confidence intervals calculated for V0 2 max were equivalent; thus, the nonsignificant VO2max change in STG cannot be due to excessive heterogeneity in this group. The data of Belman and Gaesser (1991) showed different results. By training elderly subjects at intensities above and below the lactate threshold, they observed in both groups a small increase (7%) in VO2max. Their high-intensity group was trained at a heart rate very close to that of our ITG group. The small improvement in their V02max could be explained by a shorter program (8 vs 12 weeks), and most likely by their using a 30-min continuous training program versus a progressively increased interval training program. This observation is also true for the study of Takeshima et al. (1993), who used the anaerobic threshold for the intensity of exercise but observed only an improvement of 10% in V02max. Indeed, an interval training program seems to be more effective. Makrides et al. (1990) showed a 38% increase in peak O2 with interval training consisting of repeated 5-min bouts of high-intensity exercise (140 bpm, 85% of peak VO2) separated by recovery periods at a lower intensity (65% of peak VO2). It is more difficult to explain why the low-intensity training of Belman and Gaesser (1991) was just as effective as their high-intensity training in improving V02max. An important difference between our two groups was the dispersion of the training heart rate. In the ITG group the mean HRt was 129 bpm and the standard deviation was 14.2 bpm. In the group trained at 50% HRr these values were, respectively, 115 and 7.9 bpm. In the ITG, the standard deviation of the mean of the training heart rate was therefore almost twice that of the 50% HRr group. Such a large inter-individual difference in HRt in the former group is very much consistent with the notion of individualized training. Training effectiveness is usually evaluated in terms of V02max. However, the aims of training programs are not only to increase aerobic capacity. In our experience, it is at least as important to improve exercise tolerance at submaximal levels. In the STG group, we observed only a small decrease in heart rate (-6 bpm), consistent with the decrease reported by Hagberg et al. (1989) for subjects trained at the same intensity. In the ITG group, we observed a significant decrease in heart rate (-14 bpm) at each submaximal level with a less substantial change in VE, smaller than that described by Makrides et al. (1990). The shift to the right of GET in both groups indicates a better O2 delivery to the contracting muscles and/or reduced diffusion distance from capillary to mitochondria, which is consistent with the post-training reduction in lactacidemia in the elderly that we have previously described (Masse'-Biron et al., 1992). The dissociation in both groups between the B266 FABRE ETAL. uniform improvement of GET and the non-uniform improvement in V02max is consistent with the idea that the mechanisms responsible for these improvements are probably dissociated (Belman and Gaesser, 1991). In 1985, Cunningham et al. suggested that because the VT occurs at a relatively high percentage of V02max in the elderly, the use of % V02max as a guide for exercise prescription in this population may underestimate the necessary stimulus for inducing a training effect. The present results support this hypothesis and show that using the VT, an individualized variable, as a guide for exercise prescription induces improvements in aerobic capacity and in submaximal exercise tolerance. Although individualized training programs seem to be very effective for the elderly, they are difficult to prescribe on a large scale because of current difficulties in conducting exercise tests for every applicant. Therefore, standardized training programs may remain useful. In this case, our results have clearly demonstrated that 50% HRr is too low a training intensity and that using 60% HRr should be a better basis for standardized training programs in healthy elderly subjects. ACKNOWLEDGMENTS This work was supported by INSERM Grant 931102. Address correspondence to Dr. Claudine Fabre, Laboratoire de Physiologie des Interactions, Service d'Exploration de la Fonction Respiratoire, Hopital A. de Villeneuve, 34295 Montpellier, Cedex 5, France. E-mail: [email protected] REFERENCES American College of Sports Medicine. Position statement on the recommended quantity and quality of exercise for developing and maintaining fitness in healthy adults. Med. Sci. Sports Exerc. 10:vii-x; 1978. Ahmaidi, S.; Varray, A.; Savy-Pacaux, A.; PreTaut, C. Cardiorespiratory fitness evaluation by the shuttle test in asthmatic subjects during aerobic training. Chest 103:1135-1141; 1993. Badenhop, D.; Cleary, A.; Shaal, F.; Fox, E.; Bartel, R. Physiological adjustment to higher or lower intensity exercise in elders. Med. Sci. Sports Exerc. 15:496-502; 1983. Balke, B.; Ware, R. An experimental study of physical fitness of Air Force personnel. US Armed Forces Med. J. 10:675-688; 1959. Beaver, W.; Wasserman, K.; Whipp, J. A new method for detecting anaerobic threshold by gas exchange. J. Appl. Physiol. 60:2020-2027; 1986. Belman, J.; Gaesser, G. Exercise training below and above the lactate threshold in the elderly. Med. Sci. Sports Exerc. 23:562-568; 1991. Blumenthal, J.; Emery, C ; Madden, D.; George, L.; Coleman, R.; Riddle, M.; McKee, D.; Reasoner, J.; Williams, R. Cardiovascular and behavioral effects of aerobic exercise training in healthy older men and women. J. Gerontol. Med. Sci. 44:M147-M157; 1989. Blumenthal, J.; Emery, C ; Madden, D.; Coleman, R.; Riddle, M.; Schniebolk, S.; Cobb, F ; Sullivan, M.; Higginbotham, M. Effects of exercise training on cardiorespiratory function in men and women > 60 years of age. Am. J. Cardiol. 67:633-639; 1991. Cunningham, D.; Nancekievill, E.; Paterson, D.; Donner, A.; Rechnitzerl, P. Ventilatory threshold and aging. J. Gerontol. 40:703-707; 1985. De Vries, H.; Adams, G. Comparison of exercise responses in old and young men: II. Ventilatory mechanics. J. Gerontol. 27:349-352; 1972. Dwnyer, J.; Bybee, R. Heart rate indices of the aerobic threshold. Med. Sci. Sports Exerc. 15:72-76; 1983. Gandevia, B.; Hugh-Gions, P. Terminology for measurements of ventilatory capacity. Thorax 1:290-293; 1957. Hagberg, J.; Graves, J.; Limacher, M.; Woods, D.; Leggett, S.; Cononie, G; Gruber, J.; Pollock, M. Cardiovascular responses of 70-79 year old men and women to exercise training. J. Appl. Physiol. 66:2589-2594; 1989. Heath, G.; Hagberg, J.; Ehsani, A.; Holloszy, J. A physiological compari- son of young and older endurance athletes. J. Appl. Physiol. 51: 634-640; 1981. Inbar, Ov, Oren, A.; Scheinowitz, M.; Rotstein, A.; Dlin, R.; Casaburi, R. Normal cardiopulmonary responses during incremental exercise in 20to-70-yr-old men. Med. Sci. Sports Exerc. 26:538-546; 1994. Katch, V.; Weltman, S.; Freedson, P. Validity of the relative percent concept for equating training intensity. Eur. J. Appl. Physiol. 39:219-227; 1978. Levy, W.; Cerqueira, M.; Abrass, I.; Schwartz, R.; Stratton, J. Endurance exercise training augments diastolic filling at rest and during exercise in healthy young and older men. Circulation 88:116-126; 1993. Makrides, L.; Heigenhauser, G.; Jones, N. High-intensity endurance training in 20- to 30- and 60- to 70-year-old healthy men. J. Appl. Physiol. 69:1792-1798; 1990. Malher, D.; Cunningham, L.; Curfman, G. Aging and exercise performance. Clin. Geriatr. Med. 2:433-453; 1986. Mass6-Biron, J.; Mercier, J.; Adam, B.; PreTaut, Ch. Intensity'd'entrainement et aptitude ae"robie chez le sujet ag6. Science et Sports 5:137142; 1990. Masse"-Biron, J.; Mercier, J.; Collomp, K.; Hardy, J.; PreTaut, Ch. Age and training effects on lactate kinetics of master athletes during maximal exercise. Eur. J. Appl. Physiol. 65:311-315; 1992. Motoyama, M.; Sunami, Y.; Kinoshita, F; Irie, T.; Sasaki, J.; Arakawa, K.; Kinonaga, A.; Tanaka; H.; Shindo, M. The effects of long-term low intensity aerobic training on serum lipid and lipoprotein concentrations in elderly men and women. Eur. J. Appl. Physiol. 70:126-131; 1995. Patessio, A.; Casaburi, R.; Carone, M.; Appendini, L.; Donner, C ; Wasserman, K. Comparison of gas exchange, lactate and lactic acidosis thresholds in patients with chronic obstructive pulmonary disease. Am. Rev. Respir. Dis. 148:622-626; 1993. Pollock, M.; Dawson, G.; Miller, J.; Ward, A.; Cooper, D.; Headly, W.; Linnerud, A.; Nomeir, M. Physiologic responses of men 49 to 65 years of age to endurance training. J. Am. Geriatr. Soc. 24:97-104; 1976. Poulin, M.; Paterson, D.; Govindasamy, D.; Cunningham, D. Endurance training of older men: responses to submaximal exercise. J. Appl. Physiol. 73:452-457; 1992. Quantin, X.; Jolimoy-Boileau, G.; PreTaut, Ch. The relationship between dyspnea, gas exchange and lactate thresholds in patients with chronic obstructive lung disease. Personal communication, 1996. Seals, D.; Hagberg, J.; Hurley, B.; Ehsani, A.; Holloszy, J. Endurance training in older men and women: cardiovascular responses to exercise. J. Appl. Physiol. 57:1024-1029; 1984. Shephard, R. Le vieillissement et la performance physique. La Revue de Geriatrie 13:397-403; 1988. Sidney, K.; Shepard, R. Frequency and intensity of exercise as determinant of the response to training in elderly subjects. Med. Sci. Sports Exerc. 10:125-131; 1978. Takeshima, N.; Takana, K.; Kobayashi, F.; Watanabe, T.; Kato, T. Effects of aerobic exercise conditioning at intensities corresponding to lactate threshold in the elderly. Eur. J. Appl. Physiol. 67:138-143; 1993. Thomas, S.; Cunningham, D.; Thompson, J.; Rechnitzer, P. Exercise training and "ventilation threshold" in elderly. J. Appl. Physiol. 59:14721476; 1985. Vallet, G.; Varray, A.; Fontaine, J.L.; PreTaut, C. Inte're't du re"entramement a l'effort individualis6, au niveau du seuil ventilatorie, au cours de la bronchopneumopathie chronique obstructive de se've'rite' mode're'e. Rev. Mai. Resp. 11:493-501; 1994. Vallet, G.; Ahmaidi, S.; Serres, I.; Fabre, C ; Bourgouin, D.; Desplan, D.; Varray, A.; Pre"faut, Ch. Comparison of two training programmes in chronic airflow limitation patients: standardized versus individualized protocols. Eur. Resp. J. 10:114-122; 1997. Varray, A.; Mercier, J.; Terral, Cl.; PreTaut, Ch. Individualized aerobic and high intensity training for asthmatic children in an exercise readaptation program. Chest 99:579-586; 1991. Wasserman, K.; Whipp, B.; Koyal, S.; Beaver, W. Anaerobic threshold and respiratory gas exchange during exercise. J. Appl. Physiol. 35: 236-243; 1973. Yerg, J.; Seals, D.; Hagberg, J.; Holloszy, J. Effect of endurance exercise training on ventilatory function in older individuals. J. Appl. Physiol. 58:791-794; 1985. Received July 22, 1996 Accepted May 1, 1997