Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
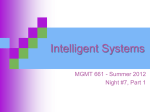
766 'White Coat' Hypertension No Harm for the Heart Philippe Gosse, Helene Promax, Philippe Durandet, Jacques Clementy Downloaded from http://hyper.ahajournals.org/ by guest on June 16, 2017 The superiority of ambulatory blood pressure monitoring over casual blood pressure measurement for the prediction of target-organ damage is now well established, although the significance of "white coat" hypertension is still controversial. Is an office blood pressure measurement that is higher than the mean ambulatory value an added risk? Because left ventricular hypertrophy is a potent risk factor, the effect of hypertension on left ventricular mass merits attention. Left ventricular mass indexed for height was measured by M-mode echocardiography in 204 essential hypertensive patients (140 males, 64 females; mean age [SD], SO [11] years). Blood pressure over 24 hours was monitored routinely with a noninvasive auscultatory device. Office blood pressure after 10 minutes of the subject in the supine position was measured by the same physician under the same conditions. The white coat effect was defined as the difference between the office and average daytime values of systolic and diastolic blood pressures. Patients were divided into four quartiles according to their office and daytime blood pressures. Two-way analysis of variance was used to assess the influence of the white coat effect at a given level of daytime blood pressure on left ventricular mass. Left ventricular mass increased significantly (P<.001) with daytime systolic blood pressure but was independent of white coat effect for both the whole population and the 143 untreated patients. We conclude that the white coat effect has no influence on left ventricular mass, favoring the view that white coat hypertension is a benign condition. (Hypertension. 1993;22:766-770.) KEY WORDS • blood pressure monitoring, ambulatory • hypertension, "white coat" • hypertrophy, left ventricular T he measurement of blood pressure by a physician may trigger a pressor response. This so-called white coat effect has a high interindividual variability1"3 and may explain, at least partially, the marked differences between office and ambulatory or self-measured blood pressure measurements. There is disagreement on the significance and prognostic implications of white coat hypertension. Some believe that the physicianinduced rise in blood pressure represents a marker of the patient's response to the stresses of everyday life, whereas others hold that the white coat effect is a benign conditioned response. It has been demonstrated that target-organ damage, especially left ventricular hypertrophy, is more closely correlated with ambulatory than office blood pressure. 47 In this study we addressed the following question: For a given level of ambulatory blood pressure, does a higher office blood pressure level have any influence on left ventricular mass? Methods Population All hypertensive individuals referred consecutively to our department by their general physicians over a 4-year period and fulfilling the following criteria were included: (1) casual blood pressure above 140/90 mm Hg on at least two occasions, (2) untreated or Received March 11, 1993; accepted in revised form June 23, 1993. From the Hopital Cardiologique, Pessac, France. Reprint requests to Dr Philippe Gosse, Hopital Cardiologique, CHU Bordeaux, Avenue de Magellan, 33604 Pessac, France. without treatment for more than 7 days, and (3) goodquality M-mode echocardiographic recordings of the left ventricle and 24-hour ambulatory blood pressure monitor records during their daily routine. Secondary causes of hypertension and coronary or valvular heart diseases were ruled out by clinical examination, electrocardiogram, and routine laboratory tests. Office Blood Pressure Measurement Office blood pressure was measured by the same physician under the same conditions. In the morning, after the subject had been supine for 10 minutes in the presence of the physician, three consecutive measurements were taken with a mercury sphygmomanometer (phase V for diastolic blood pressure). The mean of the three readings was noted. Ambulatory Blood Pressure Monitoring All recordings were performed with a Spacelabs 5200 auscultatory device and, more recently, a validated ECG-gated auscultatory device (DIASYS 200, Novacor).8 The monitor was placed on the left arm at the end of the consultation, and the blood pressure recording was checked by the physician on the right arm. Patients with differences of more than 15 mm Hg between the two arms were excluded. The monitor was programmed to measure blood pressure every 15 minutes from 6 AM to midnight and every 15 or 30 minutes at night. Recordings were taken during the patients' daily routine. No patient worked during the night. Recordings of pulse pressure below 15 mm Hg and diastolic blood pressure above 150 mm Hg were rejected, and record- Gosse el al ings were only included if at least 80% of the expected daytime measurements were available. Daytime was fixed arbitrarily as between 6 AM and 10 PM, and nighttime as between 10 PM and 6 AM. Average daytime and nighttime systolic and diastolic blood pressures were calculated. TABLE 1 . Echocardiography All echocardiograms were recorded by the same physician according to standard recommendations910 just before the office blood pressure determination. Briefly, M-mode recordings of the left ventricle guided by two-dimensional imaging were traced on a strip-chart recorder running at 100 mm/s. All recordings were coded and read blind by two observers according to the Penn convention. Left ventricular mass was calculated from Devereux's formula and was indexed for height. Downloaded from http://hyper.ahajournals.org/ by guest on June 16, 2017 Statistical Analysis Statistical analysis was carried out using PCSM software (Deltasoft, France). The white coat effect was defined as the difference between office and ambulatory daytime blood pressures and was calculated for both systolic and diastolic values. The Kolmogorov-Smirnov test was used to check that the parameters were distributed normally. Linear correlations were then calculated between (1) the white coat effect and age, weight, and office and ambulatory heart rates and (2) left ventricular mass and office and ambulatory blood pressures and white coat effect. We also carried out a linear stepwise multiple regression analysis. To assess the influence of the white coat effect for a given level of ambulatory daytime blood pressure, we divided patients into four quartiles according to their values of daytime blood pressure and four quartiles according to their values of white coat effect. The influence of white coat effect and daytime blood pressure on left ventricular mass was evaluated by two-way analysis of variance. Left ventricular mass, ambulatory blood pressure, and white coat effect were affected by age, which was therefore introduced as a covariate. Means were compared with the Newman-Keuls test when the analysis of variance showed significant differences or interaction. Systolic and diastolic blood pressures were analyzed separately. The results are presented as means with their corresponding standard deviations. Results Population Studied Two hundred and four patients were included in the analysis (140 males, 64 females; mean age, 50 [11] years; range, 16 to 74 years). Most of them (143) were untreated, and the others had been without treatment for an average of 3 months (7 days to 12 months). All patients were reported to have a blood pressure above 140/90 mm Hg on at least two occasions. The average office blood pressure at the time of the visit was 166 (18)/102 (10) mm Hg. Table 1 lists the main parameters for the population. The distributions of office and daytime blood pressures and of the white coat effect (shown in the Figure) were not significantly different from normal. White Coat Hypertension 767 Population Studied Mean SD Range 50 11 16-74 Office SBP, mm Hg 166 18 130-230 Office DBP, mm Hg 102 10 70-128 Daytime SBP, mm Hg 143 16 106-200 Daytime DBP, mm Hg 95 10 71-134 Systolic WCE, mm Hg 23 16 -11-75 9 -17-37 Parameter Age, y Diastolic WCE, mm Hg LVMI, g/m 6.5 140 38 57-284 SBP indicates systolic blood pressure; DBP, diastolic blood pressure; WCE, white coat effect; and LVMI, left ventricular mass index. Relations With White Coat Effect Age (r=.36, P<.01) and office heart rate (r=.17, F<.05) were positively correlated with the extent of the systolic white coat effect. Weight was negatively correlated with systolic white coat effect (r= — .24, P< .01). In the multivariate analysis, these three variables remained significantly correlated with systolic white coat effect but together accounted for only 18% of its variance. No significant relation was observed with diastolic white coat effect. There was a significant, albeit weak, correlation between systolic and diastolic white coat effects (r=.56, P<.Q\). Relations With Left Ventricular Mass Left ventricular mass index was more closely correlated with the daytime (r=.30, /><.001) than with the office (/'=.18, F<.01) systolic blood pressure. Coefficients of correlation with diastolic blood pressures were .18 (P<m) for daytime and .20 (/><.01) for office values. No significant correlation was observed with white coat effect. In the multivariate analysis, only the systolic daytime blood pressure was significantly and independently correlated with left ventricular mass. In the untreated population, the coefficient of correlation between left ventricular mass index and average daytime systolic blood pressure was .32 (P<.001). Relation of White Coat Effect With Left Ventricular Mass at a Given Level of Ambulatory Daytime Blood Pressure The whole population was divided in four quartiles according to their values of ambulatory daytime blood pressure and white coat effect. A white coat effect exceeding 22 mm Hg for systolic and 8 mm Hg for diastolic blood pressure was found in 50% of the population studied. Relation of White Coat Effect With Left Ventricular Mass at a Given Level of Systolic Blood Pressure The two-way analysis of variance identified a significant increase in left ventricular mass from the first to the fourth quartiles of daytime systolic blood pressure (P<.01) but no significant influence of white coat effect. As shown in Table 2, there was no constant elevation of left ventricular mass with white coat effect in each quartile of the daytime blood pressure. Introduction of age as a covariate did not affect the results of the 768 Hypertension Vol 22, No 5 November 1993 SYSTOLIC WHITE COAT EFFECT M (SD)=23 mm Hg (16) Bar graphs show distribution of white coat effect defined as the difference between office and average daytime blood pressures. M, mean. DIASTOLIC WHITE COAT EFFECT M (SD)=6.5 mm Hg (9) -17.«/-H.1 -7.B/-2.1 Downloaded from http://hyper.ahajournals.org/ by guest on June 16, 2017 analysis, and the same results were observed in an analysis restricted to the 143 untreated patients. Because the mean daytime blood pressure is affected by a variety of factors, such as the level of physical activity, the same analysis was carried out on the difference between office and nighttime systolic blood pressures used as a measure of the white coat effect. Seven patients for whom less than 80% of the required measurements were available were excluded from the analysis. The results of this additional analysis were similar to those of the initial analysis (Table 3). The two methods of estimating systolic white coat effect produced closely correlated results (r=.8O, P<.001). Relation of White Coat Effect With Left Ventricular Mass at a Given Level of Diastolic Blood Pressure The two-way analysis of variance of left ventricular mass index according to the quartiles of daytime diastolic blood pressure and diastolic white coat effect identified a significant interaction between the two factors (F<.001). Only one patient, who had a high left ventricular mass index, belonged to both the higher white coat effect quartile and the higher daytime blood pressure quartile. However, there was no consistent difference in left ventricular mass among the quartiles of the white coat effect in the Newman-Keuls test (see Table 4). Discussion Measurement of blood pressure by a physician generally produces higher values than those recorded by patients themselves at home. This consistent overestimate of blood pressure by the physician is not merely a reflection of the normal variations in blood pressure. In a study of continuous intra-arterial blood pressure recordings in the hospital, Mancia et al2 found that approach of a physician and recording of blood pressure from an arm cuff was accompanied by an abrupt rise in arterial pressure. Although this procedure gives a relatively rigorous estimate of the white coat effect, even with the use of noninvasive methods, it tends to be confined to a clinical research setting. Increasing use is TABLE 2. Left Ventricular Mass Index According to Daytime Systolic Blood Pressure and Systolic White Coat Effect Defined From Daytime Blood Pressure Daytime SBP Quartiles Systolic White Coat Effect Quartiles 1 2 (106-133 mmHg) (133.1-142 mmHg) 3 (142.1-152 mmHg) (152.1-200 mmHg) Mean Total 1 (-11-11 mmHg) 136(35) 149 (26) 136(41) 161 (38) 152(36) (n=5) (n=12) (n=9) (n=27) (n=53) 2 (11.1-22 mm Hg) 118(36) 123(32) 133(24) 159(34) 133 (32) (n=9) (n=9) (n=23) (n=8) (n=49) 3 (22.1-33 mm Hg) 116(29) 140(38) 146(33) 150(42) 137(36) (n=12) (n = 18) (n = 14) (n=6) (n=50) 4 (33.1-75 mmHg) 125 (30) 146(42) 186(36) 133 (59) 139 (44) (n=23) (n = 13) (n=6) (n=10) (n=52) 123(31) 141 (36) 144 (35) 154(43) (n=49) (n=52) (n=52) (n = 51) Mean total SBP indicates systolic blood pressure. Values are mean (SD) in grams per meter. 4 n=204 Gosse el al White Coat Hypertension 769 TABLE 3. Left Ventricular Mass Index According to Daytime Systolic Blood Pressure and Systolic White Coat Effect Defined From Nighttime Blood Pressure Daytime SBP Quartlles Systolic White Coat Effect Quartlles 1 (106-133 mmHg) 2 (133.1-142 mmHg) 3 (142.1-152 mmHg) 4 (152.1-200 mmHg) Mean Total 1 (-11-29 mm Hg) 130(40) 141 (38) 130(41) 174(35) 149 (41) (n = 5) (n=14) (n=10) (n=15) (n=44) 114(36) 146(28) 141 (31) 145 (38) 136(35) (n = 13) (n=11) (n=15) (n=14) (n=53) 123(20) 132 (33) 137(26) 145 (38) 135(31) (n=8) (n=16) (n=12) (n=13) (n=49) 125(32) 146(45) 159(31) 148(62) 141 (53) (n = 20) (n = 11) (n=12) (n=8) (n=51) 122(31) 141 (36) 142 (33) 154(43) (n=46) (n=52) (n=49) (n=50) 2 (29.1-41 mmHg) 3 (41.1-50 mmHg) 4 (50.1-112 mmHg) Mean total Downloaded from http://hyper.ahajournals.org/ by guest on June 16, 2017 n=197 SBP indicates systolic blood pressure. Values are mean (SD) in grams per meter. being made of ambulatory measurements and patient self-measurement to estimate the white coat effect, although the concordance between these results and the more rigorous procedure used by Mancia et al has yet to be established. In the present study, the white coat effect was evaluated from the difference between office blood pressure and the mean ambulatory value. We found an average value of 23 mm Hg for the systolic and 6 mm Hg for the diastolic white coat effect, with extremes of 75 and 37 mm Hg, respectively. These values are close to those reported by Mancia et al.2 Other studies have also noted the frequent overestimation of blood pressure when measured by a physician with respect to average daytime values.3 Ambulatory values are assumed to include the normal response to the stresses of everyday life provided that the recordings are made, as in the present study, during the patient's daily routine. However, the daytime ambulatory value is affected by a variety of factors (such as physical activity, emotions, duration of sleep), which may in turn affect the estimation of the white coat effect. Nevertheless, there appears to be a good reproducibility for the values of mean ambulatory blood pressure in different reported studies." We examined whether the difference between office and mean nighttime values would give a different estimate of the white coat effect. In fact, we found a high correlation between the two estimates (office-nighttime versus office-daytime). White coat hypertension is based on rather arbitrary criteria; therefore, in the absence of a clear definition of normal ambulatory blood pressure, it seems best to use daytime ambulatory values as a reference rather than nighttime or self-measured values, which are not affected by the stresses of everyday life. There is considerable individual variability in white coat effect, and it does not appear to bear any relation to clinical findings. We TABLE 4. Left Ventricular Mass Index According to Daytime Diastolic Blood Pressure and Diastollc White Coat Effect Defined From Daytime Blood Pressure Daytime DBP Quartlles 1 (71-89 mm Hg) 2 (89.1-95 mm Hg) 3 (95.1-102 mmHg) 4 (102.1-134 mmHg) Mean Total 1 (-17-0 mmHg) 132 (24) 145(25) 140(27) 148(36) 144(31) (n=6) (n = 11) (n = 13) (n=23) (n=53) 2 (0.1-8 mmHg) 138(13) 137 (42) 133(41) 134(36) 134(37) (n=4) (n = 11) (n = 20) (n = 18) (n = 53) 118(29) 147 (37) 125(24) 163(29) 143 (36) (n=51) Diastollc White Coat Effect Quartiles 3 (8.1-12 mmHg) 4 (12.1-37 mmHg) Mean total (n = 10) (n=22) (n=6) (n=13) 128 (31) 153(64) 153(21) 246 141 (47) (n=27) (n=15) (n=4) (n=1) (n=47) 127(29) 146(44) 136(33) 149(38) (n=47) (n=59) (n=43) (n=55) DBP indicates diastolic blood pressure. Values are mean (SD) in grams per meter. n=204 770 Hypertension Vol 22, No 5 November 1993 Downloaded from http://hyper.ahajournals.org/ by guest on June 16, 2017 noted only a weak correlation for the systolic value with age, office heart rate, and weight. Other studies have tended to produce conflicting results with low correlations.1213 Opinion is divided on the significance of the white coat effect.13 For some, it is an alarm response, and its extent is taken to be a marker of the patient's response to the stresses of everyday life. For others, the white coat effect is a conditioned response stemming from a defense reflex independent of true fluctuations in blood pressure and is an essentially benign phenomenon. Target-organ damage from hypertension appears to be better correlated with the ambulatory than the office value of blood pressure, although the prognostic significance of the ambulatory value remains to be established, the study of Perloff et al14 having to be confirmed on a prospective design. The risk from the white coat effect clearly needs to be assessed. In a survey of 737 young subjects in Tecumseh, Mich, with office and home self-monitored blood pressure values, Julius et al15 found a similar risk profile in "sustained" borderline hypertensive and white coat borderline hypertensive individuals as estimated from heart rate, systemic vascular resistance, minimal forearm vascular resistance, plasma triglycerides, and high-density lipoproteins. Nevertheless, the group with white coat hypertension still had a significantly higher home blood pressure than the normotensive group. The white coat effect therefore should be evaluated at strictly comparable levels of ambulatory or home blood pressure. Our results indicate that for a given level of ambulatory blood pressure, the white coat effect has no influence on left ventricular mass. In view of the high prognostic significance of an elevated left ventricular mass, our observations are in favor of a benign nature for the white coat effect. References 1. Mancia G, Bertinieri G, Grassi G, Parati G, Pomidossi G, Ferrari A, Gregorini L, Zanchetti A. Effects of blood pressure measurement by the doctor on patient's blood pressure and heart rate. Lancet. 1983;2:695-697. 2. Mancia G, Parati G, Pomidossi G, Grassi G, Casadei R, Zanchetti A. Alerting reaction and rise in blood pressure during measurement by physician and nurse. Hypertension. 1987;9:209-215. 3. Hoegholm A, Kristensen KS, Madsen NH, Svendsen TL. White coat hypertension diagnosed by 24h ambulatory monitoring. Am J Hypertens. 1992;5:64-70. 4. Devereux RB, Pickering TG, Harshfield GA, Kleinert HD, Dcnby L, Clark L, Pregibon D, Jason M, Kleiner B, Borer JS, Laragh JH. Left ventricular hypertrophy in patients with hypertension: importance of blood pressure response to regularly recurring stress. Circulation. 1983;68:470-476. 5. Gosse P, Campello G, Aouizerate E, Roudaut R, Broustet JP, Dallocchio M. Left ventricular hypertrophy in hypertension: correlations with rest, exercise and ambulatory systolic blood pressure. J Hypertens. 1986;4(suppl 5):S297-S299. 6. Pickering TG. Which measures of blood pressure give the best prediction of target organ damage and prognosis? In: Pickering TG. Ambulatory Monitoring and Blood Pressure Variability. London, England: Science Press; 1991:13.1-13.15. 7. Sokolow M, Werdegar D, Kain HK, Hinman AT. Relationship between level of blood pressure measured casually and by portable recorders and severity of complications in essential hypertension. Circulation. 1966;34:279-298. 8. O'Brien E, Mee F, Atkins N, O'Malley K. Accuracy of the Novacor DIASYS 200 determined by the British Hypertension Society protocol. J Hypertens. 1991;9:569-570. 9. Devereux RB, Reichek N. Echocardiographic determination of left ventricular mass in man: validation of the method. Circulation. 1977;5:613-618. 10. Gosse P, Roudaut R, Dallocchio M. Is echocardiography an adequate method to evaluate left ventricular hypertrophy regression? Eur Heart J. 1990;ll(supplG):107-112. 11. Pickering TG. Clinical aspects of ambulatory monitoring and determinants of normal ambulatory blood pressure. In: Pickering TG. Ambulatory Monitoring and Blood Pressure Variability. London, England: Science Press; 1991:9.1-9.15. 12. Lerman CE, Brody DS, Hui T, Lazaro C, Smith DG, Blum MJ. The white coat hypertension response: prevalence and predictors. J Gen Intern Med. 1989;4:225-231. 13. Pickering TG. Clinical measurement of blood pressure and white coat hypertension. In: Pickering TG. Ambulatory Monitoring and Blood Pressure Variability. London, England: Science Press; 1991: 7.1-7.14. 14. Perloff D, Sokolow M, Cowan R. The prognostic value of ambulatory blood pressures. JAMA. 1983;249:2792-2798. 15. Julius S, Mejia A, Jones K, Krause L, Schork N, Van de Ven C, Johnson E, Petrin J, Sekkarie MA, Kjeldsen SE, Schmouder R, Gupta R, Ferraro J, Nazzaro P, Weissfeld J. 'White coat' versus 'sustained' borderline hypertension in Tecumseh, Michigan. Hypertension. 1990;16:617-623. 'White coat' hypertension. No harm for the heart. P Gosse, H Promax, P Durandet and J Clementy Downloaded from http://hyper.ahajournals.org/ by guest on June 16, 2017 Hypertension. 1993;22:766-770 doi: 10.1161/01.HYP.22.5.766 Hypertension is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1993 American Heart Association, Inc. All rights reserved. Print ISSN: 0194-911X. Online ISSN: 1524-4563 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://hyper.ahajournals.org/content/22/5/766 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Hypertension can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Hypertension is online at: http://hyper.ahajournals.org//subscriptions/