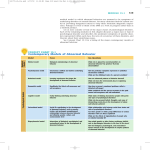
Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Abnormality in 1 hour Defining abnormality Definitions of Abnormality Defining a person or behaviour as ‘abnormal’ implies something undesirable and requiring change Therefore, we must be careful how we use the term Psychologists need methods for distinguishing ‘normal’ from ‘abnormal’ Our definition of abnormality must be objective: – It must not depend on anyone’s opinion or point of view – It should produce the same results whoever applies it It must not be under- or over-inclusive – It must not label as ‘abnormal’ or ‘normal’ behaviours or traits that aren’t Definitions of Abnormality Three definitions can be asked for in the examination: – Deviation from social norms – Failure to function adequately – Deviation from ideal mental health Deviation from Social Norms Under this definition, a person’s thinking or behaviour is classified as abnormal if it violates the (unwritten) rules about what is expected or acceptable behaviour in a particular social group. Their behaviour may: – Be incomprehensible to others – Make others feel threatened or uncomfortable With this definition, it is necessary to consider: – The degree to which a norm is violated, the importance of that norm and the value attached by the social group to different sorts of violation. – E.g. is the violation rude, eccentric, abnormal or criminal? Deviation from Social Norms: evaluation Social norms change between cultures and over time. Consequently, so do people’s conceptions of abnormality. – Homosexuality was regarded as a mental illness until 1973, but not any more. Cross-cultural misunderstandings are common, and may contribute to e.g. high diagnosis rate of schizophrenia amongst non-white British people. Classification of abnormality can only based on the context in which behaviour occurs – Same behaviour might be normal or abnormal e.g. undressing in bathroom or classroom – A subjective judgement is usually necessary e.g. there may be situational factors unknown to the observer Failure to Function Adequately Under this definition, a person is considered abnormal if they are unable to cope with the demands of everyday life. They may be unable to perform the behaviours necessary for day-to-day living e.g. self-care, hold down a job, interact meaningfully with others, make themselves understood etc. Rosenhan & Seligman (1989) suggest the following characteristics: – Suffering – Maladaptiveness (danger to self) – Vividness & unconventionality (stands out) – Unpredictability & loss of control – Irrationality/incomprehensibility – Causes observer discomfort – Violates moral/social standards Failure to Function Adequately: Evaluation Adequate functioning is defined largely by social norms and these norms change through time and culture. Most people fail to function adequately at some time, but are not considered ‘abnormal’ – After a bereavement most people find it difficult to cope normally. Ironically, they might actually be considered more abnormal if they functioned as usual Many people engage in behaviour that is maladaptive/ harmful or threatening to self, but we don’t class them as abnormal – Adrenaline sports – Smoking, drinking alcohol Deviation from Ideal Mental health Under this definition, rather than defining what is abnormal, we define what is normal/ideal and anything that deviates from this is regarded as abnormal This requires us to decide on the characteristics we consider necessary to mental health Deviation from Ideal Mental Health Psychologists vary, but usual characteristics include: – Positive view of the self – Capability for growth and development – Autonomy and independence – Accurate perception of reality – Positive friendships and relationships – Environmental mastery – able to meet the varying demands of day-to-day situations Deviation from Ideal Mental Health: Evaluation What is considered ideal is historically and culturally specific (see ‘deviation from social…’) Jahoda’s and others’ criteria set the bar too high. – Strictly applied, so few people actually meet these criteria that everyone ends up classed as abnormal and so the concept becomes meaningless Four approaches to explaining mental disorders. Psychological approaches Biological approach Psychodynamic approach Behavioural approach Cognitive approach For each approach you need... Assumptions Therapies • Explain the assumptions then link to mental disorders and give an example. • Describe and evaluate the therapies. • Does it work? • Is it accessible by everyone? • Ethical issues? Evaluation of the approach • What does it explain well? • What doesn’t it explain? • Does it offer effective therapies? • Does it raise any ethical issues? Biological approach Assumptions: – Abnormality is caused by physical processes. – Psychological disorders are illnesses or diseases affecting the nervous system – Abnormal behaviour, thinking and emotion are caused by biological dysfunctions – Understanding mental illness involves understanding what went wrong with the brain Biological causes of abnormality Brain damage • . Alzheimer’s disease is caused by degeneration of neurones. Chemical imbalances • Low level of serotonin (neurotransmitter) is associated with depression. Infections Genes • Clive wearing suffered from viral encephalitis which damaged his hippocampus as a result he could not form new memories. • Could code for abnormality in the structure and functioning of the brain i.e. schizophrenia shows a genetic pattern of inheritance. Biological approach: evaluation Uses scientific techniques to find evidence such as objective measurements like brain scans and blood tests so evidence is valid. Schizophrenia shows a genetic pattern of inheritance but environmental factors are also involved as the concordance rate in MZ twins is only 46% (should be 100% if it was only genetic). The changes observed in schizophrenics (enlarged ventricles) could be the effect rather than the cause of the disorder as the brain is a plastic organ which changes depending on the way we use it. More evaluation It does not take into account the early childhood experience which according to the psychodynamic approach could cause unconscious conflicts between the Id, the ego and superego which could cause abnormal behaviour in later life. The therapies proposed by the approach (drugs and ECT) are effective but they are not a cure, they only control the symptoms. It does not blame the patient but it disempowers them as they take a passive role in the treatment i.e. just take the medication prescribed by the professionals. Therapies: ECT Electro-convulsive therapy: Patient is relaxed with a sedative. Electrodes are attached to the temple. A voltage of 70 – 130 volts is passed through the brain for half a second. This produces a convulsion for 1 minute. Patient awakes and remembers nothing. 2 – 3 sessions a week for 3 – 4 weeks. Evaluating ECT Johnson stated that 11,000 procedures were carried out in the UK in 1999. Can be useful in suppressing depressive symptoms for up to one year. It is not known how it works. Can cause temporary memory loss and emotional side effects such as withdrawal and flatness. Does not deal with the problem and symptoms return usually after one year. Can cause death (4 in 100 000). Patients cannot give informed consent as they are in a distressed and confused state, given only when all other treatments have failed. Therapies: Drugs Antidepressants: i.e. Prozac, act by stopping the reuptake of the serotonin in the synaptic gap. Antipsychotic drugs: Block the dopamine receptors (dopamine is a neurotransmitter which is raised in schizophrenia). Drugs: evaluation Can be very effective and allow people to lead a normal life but they do not cure the disorder they only control the symptoms so when the drugs are stopped the symptoms reappear. They do not work for all patients, antipsychotic drugs work only for 50-60% of schizophrenic patients. They can have serious side-effects i.e. antidepressants can be very addictive. More evaluation.. They target the biological changes but do not change life circumstances, cognitive biases and daily stressors which might trigger mental disorders such as depression. They are a fairly cheap treatment and can act fairly quickly; they can be used to control the symptoms enough to allow the patient to start psychological therapies such as CBT or psychoanalysis. Psychodynamic approach: Assumptions: The tripartite structure of personality The earliest part of the human personality THE ID = the biological part (instincts & drives) Present at birth Motivated by the pleasure principle The second part of the human personality to develop THE EGO (the ‘self’) 1 - 3 years Motivated by the reality principle The third part of the human personality to develop THE SUPEREGO (the moral part) 3 - 5 years Motivated by the morality principle The Unconscious The conscious. The small amount of mental activity we know about. Thoughts Perceptions The preconscious. Things we could be aware of if we wanted or tried. The unconscious. Things we are unaware of and can not become aware of. Memories Stored knowledge Bad Worse Really Bad Fears Unacceptable sexual desires Violent motives Irrational wishes Immoral urges Selfish needs Shameful experiences Traumatic experiences Explanation of abnormal behaviour According to the psychodynamic approach abnormality is caused by unconscious conflicts between the Id, the superego and the ego. A consequence of these conflicts is anxiety. In order to protect itself against this the ego uses defence mechanisms i.e. repression, displacement, denial. If these defence mechanisms are unsuccessful this anxiety seep through to the conscious mind and creates mental disorders such as phobias. These conflicts originate mainly in early childhood while the child goes through the psychosexual stages of development. Schizophrenia is explained as a regression to the oral stage when the ego (which operates on the reality principle) is developing and the Id is dominant. The weak ego explains the lack of grasp of reality in schizophrenics. Anorexia is explained by repressing fear of sexual activities, by not eating the girls aim at retaining their child physic thus avoiding sexualisation. Evaluation This theory is almost impossible to test scientifically and the support for the theory consist mainly of case studies carried out on upperclass Austrian women, the sample does not represent the wider population therefore the results cannot be generalised. They are not replicable so the results are not reliable. They are high in ecological validity the patients were real people in a real therapeutic situations. The interpretation of the data was done by Freud so it might have been biased. This theory was the first theory which took into account the childhood experiences as a possible cause of mental disorders. This approach was the first to propose a “talking” cure which changed the way mental patients were treated. It does not explain the biological factors such as enlarged ventricles in schizophrenics but they could be the effect rather than the cause of the disorder as the brain is a plastic organ which changes depending on the way we use it. Therapy Psychoanalysis: its aim is to bring the unconscious conflicts to the conscious mind where they can be dealt with. It uses two main strategies 1. Free association: Client is asked to talk about anything that comes to mind and the therapist writes this down and then later analysis the content to reveal repressed desires. The client is made aware of this to then overcome them. 2. Dream analysis: Client is asked to talk about dreams (manifest content) the therapist then interprets the hidden meaning (latent content) and makes client aware of this so they can overcome repressed issues Evaluation Uses retrospective data (from childhood), this can be inaccurate because people might have forgotten and it can be distorted by schemas. It may take a long time; sometimes years so is not appropriate in cases when urgent intervention is required (i.e. suicidal patients). It is very expensive and rarely available in its original form on the NHS, this limits access. People with mental disorders such as schizophrenia might not have the necessary insight to take part in the treatment. Can be very unethical to bring up repressed memories as they can be painful. Behavioural approach Assumptions: Abnormal behaviour like any other behaviour is learned from the environment. Behaviour can be learned in 3 ways: 1. Classical conditioning: learning by association i.e. phobia UCS: bite UCR: fear NS: dog, pairing dog and bite, dog becomes the CS, CR: fear (phobia: the dog elicits the fear response). 2. Operant conditioning: learning by consequences i.e. depression. A person displays depressed behaviour others shows sympathy (positive reinforcement) and are likely to let them off their normal duties (negative reinforcement) so the behaviour will be repeated as it has been reinforced. 3. Social learning: learning by imitation i.e. anorexia. Young girls see very thin models being praised and getting attention and money (reinforcements) they try to get as thin as these models to get the same reinforcements. Classical conditioning: Learning a phobia Rat: NS Noise: UCS) BANG Pairing Fear: UCR Rat: NS Noise: UCS) BANG Fear: UCR After conditioning Rat: CS Fear: CR Evaluation of the behavioural approach This approach can offer satisfactory explanations for some disorders such as phobias and eating disorders. However many people have phobias of objects they have never met (i.e. snakes) these cannot be explained by classical conditioning. These could be due to evolution. It does not explain the biological factors such as enlarged ventricles in schizophrenics but they could be the effect rather than the cause of the disorder as the brain is a plastic organ which changes depending on the way we use it. More evaluation.... It does not take into account the early childhood experience which according to the psychodynamic approach could cause unconscious conflicts between the Id, the ego and superego which could cause abnormal behaviour in later life. Treatments based on the behavioural approach such as systematic desensitisation can be very effective for disorders such as phobias. It does not take into account cognitive factors such as cognitive biases i.e. even when severely underweighted, anorexic see themselves as overweight. Therapies As the assumption of the behavioural approach is that abnormal behaviour is learned, the aim of the therapies it proposes is to “unlearn” the abnormal behaviour and replace it by a normal behaviour. Systematic desensitisation aims at “unlearning” the association between the phobic abject and fear to replace it by a new association between the object and a state of relaxation. Systematic desensitisation It is a step by step approach The client learns relaxation techniques The client works out a hierarchy of fear from the least frightening to the most frightening Fur Paw Mouth Dog The client works through the hierarchy learning to use relaxation techniques in the presence of the feared object Evaluation It can be very effective in the treatment of some phobias (6090% for spider phobias) but it does not seem so effective with social phobias or phobias of objects or situations which relate to evolution. Once the phobia is improved it may be replace by another phobia or another form of anxiety disorder which suggests that phobias might have a deeper psychological cause. It is an expensive treatment as it is carried out by a qualified clinical psychologist so it is not accessible to everybody. It requires 6-8 sessions for moderate phobias, more for strong phobias so it requires commitment from the patient. It does not address psychological factors for example the psychodynamic approach argues that phobias are due to an unconscious conflict and the phobic object is a symbol of the real object of fear. Basic assumptions Emotional problems can be attributed directly to distortions (maladaptive thoughts) in our thinking processes. These maladaptive thoughts usually take place automatically and without full awareness. Examples of Cognitive Biases that may be used by people with Depression Cognitive Bias Explanation Minimisation The bias towards minimising success in life. Maximisation The bias towards maximising the importance of even trivial failures. Selective Abstraction A bias towards focusing on only the negative aspects of life and ignoring the wider picture All or nothing Thinking A tendency to see life in terms of black and white and ignoring the middle ground; you are a success or a failure, rather than not good at some things but OK at others. Ellis’s ABC Model Activating events (A) have consequences (C) which are affected by beliefs It is not the event which (B). creates the problem, it is the way you think about it An example... Sally and Clive split up Beliefs Rational thoughts “we were not compatible” Activating event Irrational thoughts “It’s my fault, nobody can ever love me, all my relationships will fail” Consequences Desirable emotions “ I am sad but next time it will work out” Desirable behaviour “ I have learned from this, Lets go out” Undesirable emotions “ I feel so guilty, I am unlovable” Undesirable behaviour “ I’ll never have another relationship. It hurts too much” Evaluating the cognitive approach as an explanation of abnormality It does not take into account biological factors such as enlarged ventricles in schizophrenics (but...)or genetic factors. It suggests that it is the patient who is at fault rather than the situation in which they are. A disorder such as depression can change the way we think so the faulty thinking might be the effect rather than the cause of the disorder More evaluation It does not account for the cause of the faulty thinking (i.e. early childhood experiences) Some irrational beliefs are quite realistic (Alloy & Abrahmson, 1979) There is clear evidence for cognitive biases and dysfunctional thinking and beliefs in disorders such as depression and anxiety disorders. Let summarise.... Negative schemata about the self, the world and the future So what should the therapist target? Cognitive bias Rational-Emotive-Behaviour Therapy (a form of CBT) Helps the patient identify the maladaptive thoughts and the consequences of thinking in this way disputes the beliefs and tries to show The therapist disputes that they are not true i.e. the client does not always fail in all relationships The client and the therapist set goals to think in a more adaptive way i.e. focus on the client’s success and trying to build on those. The treatment focuses on the present situation, looking back to the past only when it can be useful i.e. to learn from it Logical disputing: Does it make sense? Empirical disputing: Is it consistent with reality? Pragmatic disputing: Is this belief/attitude helpful in the client’s life? Evaluation of the REBT Suitable for treating a wide range of mental disorder Gives the individual responsibility for their treatment Less time consuming than psychoanalysis but how does it compare with the biological approach therapies? Evidence to support CBT use for depression Is it accessible to everyone? Ethics?