Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
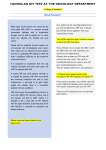
reviews Annals of Oncology 26. Pettengell R, Schmitz N, Gisselbrecht C et al. Rituximab purging and/or maintenance in patients undergoing autologous transplantation for relapsed follicular lymphoma: a prospective randomized trial from the lymphoma working party of the European Group for Blood and Marrow Transplantation. J Clin Oncol 2013; 31(13): 1624–1630. 27. Vidal L, Gafter-Gvili A, Salles G et al. Rituximab maintenance for the treatment of patients with follicular lymphoma: an updated systematic review and meta-analysis of randomized trials. J Natl Cancer Inst 2011; 103(23): 1799–1806. 28. Gisselbrecht C, Schmitz N, Mounier N et al. Rituximab maintenance therapy after autologous stem-cell transplantation in patients with relapsed CD20(+) diffuse large B-cell lymphoma: final analysis of the collaborative trial in relapsed aggressive lymphoma. J Clin Oncol 2012; 30(36): 4462–4469. 29. Muller C, Murawski N, Wiesen MH et al. The role of sex and weight on rituximab clearance and serum elimination half-life in elderly patients with DLBCL. Blood 2012; 119(14): 3276–3284. Annals of Oncology 27: 397–408, 2016 doi:10.1093/annonc/mdv606 Published online 17 December 2015 Non-AIDS-related malignancies: expert consensus review and practical applications from the multidisciplinary CANCERVIH Working Group J.-P. Spano1,2,3*, †, I. Poizot-Martin4,5,†, D. Costagliola2,3, F. Boué6,7, O. Rosmorduc8,9, A. Lavolé10, S. Choquet2,3,11, P.-E. Heudel12, V. Leblond8,11,13, J. Gabarre11, M.-A. Valantin2,3,14, C. Solas15, A. Guihot8,16, G. Carcelain8,13, B. Autran8,13, C. Katlama2,3,14 & L. Quéro17,18 1 Department of Medical Oncology, Groupe hospitalier Pitié-Salpêtrière-Charles Foix, AP-HP, Paris; 2INSERM, UMR_S 1136, Institut Pierre Louis d’Epidémiologie et de Santé publique, Paris; 3Pierre Louis Institute of Epidemiology and Public Health, Sorbonne Universités, UPMC Université Paris 06, Paris; 4Clinical Immunohaematology Service, Université Aix-Marseille, AP-HM Sainte-Marguerite, Marseille; 5INSERM, U912 (SESSTIM), Marseille; 6Department of Internal Medicine and Immunology, Hôpital Antoine Béclère, Clamart; 7Faculty of Medicine, Université Paris-Sud, Le Kremlin-Bicêtre; 8Faculty of Medicine, Sorbonne Universités, UMPC Université Paris 06, Paris; 9 Hepatology Service, Hôpital Saint-Antoine, Paris; 10Pneumology Service, Hôpital Tenon, Paris; 11Department of Hematology, Groupe hospitalier Pitié-Salpêtrière-Charles Foix, Paris; 12Medical Oncology Service, Centre Léon Bérard, Lyon; 13Centre for Research in Immunology and Infectious Diseases, Sorbonne Universités, UPMC Université Paris 06, Paris; 14Department of Infectious Diseases, Groupe hospitalier Pitié-Salpêtrière-Charles Foix, Paris; 15Laboratory of Pharmacokinetics and Toxicology, Hôpital de La Timone, Marseille; 16Department of Immunology, Groupe hospitalier Pitié-Salpêtrière-Charles Foix, Paris; 17Department of Oncology and Radiotherapy, Hôpital Saint Louis, Paris; 18INSERM UMR_S 965, Université Paris Denis Diderot, Paris, France Received 10 June 2015; revised 26 October 2015 and 29 November 2015; accepted 1 December 2015 Malignancies represent a major cause of morbidity and mortality in human immunodeficiency virus (HIV)-infected patients. The introduction of combined antiretroviral therapy has modified the spectrum of malignancies in HIV infection with a decreased incidence of acquired immunodeficiency syndrome (AIDS) malignancies such as Kaposi’s sarcoma and nonHodgkin’s lymphoma due to partial immune recovery and an increase in non-AIDS-defining malignancies due to prolonged survival. Management of HIV-infected patients with cancer requires a multidisciplinary approach, involving both oncologists and HIV physicians to optimally manage both diseases and drug interactions between anticancer and antiHIV drugs. The French CANCERVIH group presents here a review and an experience of managing non-AIDS malignancies in HIV-infected individuals. Key words: cancer, AIDS, HIV, treatment, review introduction The CANCERVIH working group is a national French multidisciplinary network dedicated to human immunodeficiency virus *Correspondence to: Prof. Jean Philippe Spano, Department of Medical Oncology, PitieSalpetriere Hospital, 47 bld l’hopital, Paris 75013, France. Tel: +33-1-42-16-04-72; Fax: +33-1-42-16-04-69; E-mail: [email protected] † Both authors contributed equally to the work. (HIV)-infected patients with cancer and funded by the French National Cancer Institute (INCa). The backbone of this network is based upon the creation of a multidisciplinary national board, namely CANCERVIH, which is closely associated with local or regional-specific multidisciplinary board from every center participating in this working group. The national CANCERVIH is constituted by experts, and also for some of them, more specifically specialized in AIDS and non-AIDS malignancies. Since May 2014, the role of this unique © The Author 2015. Published by Oxford University Press on behalf of the European Society for Medical Oncology. All rights reserved. For permissions, please email: [email protected]. reviews national board CANCERVIH is to analyze and to propose therapeutic strategy for HIV-positive patients with malignancies during bimonthly national web conference. Each CANCERVIH expert carried out a systematic literature review of non-AIDS-related malignancies using the Medline database (from January 1990 to October 2015). Each expert of the working group independently evaluated publications and submitted preliminary recommendations to the CANCERVIH expert panel. Each preliminary recommendation was then discussed within the CANCERVIH group and adopted by qualified majority. One of the most recent and significant recommendation approved in France was to propose a systematic HIV screening test for all new cases of malignancies in patients from the general population, mentioned in the Morlat report [1]. Malignancies have always been a major feature of HIV/AIDS from the start of the epidemics in the early 1980s with the emergence of Kaposi’s sarcoma (KS) in young gay men with an unusual immune deficiency later called Acquired Immune Deficiency Syndrome (AIDS) to the large pandemics of current times. While AIDS-related cancers—mostly virally induced such as Kaposi’s sarcoma (KS), associated with HHV8, cervical cancer associated with oncogenic human papillomavirus (HPV) types [2–4] and non-Hodgkin lymphoma (NHL) associated with Epstein Barr virus (EBV) in ∼30% of diffuse large B-cell lymphoma [5–7] and 50% of Burkitt lymphoma—still represent a major cause of mortality and morbidity in late presenters worldwide, combined antiretroviral therapy enabling durable control of viral replication has led to increased life expectancy with malignancies therefore taking a longer time to develop. Indeed, currently, all HIV-infected patients are likely to receive combination anti-retroviral therapy (cART) irrespective of their CD4 cell count. Lastly, due to multiple factors, the incidence of non-AIDS-defining cancers in such patients is two to three times more frequent than in the general population [8–10]. Several guidelines and reviews have already been published for HIVinfected patients with cancer [11], cervical cancer [12], KS [13], malignant lymphoma [14] and for chemotherapy in HIV-infected patients [15]. The objective of this article was to provide an update on current therapeutic approaches for the main non-AIDS-related malignancies with a particular focus on drug–drug interactions. epidemiology and risk factors Cancer is a frequent comorbidity in HIV-infected individuals and in 2010, represented 34% of the causes of death in France [2]. In a meta-analysis of studies conducted in the cART era [9], the relative risks compared with the general population differ widely according to cancer type, the highest being for anal cancer (47) and Hodgkin’s lymphoma (HL) (19) with lung cancer much lower (3.5), whereas the relative risk for liver cancer depends a lot on the frequency of HCV co-infection; these four cancers are the most frequent non-AIDS-defining cancers in HIV-infected individuals. Interestingly, the relative risks for breast and prostate cancer, two hormone-dependent cancers, were <1 (0.6 for both) in the same meta-analysis. After adjusting for the difference in age distribution between individuals with AIDS or HIV infection and the general population, Shiels et al. showed that the differences in median age at diagnosis were modest and most were not significant [16], | Spano et al. Annals of Oncology whereas Hleyhel et al. also found modest differences except for liver cancer in HBV or HCV co-infected individuals (11 years younger) [17], dismissing the hypothesis of general accelerated aging in HIV-infected individuals [18, 19]. Recent papers on the risk of anal cancer in HIV-infected individuals show an increased risk in the cART era compared with the pre-cART era [20–22]. This is consistent with the finding that duration of immunodeficiency and not current CD4 cell count level is a risk factor for anal cancer [23]. Palefsky and Holly [24] have posited that immune suppression affects earlier stages of HPV-related intraepithelial neoplasia, but plays a small role in progression to invasive cancer. The risk of HL, lung and liver cancers is also elevated in organ transplant recipients [8], and immunodeficiency is a risk factor for these cancers, even when accounting for tobacco exposure for lung cancer or HBV/HCV status for liver cancer [23, 25]. Lung cancer is the only frequent cancer in HIV-infected patients not known to be associated with viral infection and the proportion of smokers is higher in HIV-infected individuals than in the general population. Several studies have suggested that HIV infection is associated with the risk of lung cancer even after adjusting for cigarette smoking [26–28], although Helleberg et al. have shown that nonsmoking HIV patients did not have increased risk of nonvirological cancers compared with nonsmoking controls [29]. Persistent inflammation and activation, commonly described in HIV patients even with controlled viral load under cART, have been shown to increase the risk of lung cancer in non-HIVinfected individuals [30]. In addition, smoking may act synergistically on HIV infection to increase immune activation and therefore the risk of lung cancer in smoking HIV-infected individuals [31]. Finally, given the link between the different cancers and immunodeficiency, one may expect a lower risk in treated patients with recovered immunity (CD4 cell count >500/µl) or who initiate cART with maintained CD4 levels. However, in Silverberg et al. paper, the relative risks in HIV-infected patients with a current CD4 cell count >500/µl compared with non-HIVinfected individuals was still highly significant for anal cancer (34) and HL (13.5), but no higher for lung (1.2) and liver cancer (1.0) [25]. In the FHDH ANRS CO4, the relative risk in HIVinfected individuals with a CD4 cell count >500/µl for at least 2 years and a controlled viral load was still elevated relative to the general population for HL (9.4) and liver cancer (2.4) but no higher for lung cancer (0.9) [17]. The new WHO guidelines recommending initiation of cART regardless of CD4 cell count should therefore result in decreasing excess risk in the future for the most frequent non-AIDS-defining cancers except for anal cancer in individuals diagnosed with a low CD4 cell count [32]. nonsmall-cell lung cancer diagnosis The high prevalence of smoking in the HIV-infected population is a primary contributor to the increased risk of nonsmall-cell lung cancer (NSCLC) compared with the general population [29, 33] and treatment of tobacco abuse is highly recommended [34]. NSCLC represents 86%–94% of HIV lung cancer cases as in the general population and adenocarcinoma is the most common Volume 27 | No. 3 | March 2016 reviews Annals of Oncology histological type [35]. The incidence of epidermal growth factor receptor (EGFR) mutations and anaplastic lymphoma kinase (ALK) rearrangement in HIV NSCLC is not known. However, a low prevalence is expected according to the demographic characteristics of the HIV–NSCLC population. Indeed, such mutations are observed more frequently in nonsmokers in the general population. Most HIV-infected patients with lung cancer often present common features at diagnosis, such as respiratory signs and several symptoms due to advanced stage. prognosis The reasons for poorer prognosis in HIV–NSCLC cases compared with the general population remain unclear [36–40]. A large recent study based on cancer registry in the United States showed that 1058 HIV-infected patients with LC experienced higher cancerspecific mortality compared with 327 866 non-HIV-infected patients with LC even after stratification on stage and treatment [hazard ratio (HR), 1.28; 95% confidence interval (CI) 1.14–0.144], suggesting a role played by persistent immunodepression [41]. However, from 2001 to 2004 in France, the 5-year survival rate in HIV-infected patients with lung carcinoma (LC) was similar compared with the general population (17%versus 17%) [42]. management The therapeutic recommendations are based on NSCLC clinical practice guidelines in the general population [43, 44]. Surgery should be the treatment of choice in early-stage disease. Patients with locally advanced disease should be offered chemoradiotherapy. In first-line metastatic disease, patients should be screened for EGFR mutations and ALK rearrangement. In the absence of an oncogenic driver, standard chemotherapy regimens are indicated, with particular attention to drug interactions [45, 46]. Prospective studies should be strongly encouraged. In July 2015, the IFCT (Francophone Thoracic Cancerology Intergroup) completed a phase II, multicenter study dedicated to HIV NSCLC evaluating carboplatin and pemetrexed (NCT01296113 clinical Trials.gov). The National Cancer Institute (NCI) promotes a phase I Pharmacokinetic Study of Erlotinib for advanced NSCLC in persons with HIV Infection (NCT02134886 clinicalTrials.gov). Preclinical in vivo assessment showed that CYP3A4 inhibitors alter the exposure of erlotinib: ritonavir resulted in a 3.0-fold increase in erlotinib area under curve [47]. Consequently, pending the results of the NCT02134886 trial, erlotinib should be used with caution in patients on a ritonavir-containing antiretroviral regimen. For second-line treatment in advanced disease, two phase III trials have demonstrated an improvement in overall survival in the general population with immune checkpoint inhibitors (nivolumab) compared with docetaxel with a better toxicity profile (respectively, 9.2 versus 6 months, HR, 0.59; 95% CI 0.44–0.79 for squamous NSCLC and 12.2 versus 9.4 months, HR 0.73; 96% CI 0.59–0.89 for nonsquamous NSCLC) [48, 49]. The efficacy and safety of such novel therapy have to be proven in HIV-NSCLC. One phase I study of ipilimumab plus nivolumab in advanced HIV-associated solid tumors is currently recruiting (NCT02408861 clinicalTrials.gov). Given the potential impact of such novel therapies on HIV infection, there is an urgent need for prospective studies. Volume 27 | No. 3 | March 2016 screening In the general population, the randomized National Lung Screening Trial showed a significant 20% lung cancer mortality reduction and a 6.7% overall mortality reduction in current or heavy smokers aged 55–74 years (with at least a 30-pack-peryear smoking history) undergoing three annual low-dose computed tomography (CT) chest scans versus radiography [50]. A recent study, the ANRS EP48 HIV CHEST, demonstrated that chest CT was a safe and effective procedure to detect lung cancers, most of them at early stages, in HIV-infected heavy smokers [51]. However, another lung cancer screening trial of 224 HIV-infected current/former smokers were not convincing, given that, in this study, only one lung cancer was detected in 678 patient years [52]. Finally, there is insufficient evidence to recommend NSCLC screening with low-dose CT in asymptomatic persons. hepatocellular carcinoma diagnosis Between 1996 and 2009, there was an increase in the proportion of in-care HIV-infected patients with cirrhosis, decompensated cirrhosis and hepatocellular carcinoma (HCC). The risk factors associated with a higher likelihood of cirrhosis and HCC in HIV-infected patients were hepatitis B virus (HBV), hepatitis C virus (HCV), age, diabetes, low CD4+, alcohol abuse, Hispanic ethnicity. [53]. In addition, those who did not undergo a screening program exhibited more advanced tumor stage and liver failure or cirrhosis decompensation than those diagnosed through screening [53, 54]. Therefore, active HCC-screening programs in the HIV-infected patients may lead to better survival (61% versus 15% at 36 months) [54]. British HIV Association, European Association for Study of the Liver (EASL), European Society for Medical Oncology (ESMO) and American Association for the Study of Liver Disease (AASLD) guidelines recommend screening for patients with hepatitis and HIV co-infection [55–58]. Strength of recommendation regarding active HCC-screening programs is 1B according to grade system [56]. While achievement of a sustained viral response in HCV-infected patients is associated with a low risk of developing clinical decompensation, the risk of developing an HCC is not fully abrogated but is attenuated by 50%–75% following HCV clearance. The new interferon-free anti-HCV regimens with short treatment duration and fewer side-effects, available in both HCV-infected and co-infected patients from 2015, should similarly decrease the HCC risk in these patients. treatment curative treatment. According to the Barcelona Clinic Liver Cancer (BCLC) staging system, liver transplantation (LT), resection or radiofrequency ablation are recommended as early HCC treatment options (Figure 1) [54, 56]. LT should be considered in patients with a solitary lesion of <5 cm or three nodules <3 cm (Milan Criteria) that are not suitable for resection. HCC represents a growing indication for the requirement of LT in HIV-infected patients who fulfill these criteria [59–62]. When a long waiting time (>6 months) for LT is anticipated, patients may be offered additional liver resection, local ablation doi:10.1093/annonc/mdv606 | reviews Annals of Oncology HCC Stage 0 PS 0, child-pugh A Very early stage 1 HCC <2 cm Carcinoma in situ 1 nodule Portal pressure /bilirubin No Resection Stage A-C PS 0–2, child-pugh A-B Intermediate stage B Multinodular PS 0 Early stage A 1 HCC or 3 nodules <3 cm, PS 0 Stage A-C PS >2, child-pugh C Advanced stage C Portal invasion N1,M1; PS 1–2 Terminal stage D 3 nodules £ 3 cm Chemo embolization Yes Sorafenib Supportive care Associated diseases No Yes Liver transplantation PEI/ RF PEI: percutaneous ethanol injection; RF: radiofrequence; PS: performance status; HCC: hepatocellular carcinoma Figure 1. Curative and palliative treatment assignment of hepatocellular carcinoma (HCC) according to the Barcelona Clinic Liver Cancer (BCLC) staging system (adapted from a previous study [56]). Table 1. Immunological and virological criteria necessary for considering liver transplant in HIV-related patients (adapted from Nunnari et al. [64]) Immunological criteria No AIDS-defined opportunistic infections within the previous year CD4 cell count >200 cells/μl or >100 cells/μl in cases of therapy intolerance Virological criteria • Undetectable HIV viral load (<50 copies/ml) in the last 12 months or effective therapeutic options for HIV infection during the posttransplant period • • AIDS, acquired immunodeficiency immunodeficiency virus. syndrome; HIV, human using radiofrequency or chemoembolization (see infra) in order to minimize the risk of tumor progression. The results of a case– control study on HCC patients who were scheduled for an LT (21 HIV-infected patients and 65 non-HIV-infected controls) demonstrated that there was a trend toward a higher dropout rate among HIV-infected patients compared with non-HIVinfected ones (23% versus 10%) on a waiting list for an LT, despite both groups exhibiting similar initial tumor stages [63]. OS following LT at 1 and 3 years reached 81% and 74% in HIVinfected patients, compared with 93% and 85% in non-HIVinfected, respectively (P = 0.08). Due to the higher dropout rate | Spano et al. among the HIV-infected patients, HIV infection may therefore impair the results of LTs for HCC on an intent-to-treat basis, though it was found to have no significant impact on OS or relapse-free survival after LT. Conversely, there were no differences observed in HCC recurrence (7% versus 14%, respectively) or survival rates (65% versus 70% at 3 years) between the 30 HIV-infected patients and the 125 non-HIV-infected controls who underwent LT for HCC [61]. The criteria for considering LT in HIV-infected patients have recently been outlined and are similar to those applied to non-HIV-infected patients, except for those with specific immunological and virological features (Table 1) [64]. noncurative treatment. For HIV-infected patients, candidates for transarterial chemoembolization include those with either Child–Pugh A or B liver function and those with BCLCclassified intermediate stage B HCC, including patients with unresectable, multinodular or large tumors (as recommended for non-HIV-infected patients) (Figure 1). A more aggressive clinical course of HCC was evidenced in an HIV/HCV-co-infected group, defined as exhibiting shorter survival time. In a recent multivariate analysis, α-fetoprotein level, Child–Pugh C classification, and the size of the largest nodule emerged as independent prognostic factors, while HIV status was not associated with survival [65]. Owing to the absence of large randomized trials, it is difficult to confirm the efficacy and tolerance of the reference treatment, sorafenib, in HIV-infected patients undergoing HAART. However, Volume 27 | No. 3 | March 2016 reviews Annals of Oncology a recent study involving 27 patients reported a median OS of 12.8 months and time to progression of 5.1 months with this combination, similar to the findings reported in the pivotal SHARP study. The same applied to the tolerance (Grade 3–4 adverse event) observed: diarrhea 14.8%; hypertension 11%; hand–foot skin reaction 14.9%; all of which suggest that this treatment may also benefit HIV-infected patients. However, most HIV-infected patients are excluded from clinical trials, partly due to the risk of potential drug interactions and side-effects [66, 67]. screening Surveillance of patients at risk for HCC should be carried out by abdominal ultrasound every 6 months. Noninvasive diagnosis of HCC (i.e. without liver biopsy) is only possible in cirrhotic patients and requires state-of-the-art imaging techniques (multiple-phase multidetector CT scan and/or dynamic contrastenhanced MRI), with identification of the typical vascular hallmark of HCC (hypervascular in the arterial phase with washout in the portal venous or delayed phases). anal cancer diagnosis HIV-infected patients with anal carcinoma are younger than non-HIV-infected patients with a median age at diagnosis of 45 versus 60 years, respectively. A majority of HIV-infected patients with anal cancer are men and most of them have sex with men [68]. The prevalence of HPV infection is ∼90% in HIV-infected patients with anal cancer [69, 70]. In the EDITH V study, Abramowitz et al. reported that HIV-infected patients had a higher proportion of multiple HPV infection than non-HIVinfected patients with an under-representation of the HPV16 genotype. The proportion of multiple HPV infections was significantly higher among HIV-infected than among non-HIVinfected patients (56.0% versus 19.6%, respectively) [69]. Anal intraepithelial neoplasia (AIN) of all grades affects ∼70%–80% of HIV-infected men who have sex with men, with high-grade intraepithelial neoplasia in 25%–50% [71, 72]. In this population, disease progression rates from high-grade intraepithelial neoplasia to invasive anal cancer have been reported to be ∼15% [73]. prognosis Several retrospective studies have reported overall 5-year survival of 62%–67% after chemoradiotherapy in HIV-infected patients which is comparable with the rate for HIV-uninfected patients (Table 2). However, some studies have reported highlocal recurrence rates (30–60%) and low sphincter preservation in HIV-infected patients in comparison with HIV-uninfected patients (25%–30%). This higher local recurrence rate observed in some studies may be due to lower tolerance of chemoradiotherapy among HIV-infected patients resulting in prolonged overall treatment time compared with HIV-uninfected patients [77]. treatment The treatment of anal cancer in HIV-infected patients does not differ from non-HIV-infected patients. Table 2. Results from studies of anal cancer in HIV-infected patients treated during cART era Authors Date of publication Patients (n) Treatment Median follow-up (months) Cleator et al. [74] 2000 12 58 Stadler et al. [75] 2004 8 Wexler et al. [76] 2008 32 Oehler-Janne et al. [77] 2008 40 Seo et al. [78] 2009 10 Hogg et al. [79] 2009 21 Abramowitz [80] 2010 44 Fraunholz et al. [81] 2010 21 Munoz-Bongrand et al. [82] 2011 20 RCT 5-FU/MMC RCT 5-FU/CDDP RCT 5-FU MMC or CDDP RCT 5-FU MMC or CDDP RCT 5-FU/MMC RCT 5-FU/MMC RCT 5-FU/CDDP RCT 5-FU/MMC RCT 5-FU/CDDP Local control rate Overall survival rate 82% 64% 24 50% 75% 35 91% 84% 60% (5 years) 67% (3 years) 65% (5 years) 36 92% 38% 61% (5 years) 100% 94% 37 81% 71% 27 82% 87% 53 81% 59% 32.5 70% 50% 92% (3 years) 73% (3 years) 85% (3 years) 67% (5 years) 39% (5 years) 37.2 Clinical complete response rate RCT, radiochemotherapy; 5-FU, 5-fluorouracil; CDDP, cisplatin; MMC, mitomycin C. Volume 27 | No. 3 | March 2016 doi:10.1093/annonc/mdv606 | reviews Whenever possible, management of patients is recommended in centers with both specific expertise and a multidisciplinary approach, in order to provide optimal care [11, 83]. For localized anal cancer (tumor size ≤2 cm without lymph node involvement), exclusive radiotherapy is recommended. For locally advanced anal cancer (tumor size >2 cm or lymph node involvement), standard therapy combines radiotherapy with concurrent 5-FU-MITOMYCINE C chemotherapy [84]. It has been reported that HIV-infected patients exhibit lower treatment tolerance with higher rates of severe acute skin, gastrointestinal and hematologic toxicities during chemoradiotherapy, which leads to prolonged overall treatment time compared with non-HIV-infected patients [68,74,77,81,82]. New radiation techniques, such as intensity-modulated radiation therapy or volumetric modulated arc therapy may decrease skin, bowel or hematological radiotherapy-induced toxicities. Localized relapse or persistent disease following chemoradiotherapy is treated using abdominoperineal resection with a permanent iliac colostomy [85]. 5-FU plus CDDP combination chemotherapy is the most common treatment regimen used for recurrent or metastatic anal cancer [86, 87]. screening There are no definitive guidelines for the screening of anal cancer. Screening for people at high risk for AIN consists in anal cytology testing (Pap tests) and digital anal examination. If digital anal examination reveals a macroscopic lesion or the anal Pap test reveals any abnormalities, high-resolution anoscopy should be carried out. Annals of Oncology In advanced cases, six to eight cycles of ABVD are recommended, leading to complete response rates of >85%, which is similar to that for non-HIV patients [90, 91, 93, 94]. A German group used the bleomycin, etoposide, adriamycin, cyclophosphamide, vincristine, procarbazine, prednisone (BEACOPP) baseline combination in advanced HIV-HL patients, achieving a 2-year OS rate of 87%, though resulting in 7% toxic mortality [90]. For this reason, ABVD should be kept as the standard of choice, but if BEACOPP is used no more than six cycles should be administered given that, in the German study, three of four patients with fatal neutropenic sepsis had experienced their fatal event after the seventh and eighth cycle of BEACOPP. Some prognostic factors have been identified for HIV-HL cases: high IPS [91, 94], stage III–IV [91], no complete response [90] and CD4 <200 cells/µl [94]. While the use of granulocyte colony-stimulating factor as a support following AVBD is controversial in non-HIV patients, it is necessary in HIV+ patients due to the increased hematological toxicity that causes frequent delays in administering ABVD [93]. salvage therapy The standard of care in refractory or relapsing patents is the same for both HIV-positive and -negative patients, i.e. salvage treatment followed by high-dose therapy and autologous stemcell transplant. HIV infection has been proven to not impair graft collection or engraftment, and early and long-term adverse events occur in a similar fashion to those observed in non-HIVinfected patients [95]. New drugs are now available for HIVnegative patients, such as brentuximab vedotin, which can be used in the same way as for HIV-infected patients [96]. Hodgkin’s lymphoma Unlike other tumors, the risk of HL was found to not be reduced in the ART era, mixed cellularity (MC) remains the most frequent histology but frequency of nodular sclerosis clearly increases [88]. The histologic subtypes of 848 HIV-HL patients are MC, nodular sclerosis and classical HL not otherwise specified in 35%, 30% and 38%, respectively [88]. In the French ANRS CO16 LYMPHOVIR cohort of 68 patients, histological distribution was 42 MC and 12 scleronodular HL. Fourteen cases could not be classified because the diagnosis was done on bone marrow, liver or small-needle biopsies [89]. The oncogenic role of EBV appears highly significant, as most cases of HIV-HL are associated with this virus. HIV-HL patients often present with advanced disease (stage III or IV), extranodal involvement, high frequency of B symptoms, altered performance status, higher International Prognostic Score (IPS) and older age [89–93]. Nevertheless, patients with limited-stage disease (I or II) represent 20%–35% of all cases. first-line therapy In stages I or II, the standard treatment consists of chemotherapy [two to four cycles of doxorubicin, bleomycin, vinblastine and dacarbazine (ABVD), according to prognostic factors collected during staging], followed by involved-field irradiation. This treatment provides similarly good results to those found for non-HIV patients, with reported complete remission rates of >90% [90, 91]. | Spano et al. antiretroviral treatments The current guidelines, in 2015, recommend starting ART in any HIV-infected patient independently of CD4 lymphocyte count [97]. Indeed, the early control of HIV replication is associated with optimal survival, less comorbidities and a massively reduced risk in HIV transmission. In patients receiving antiretroviral therapy, antiretroviral treatment should be continued during chemotherapy [97–102]. However, ART has to be adjusted to avoid drug interactions with chemotherapy leading potentially to higher toxicity (Table 3). The following should preferably be used: nucleoside reverse-transcriptase inhibitors, such as abacavir, emtricitabine or lamivudine; non-nucleoside reverse-transcriptase inhibitors—mostly rilpivirine; all integrasestrand transfer inhibitors, except elvitegravir; CCR5 antagonists. The management of antiretroviral drug and cytotoxic agent coadministration often requires expert knowledge and experience in order to reduce drug interactions and maintain virus control, with decisions made based on treatment history and drug-resistance tests. pharmacological aspects and drug interactions The pharmacological issues involved in the treatment of HIVinfected patients with malignancies not only concern Volume 27 | No. 3 | March 2016 reviews Annals of Oncology Table 3. Toxicities from antiretroviral treatment Toxicities Nucleoside reverse-transcriptase inhibitors Tenofovir Decreased bone-mineral density, osteomalacia, increased risk of fractures, decreased eGFR, Fanconi syndrome Emtricitabine/lamivudine Abacavir Rash, nausea, diarrhea, ischemic heart disease, systemic hypersensitivity syndrome (HLA B*5701-dependent) Stavudine Pancreatitis, steatosis, peripheral neuropathy, lipodystrophy, dyslipidemia, hyperlactatemia Didanosine Pancreatitis, steatosis, peripheral neuropathy, lipodystrophy, hyperlactatemia, ischemic heart disease, obliterative portal venopathy Zidovudine Nail pigmentation, nausea, steatosis, myopathy, rhabdomyolysis, dyslipidemia, hyperlactatemia, anemia, lipodystrophy Non-nucleoside reverse-transcriptase inhibitors Rilpivirine Rash, hepatitis, decreased eGFR, depression, sleep disturbances, headache Efavirenz Rash, hepatitis, dizziness, sleep disturbances, depression, dyslipidemia, gynecomastia, decreased plasma 25-(OH) vitamin D, teratogenesis Nevirapine Rash, hepatitis, systemic hypersensitivity (CD4 and gender-dependent) Etravirine Rash Protease inhibitors Atazanavir Jaundice cholelithiasis, decreased eGFR, nephrolithiasis, nausea, diarrhea, dyslipidemia Darunavir Rash, dyslipidemia Lopinavir Dyslipidemia, nausea, diarrhea, decreased eGFR, ischemic heart disease Indinavir Dry skin, nail dystrophy, jaundice, nephrolithiasis, abdominal fat, dyslipidemia, diabetes mellitus, nausea, diarrhea, ischemic heart disease Fosamprenavir Dyslipidemia, rash, nausea, diarrhea, ischemic heart disease Saquinavir Dyslipidemia, nausea, diarrhea Tipranavir Dyslipidemia, hepatitis, intracranial hemorrhage, diabetes mellitus, nausea, diarrhea Integrase-strand transfer inhibitors Raltegravir Nausea, myopathy, rhabdomyolysis, mood change Dolutegravir Rash, nausea, decreased eGFR due to inhibition of renal tubular creatinine secretion without affecting the glomerular filtration itself, headache, systemic hypersensitivity syndrome (<1%) Elvitegravir Nausea, vomiting, hyperbilirubinemia, decreased eGFR due to inhibition of renal tubular creatinine secretion without affecting the glomerular filtration itself, headache Fusion inhibitor Enfuvirtide Nodule injection, hypersensitivity CCR5 inhibitor Maraviroc Caution must be taken in the event of hepatitis co-infection and pre-existing liver damage, and in patients with heart failure eGFR, estimated glomerular filtration rate. antineoplastic agents but all treatments that may concern cancer disease management, such as antiemetics, analgesics, corticosteroid therapy or antimicrobial agents (Table 4). The potential of antiretrovirals to cause drug interactions is also well known and has been thoroughly documented [46, 103–108]. Drug–drug interactions can be classified into two categories: (i) Pharmacokinetic interactions caused by shared metabolic pathways and transporters between both the antiretrovirals and the anticancer drugs. These mostly concern the cytochrome P450 (CYP) enzyme system, particularly the CYP3A4/ 5 isoenzyme. Other isoenzymes, such as CYP1A2, CYP2C9, CYP2D6 or the phase-II UDP-glucuronosyltransferase 1A1 (UGT1A1) enzyme, can also be a cause for concern. These interactions generally result in the inhibition or induction of CYP isoenzymes or UGT1A1 by antiretrovirals, which leads to increased or decreased metabolism exposure of drug substrates to the same enzyme. (ii) Pharmacodynamic interactions are caused by synergistic or antagonistic effects and can lead to overlapping toxicities or decreased treatment efficiency. Volume 27 | No. 3 | March 2016 The antiretroviral drug classes with the highest risk of pharmacokinetic interactions are protease inhibitors (PI) and non-nucleoside reverse-transcriptase inhibitors (NNRTI). PIs are potent inhibitors of CYP3A (except tipranavir), with ritonavir being the most potent, which may potentially increase the exposure of several antineoplastic agents, leading to severe acute toxicities. In contrast, NNRTIs, except rilpivirine and the PI tipranavir, are inducers of CYP3A, which may increase the risk of treatment failure by decreasing anticancer-drug exposure. Integrase inhibitors—namely, raltegravir with almost no drug interactions and dolutegravir ‘with the exception of’ elvitegravir used as boosted by cobicistat—offer a favorable drug–drug interaction profile, partly due to a predominant metabolism ‘through’ glucuronidation by UGT1A1. Boosted PIs, NNRTIs and elvitegravir/cobicistat should generally be avoided in chemotherapy regimens that include drugs metabolized by CYP3A (Table 4). Pharmacodynamic interactions particularly concern NRTIs. Zidovudine, no longer used in western countries, must be avoided due to its increased risk of myelotoxicity with all doi:10.1093/annonc/mdv606 | reviews Annals of Oncology Table 4. Drug–drug interactions: principal recommendations for the use of antiretrovirals in association with major anticancer agents Antineoplastic agents Antiretrovirals not recommended ‘or’ requiring close specific monitoring ‘and/or’ dose adjustment if co-administered; Potential interactions; multidisciplinary discussion highly advised Authorized antiretrovirals±TDM and clinical monitoring; No clinically significant interaction expected Alkylating agents Cyclophosphamide Ifosfamide Bendamustine Boosted PI NNRTI except rilpivirine Elvitegravir/cobicistat with cyclophosphamide/ifosfamide Zidovudine Tenofovir with ifosfamidea Anthracyclines Daunorubicin Doxorubicin Epirubicin Antibiotic cytotoxics Bleomycin Dactinomycin Boosted PI NNRTI Elvitegravir/cobicistat Zidovudine Zidovudine with dactinomycin Rilpivirine Etravirine only with bendamustine Raltegravir, dolutegravir elvitegravir/cobicistat only with bendamustine Maravirocb, enfuvirtide NRTI except zidovudine Raltegravir, dolutegravir maraviroc, enfuvirtide NRTI except zidovudine Antimetabolites Methotrexate Pemetrexed Cytarabine Capecitabine Fluorouracil Gemcitabine Mercaptopurine Immunosuppressants, immuno-modulators Dacarbazine Everolimus Procarbazine Temsirolimus Monoclonal antibodies Alemtuzumab Bevacizumab Cetuximab Rituximab Panitumumab Trastuzumab Platinum derivatives Cisplatin Carboplatin Oxaliplatin Zidovudine Proteasome inhibitor Bortezomib Taxanes Docetaxel Paclitaxel Topoisomerase I and II inhibitors Etoposide Irinotecan Boosted PI Elvitegravir/cobicistat with everolimus/temsirolimus NNRTIe Zidovudine Boosted PI NNRTI Elvitegravir/cobicistat, raltegravir, dolutegravir maraviroc, enfuvirtide NRTI (zidovudine only with bleomycin) Boosted PI NNRTIc Elvitegravir/cobicistat, raltegravir, dolutegravir maraviroc, enfuvirtide NRTIa,d except zidovudine Elvitegravir/cobicistat only with procarbazine/ dacarbazine Raltegravir, dolutegravir maravirocb, enfuvirtide NRTI except zidovudine All antiretrovirals (zidovudine can be considered according to accompanying drugs) Elvitegravir/cobicistat with cisplatin Zidovudine, tenofovira Boosted PI NNRTI except rilpivirine Elvitegravir/cobicistat Zidovudine Boosted PI NNRTI except rilpivirine Elvitegravir/cobicistat Zidovudine Boosted PI NNRTI except rilpivirine Elvitegravir/cobicistat Zidovudine Boosted PI NNRTI Elvitegravir/cobicistat only with carboplatin/ oxaliplatin Raltegravir, dolutegravir, maraviroc, enfuvirtide NRTI except zidovudine and tenofovir Rilpivirine Raltegravir, dolutegravir, maraviroc, enfuvirtide NRTI except zidovudine Rilpivirineb Raltegravirb, dolutegravirb, maravirocb, enfuvirtide NRTI except zidovudine Rilpivirine Raltegravir, dolutegravir, maraviroc, enfuvirtide NRTI except zidovudine Continued | Spano et al. Volume 27 | No. 3 | March 2016 reviews Annals of Oncology Table 4. Continued Antineoplastic agents Antiretrovirals not recommended ‘or’ requiring close specific monitoring ‘and/or’ dose adjustment if co-administered; Potential interactions; multidisciplinary discussion highly advised Authorized antiretrovirals±TDM and clinical monitoring; No clinically significant interaction expected Tyrosine kinase inhibitors Imatinib Dasatinib Erlotinib Gefitinib Lapatinib Nilotinib Pazopanib Sorafenib Sunitinib Vinca alkaloids Vinblastine Vincristine Vinorelbine Boosted PI NNRTIe Elvitegravir/cobicistat Zidovudine Raltegravirb, dolutegravirb, maravirocb, enfuvirtide NRTI except zidovudine Boosted PI NNRTI except rilpivirine Elvitegravir/cobicistat Zidovudine Rilpivirineb Raltegravirb, dolutegravirb, maravirocb, enfuvirtide NRTI except zidovudine a Potential additive nephrotoxicity of tenofovir with ifosfamide, pemetrexed, methotrexate and platinum derivatives. Close monitoring of renal function advised. b Increase and/or decrease in antiretroviral exposure possible due to mild or moderate inhibitory effects of various anticancer agents on CYP isoenzymes; clinical and pharmacological monitoring may be advised. c Rilpivirine inhibits the active renal tubular secretion of creatinine and should be used with caution in combination with methotrexate and pemetrexed. Close monitoring of renal function advised. d Potential competition or inhibition of the metabolism of capecitabine and 5-fluorouracil by NRTI except abacavir, which may lead to increased fluorouracil toxicity. Clinical relevance unknown. e Rilpivirine may be authorized under specific monitoring in some cases, according to the anticancer agents administered. Boosted PI, protease inhibitors associated with ritonavir (atazanavir/r, darunavir/r, fosamprenavir/r, indinavir/r, lopinavir/r, saquinavir/r, tipranavir/r); NNRTI, non-nucleoside reverse-transcriptase inhibitors (efavirenz, etravirine, nevirapine, rilpivirine); NRTI, nucleos(t)ide reverse-transcriptase inhibitors (abacavir, emtricitabine, lamivudine, tenofovir, zidovudine). anticancer drugs, whereas tenofovir should not be administered along with potent nephrotoxic agents, such as cisplatin, methotrexate and ifosfamide. If no substitute for tenofovir can be found, its administration should be accompanied by close monitoring of the patient’s renal function. Rilpivirine, associated with prolongation of the QTc interval at supra-therapeutic doses, should be used with caution in combination with drugs that have the potential to increase the QT interval or in patients at risk for Torsade de Pointes. new perspectives in cancer treatment in HIV-infected patients The last 2 years have seen unprecedented progress in cancer treatment with therapeutic monoclonal antibodies restoring immune control of tumors by blocking the immune checkpoints on tumor-infiltrating lymphocytes. The first successes registered for anti-CTLA4 antibodies in melanoma were rapidly followed by anti-PD1/L1 antibodies which showed durable tumor responses on several cancer types including, apart from melanoma, tumors frequently involved in HIV-infected patients such as NSLC, NHL or HL [109–111]. These therapeutic antibodies should be as efficient in HIV-infected cancer patients and the rationale for these treatments should be strengthened further Volume 27 | No. 3 | March 2016 since T-cell overexpression of PD-1 and other immune checkpoints has been abundantly documented in HIV infection as part of the immune exhaustion characteristics of HIV-related immune deficiencies, particularly on T cells directed against HIV itself and oncogenic viruses, such as EBV or hepatotropic viruses [112, 113]. Therefore, the spectrum of action of these antibodies should be even broader in this context and help restore immune control of EBV+, HBV+ or HCV+ tumors. In addition, it is also proposed these antiantibodies reactivate latently infected CD4+ cells expressing these immune checkpoints and help purge the HIV reservoirs as part of a combined regimen toward HIV cure. Whether the same successes and good tolerability of anti-PD1/L1 antibodies observed in HIVnegative populations will be maintained in HIV+ patients is nevertheless a challenging question and a number of studies are in progress or due to start soon to answer these questions. Indeed, another challenge is to evaluate their tolerance with caution as, in this context, these therapeutic antibodies might prompt a severe immune restoration syndrome by rapidly restoring immune competence. It is particularly important to check their intestinal tolerability as the gut lymphoid tissues are durably affected by HIV-related immune alterations and antiCTLA-4 antibody usage is strongly limited in HIV-negative melanoma patients by the severe colitis induced by mucosal gut lymphocyte reactivation. Once good tolerance and efficacy of doi:10.1093/annonc/mdv606 | reviews immune checkpoint blockers is established in HIV-infected patients, one can envision a rapid revolution in the clinical management of cancers in HIV infection with the use of these antibodies becoming a top priority in HIV+ cancer medicine. conclusion A strong impetus for multidisciplinary collaboration in order to optimize the management of HIV-infected patients with malignancies has emerged over the last few years. As patient management in this setting is, by necessity, multidisciplinary, the development of multidisciplinary approaches involving hematologists, oncologists and HIV specialists has enabled the CANCERVIH group, supported by the French National Cancer Institute, to develop specific guidelines to target and aid HIVinfected patients. These patients are usually excluded from early-phase clinical trials and cannot therefore access the most innovative therapies. However, there is an urgent unmet need for investigation of such therapies, particularly immune-based therapies targeting the immune checkpoints at the interface of immunity and tumor cell proliferation in HIV-infected patients. acknowledgements The authors thank the INCa for its institutional support, Marianne Veyri for her administrative support and Jacques Cadranel for revising the lung cancer section of the manuscript. disclosure J-PS declares some potential conflicts of interest: Adboard or consultant: Gilead, Merck MSD, Roche, Teva Pharma Symposia: BMS, GSK. DC declares that she has received in the past 3 years: travel grants, consultancy fees, honoraria and study grants from various pharmaceutical companies including Gilead Sciences, Janssen-Cilag, Merck-Sharp & Dohme-Chibret, and ViiV Healthcare. SC declares a potential conflict of interest: Consultant: Roche. Véronique LEBLOND has received honoraria from Roche, Janssen, Gilead Sciences, GSK (board consultation, speaker bureau). CK has received travel grants, consultancy fees, honoraria and study grants from Bristol-Myers-Squibb (BMS), Merck-Sharp & Dohme-Chibret and ViiV Healthcare. M-AV has received honoraria for consulting/educational lectures and travel grants from Janssen-Cilag, Gilead Sciences, ViiV Healthcare, Bristol-Myers-Squibb and Merck/Schering-Plough. IP-M, FB, OR, AL, P-EH, JG, CS, AG, GC, BA and LQ have declared no conflicts of interest. references 1. Morlat P. Prise en Charge Médicale des Personnes Vivant Avec le VIH. Recommandations du Groupe D’experts. Rapport 2013. Paris : La Documentation Française ed: ANRS and CNS; 2013. p. 476. https://www.sidainfo-service.org/sites/sida/IMG/pdf/Rapport_Morlat_2013_Mise_en_ligne.pdf (18 January 2016, date last accessed) 2. Morlat P, Roussillon C, Henard S et al. Causes of death among HIV-infected patients in France in 2010 (national survey): trends since 2000. AIDS 2014; 28: 1181–1191. 3. Frisch M, Biggar RJ, Engels EA et al. Association of cancer with AIDS-related immunosuppression in adults. JAMA 2001; 285: 1736–1745. | Spano et al. Annals of Oncology 4. Goedert JJ, Cote TR, Virgo P et al. Spectrum of AIDS-associated malignant disorders. Lancet 1998; 351: 1833–1839. 5. Arvey A, Ojesina AI, Pedamallu CS et al. The tumor virus landscape of AIDSrelated lymphomas. Blood 2015; 125: e14–e22. 6. Chadburn A, Chiu A, Lee JY et al. Immunophenotypic analysis of AIDS-related diffuse large B-cell lymphoma and clinical implications in patients from AIDS Malignancies Consortium clinical trials 010 and 034. J Clin Oncol 2009; 27: 5039–5048. 7. Chao C, Silverberg MJ, Martinez-Maza O et al. Epstein-Barr virus infection and expression of B-cell oncogenic markers in HIV-related diffuse large B-cell Lymphoma. Clin Cancer Res 2012; 18: 4702–4712. 8. Grulich AE, van Leeuwen MT, Falster MO, Vajdic CM. Incidence of cancers in people with HIV/AIDS compared with immunosuppressed transplant recipients: a meta-analysis. Lancet 2007; 370: 59–67. 9. Shiels MS, Cole SR, Kirk GD, Poole C. A meta-analysis of the incidence of nonAIDS cancers in HIV-infected individuals. J Acquir Immune Defic Syndr 2009; 52: 611–622. 10. Spano JP, Costagliola D, Katlama C et al. AIDS-related malignancies: state of the art and therapeutic challenges. J Clin Oncol 2008; 26: 4834–4842. 11. Bower M, Palfreeman A, Alfa-Wali M et al. British HIV Association guidelines for HIV-associated malignancies 2014. HIV Med 2014; 15: 1–92. 12. Ntekim A, Campbell O, Rothenbacher D. Optimal management of cervical cancer in HIV-positive patients: a systematic review. Cancer Med 2015; 4: 1381–1393. 13. Arruda E, Jacome AA, Toscano AL et al. Consensus of the Brazilian Society of Infectious Diseases and Brazilian Society of Clinical Oncology on the management and treatment of Kaposi’s sarcoma. Braz J Infect Dis 2014; 18: 315–326. 14. Hentrich M, Hoffmann C, Mosthaf F et al. Therapy of HIV-associated lymphomarecommendations of the Oncology Working Group of the German Study Group of Physicians in Private Practice Treating HIV-Infected Patients (DAGNA), in cooperation with the German AIDS Society (DAIG). Ann Hematol 2014; 93: 913–921. 15. Torres HA, Mulanovich V. Management of HIV infection in patients with cancer receiving chemotherapy. Clin Infect Dis 2014; 59: 106–114. 16. Shiels MS, Pfeiffer RM, Engels EA. Age at cancer diagnosis among persons with AIDS in the United States. Ann Intern Med 2010; 153: 452–460. 17. Hleyhel M, Cancer Risk Group of the French Hospital Database on HIV. Risk of non-AIDS-defining cancers among HIV-1-infected individuals in France between 1997 and 2009: results from a French cohort. AIDS 2014; 28: 2109–2118. 18. Bhavan KP, Kampalath VN, Overton ET. The aging of the HIV epidemic. Curr HIV/ AIDS Rep 2008; 5: 150–158. 19. Effros RB, Fletcher CV, Gebo K et al. Aging and infectious diseases: workshop on HIV infection and aging: what is known and future research directions. Clin Infect Dis 2008; 47: 542–553. 20. Seaberg EC, Wiley D, Martinez-Maza O et al. Cancer incidence in the multicenter AIDS Cohort Study before and during the HAART era: 1984 to 2007. Cancer 2010; 116: 5507–5516. 21. Piketty C, Selinger-Leneman H, Bouvier AM et al. Incidence of HIV-related anal cancer remains increased despite long-term combined antiretroviral treatment: results from the French Hospital Database on HIV. J Clin Oncol 2012; 30: 4360–4366. 22. Franceschi S, Lise M, Clifford GM et al. Changing patterns of cancer incidence in the early- and late-HAART periods: the Swiss HIV Cohort Study. Br J Cancer 2010; 103: 416–422. 23. Guiguet M, Boue F, Cadranel J et al. Effect of immunodeficiency, HIV viral load, and antiretroviral therapy on the risk of individual malignancies (FHDH-ANRS CO4): a prospective cohort study. Lancet Oncol 2009; 10: 1152–1159. 24. Palefsky JM, Holly EA. Chapter 6: immunosuppression and co-infection with HIV. J Natl Cancer Inst Monogr 2003; 41–46. 25. Silverberg MJ, Chao C, Leyden WA et al. HIV infection, immunodeficiency, viral replication, and the risk of cancer. Cancer Epidemiol Biomarkers Prev 2011; 20: 2551–2559. 26. Engels EA, Brock MV, Chen J et al. Elevated incidence of lung cancer among HIV-infected individuals. J Clin Oncol 2006; 24: 1383–1388. 27. Chaturvedi AK, Pfeiffer RM, Chang L et al. Elevated risk of lung cancer among people with AIDS. AIDS 2007; 21: 207–213. Volume 27 | No. 3 | March 2016 Annals of Oncology 28. Kirk GD, Merlo C, O’Driscoll P et al. HIV infection is associated with an increased risk for lung cancer, independent of smoking. Clin Infect Dis 2007; 45: 103–110. 29. Helleberg M, Gerstoft J, Afzal S et al. Risk of cancer among HIV-infected individuals compared to the background population: impact of smoking and HIV. AIDS 2014; 28: 1499–1508. 30. Pine SR, Mechanic LE, Enewold L et al. Increased levels of circulating interleukin 6, interleukin 8, C-reactive protein, and risk of lung cancer. J Natl Cancer Inst 2011; 103: 1112–1122. 31. Valiathan R, Miguez MJ, Patel B et al. Tobacco smoking increases immune activation and impairs T-cell function in HIV infected patients on antiretrovirals: a cross-sectional pilot study. PLoS One 2014; 9: e97698. 32. Guideline on When to Start Antiretroviral Therapy and on pre-Exposure Prophylaxis for HIV. In Data WLC-i-P Edition. World Health Organization 2015. http://apps.who.int/iris/bitstream/10665/186275/1/9789241509565_eng.pdf (18 January 2016, date last accessed). 33. Tron L, Lert F, Spire B et al. Tobacco smoking in HIV-infected versus general population in France: heterogeneity across the various groups of people living with HIV. PLoS One 2014; 9: e107451. 34. Leone FT, Evers-Casey S, Toll BA, Vachani A. Treatment of tobacco use in lung cancer: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2013; 143: e61S–e77S. 35. Mani D, Haigentz M, Jr, Aboulafia DM. Lung cancer in HIV infection. Clin Lung Cancer 2012; 13: 6–13. 36. Brock MV, Hooker CM, Engels EA et al. Delayed diagnosis and elevated mortality in an urban population with HIV and lung cancer: implications for patient care. J Acquir Immune Defic Syndr 2006; 43: 47–55. 37. D’Jaen GA, Pantanowitz L, Bower M et al. Human immunodeficiency virusassociated primary lung cancer in the era of highly active antiretroviral therapy: a multi-institutional collaboration. Clin Lung Cancer 2010; 11: 396–404. 38. Rengan R, Mitra N, Liao K et al. Effect of HIV on survival in patients with nonsmall-cell lung cancer in the era of highly active antiretroviral therapy: a population-based study. Lancet Oncol 2012; 13: 1203–1209. 39. Sigel K, Wisnivesky J, Gordon K et al. HIV as an independent risk factor for incident lung cancer. AIDS 2012; 26: 1017–1025. 40. Suneja G, Shiels MS, Angulo R et al. Cancer treatment disparities in HIV-infected individuals in the United States. J Clin Oncol 2014; 32: 2344–2350. 41. Coghill AE, Shiels MS, Suneja G, Engels EA. Elevated cancer-specific mortality among HIV-infected patients in the United States. J Clin Oncol 2015; 33: 2376–2383. 42. Hleyhel M, Belot A, Bouvier AM et al. Trends in survival after cancer diagnosis among HIV-infected individuals between 1992 and 2009. Results from the FHDH-ANRS CO4 cohort. Int J Cancer 2015; 137: 2443–2453. 43. Besse B, Adjei A, Baas P et al. 2nd ESMO Consensus Conference on Lung Cancer: non-small-cell lung cancer first-line/second and further lines of treatment in advanced disease. Ann Oncol 2014; 25: 1475–1484. 44. Vansteenkiste J, De Ruysscher D, Eberhardt WE et al. Early and locally advanced non-small-cell lung cancer (NSCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2013; 24(Suppl 6): vi89–vi98. 45. Makinson A, Tenon JC, Eymard-Duvernay S et al. Human immunodeficiency virus infection and non-small cell lung cancer: survival and toxicity of antineoplastic chemotherapy in a cohort study. J Thorac Oncol 2011; 6: 1022–1029. 46. Rudek MA, Flexner C, Ambinder RF. Use of antineoplastic agents in patients with cancer who have HIV/AIDS. Lancet Oncol 2011; 12: 905–912. 47. Deeken J, Beumer J, Anders N et al. Preclinical assessment of the interactions between the antiretroviral drugs, ritonavir and efavirenz, and the tyrosine kinase inhibitor erlotinib. Cancer Chemother Pharmacol 2015; 76: 813–819. 48. Brahmer J, Reckamp KL, Baas P et al. Nivolumab versus docetaxel in advanced squamous-cell non-small-cell lung cancer. N Engl J Med 2015; 373: 123–135. 49. Borghaei H, Paz-Ares L, Horn L et al. Nivolumab versus docetaxel in advanced nonsquamous non-small-cell lung cancer. N Engl J Med 2015; 373: 1627–1639. 50. National Lung Screening Trial Research TAberle DR, Adams AM et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med 2011; 365: 395–409. Volume 27 | No. 3 | March 2016 reviews 51. Makinson A, Eymard-Duvernay S, Raffi F et al. Feasibility and efficacy of early lung cancer diagnosis with chest computed tomography in HIV-infected smokers. The ANRS EP48 HIV CHEST Study. AIDS 2015 October 30 [epub ahead of print], doi: 10.1097/QAD.0000000000000943. 52. Hulbert A, Hooker CM, Keruly JC et al. Prospective CT screening for lung cancer in a high-risk population: HIV-positive smokers. J Thorac Oncol 2014; 9: 752–759. 53. Brau N, Fox RK, Xiao P et al. Presentation and outcome of hepatocellular carcinoma in HIV-infected patients: a U.S.-Canadian multicenter study. J Hepatol 2007; 47: 527–537. 54. Lim C, Goutte N, Gervais A et al. Standardized care management ensures similar survival rates in HIV-positive and HIV-negative patients with hepatocellular carcinoma. J Acquir Immune Defic Syndr 2012; 61: 581–587. 55. Bruix J, Sherman M, American Association for the Study of Liver D. Management of hepatocellular carcinoma: an update. Hepatology 2011; 53: 1020–1022. 56. European Association For The Study of The L, European Organisation For R, Treatment of C. EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol 2012; 56: 908–943. 57. Verslype C, Rosmorduc O, Rougier P, Group EGW. Hepatocellular carcinoma: ESMO-ESDO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2012; 23(Suppl 7): vii41–vii48. 58. Wilkins E, Nelson M, Agarwal K et al. British HIV Association guidelines for the management of hepatitis viruses in adults infected with HIV 2013. HIV Med 2013; 14(Suppl 4): 1–71. 59. Di Benedetto F, De Ruvo N, Berretta M et al. Hepatocellular carcinoma in HIV patients treated by liver transplantation. Eur J Surg Oncol 2008; 34: 422–427. 60. Di Benedetto F, Di Sandro S, De Ruvo N et al. Human immunodeficiency virus and liver transplantation: our point of view. Transplant Proc 2008; 40: 1965–1971. 61. Di Benedetto F, Tarantino G, Ercolani G et al. Multicenter Italian experience in liver transplantation for hepatocellular carcinoma in HIV-infected patients. Oncologist 2013; 18: 592–599. 62. Berretta M, Garlassi E, Cacopardo B et al. Hepatocellular carcinoma in HIVinfected patients: check early, treat hard. Oncologist 2011; 16: 1258–1269. 63. Vibert E, Duclos-Vallee JC, Ghigna MR et al. Liver transplantation for hepatocellular carcinoma: the impact of human immunodeficiency virus infection. Hepatology 2011; 53: 475–482. 64. Nunnari G, Berretta M, Pinzone MR et al. Hepatocellular carcinoma in HIV positive patients. Eur Rev Med Pharmacol Sci 2012; 16: 1257–1270. 65. Gelu-Simeon M, Sobesky R, Haim-Boukobza S et al. Do the epidemiology, physiological mechanisms and characteristics of hepatocellular carcinoma in HIVinfected patients justify specific screening policies? AIDS 2014; 28: 1379–1391. 66. Berretta M, Di Benedetto F, Dal Maso L et al. Sorafenib for the treatment of unresectable hepatocellular carcinoma in HIV-positive patients. Anticancer Drugs 2013; 24: 212–218. 67. Ozenne V, Gervais A, Peytavin G et al. Suspected interaction between sorafenib and HAART in an HIV-1 infected patient: a case report. Hepatogastroenterology 2011; 58: 161–162. 68. Abramowitz L, Mathieu N, Roudot-Thoraval F et al. Epidermoid anal cancer prognosis comparison among HIV+ and HIV- patients. Aliment Pharmacol Ther 2009; 30: 414–421. 69. Abramowitz L, Jacquard AC, Jaroud F et al. Human papillomavirus genotype distribution in anal cancer in France: the EDiTH V study. Int J Cancer 2011; 129: 433–439. 70. Mendez-Martinez R, Rivera-Martinez NE, Crabtree-Ramirez B et al. Multiple human papillomavirus infections are highly prevalent in the anal canal of human immunodeficiency virus-positive men who have sex with men. BMC Infect Dis 2014; 14: 671. 71. Kreuter A, Potthoff A, Brockmeyer NH et al. Anal carcinoma in human immunodeficiency virus-positive men: results of a prospective study from Germany. Br J Dermatol 2010; 162: 1269–1277. 72. Palefsky JM, Holly EA, Efirdc JT et al. Anal intraepithelial neoplasia in the highly active antiretroviral therapy era among HIV-positive men who have sex with men. AIDS 2005; 19: 1407–1414. doi:10.1093/annonc/mdv606 | reviews 73. Watson AJ, Smith BB, Whitehead MR et al. Malignant progression of anal intraepithelial neoplasia. ANZ J Surg 2006; 76: 715–717. 74. Cleator S, Fife K, Nelson M et al. Treatment of HIV-associated invasive anal cancer with combined chemoradiation. Eur J Cancer 2000; 36: 754–758. 75. Stadler RF, Gregorcyk SG, Euhus DM et al. Outcome of HIV-infected patients with invasive squamous-cell carcinoma of the anal canal in the era of highly active antiretroviral therapy. Dis Colon Rectum 2004; 47: 1305–1309. 76. Wexler A, Berson AM, Goldstone SE et al. Invasive anal squamous-cell carcinoma in the HIV-positive patient: outcome in the era of highly active antiretroviral therapy. Dis Colon Rectum 2008; 51: 73–81. 77. Oehler-Janne C, Huguet F, Provencher S et al. HIV-specific differences in outcome of squamous cell carcinoma of the anal canal: a multicentric cohort study of HIV-positive patients receiving highly active antiretroviral therapy. J Clin Oncol 2008; 26: 2550–2557. 78. Seo Y, Kinsella MT, Reynolds HL et al. Outcomes of chemoradiotherapy with 5Fluorouracil and mitomycin C for anal cancer in immunocompetent versus immunodeficient patients. Int J Radiat Oncol Biol Phys 2009; 75: 143–149. 79. Hogg ME, Popowich DA, Wang EC et al. HIV and anal cancer outcomes: a single institution’s experience. Dis Colon Rectum 2009; 52: 891–897. 80. Abramowitz L, Remy V, Vainchtock A. Economic burden of anal cancer management in France. Rev Epidemiol Sante Publique 2010; 58: 331–338. 81. Fraunholz I, Weiss C, Eberlein K et al. Concurrent chemoradiotherapy with 5fluorouracil and mitomycin C for invasive anal carcinoma in human immunodeficiency virus-positive patients receiving highly active antiretroviral therapy. Int J Radiat Oncol Biol Phys 2010; 76: 1425–1432. 82. Munoz-Bongrand N, Poghosyan T, Zohar S et al. Anal carcinoma in HIV-infected patients in the era of antiretroviral therapy: a comparative study. Dis Colon Rectum 2011; 54: 729–735. 83. Quero L, Duval X, Abramowitz L. [Anal cancer in HIV patients]. Bull Cancer 2014; 101: 1034–1039. 84. Glynne-Jones R, Northover JM, Cervantes A, Group EGW. Anal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2010; 21(Suppl 5): v87–v92. 85. Cunin L, Alfa-Wali M, Turner J et al. Salvage surgery for residual primary and locally recurrent anal squamous cell carcinoma after chemoradiotherapy in HIVpositive individuals. Ann Surg Oncol 2014; 21: 527–532. 86. Faivre C, Rougier P, Ducreux M et al. [5-fluorouracile and cisplatinum combination chemotherapy for metastatic squamous-cell anal cancer]. Bull Cancer 1999; 86: 861–865. 87. Jaiyesimi IA, Pazdur R. Cisplatin and 5-fluorouracil as salvage therapy for recurrent metastatic squamous cell carcinoma of the anal canal. Am J Clin Oncol 1993; 16: 536–540. 88. Shiels MS, Koritzinsky EH, Clarke CA et al. Prevalence of HIV infection among U. S. Hodgkin lymphoma cases. Cancer Epidemiol Biomarkers Prev 2014; 23: 274–281. 89. Besson C, Lancar R, Prevot S et al. High risk features contrast with favorable outcomes in HIV-associated Hodgkin lymphoma in the modern cART era, ANRS CO16 LYMPHOVIR Cohort. Clin Infect Dis 2015; 61: 1469–1475. 90. Hentrich M, Berger M, Wyen C et al. Stage-adapted treatment of HIV-associated Hodgkin lymphoma: results of a prospective multicenter study. J Clin Oncol 2012; 30: 4117–4123. 91. Montoto S, Shaw K, Okosun J et al. HIV status does not influence outcome in patients with classical Hodgkin lymphoma treated with chemotherapy using doxorubicin, bleomycin, vinblastine, and dacarbazine in the highly active antiretroviral therapy era. J Clin Oncol 2012; 30: 4111–4116. 92. Uldrick TS, Little RF. How I treat classical Hodgkin lymphoma in patients infected with human immunodeficiency virus. Blood 2015; 125: 1226–1235; quiz 1355. 93. Xicoy B, Ribera JM, Miralles P et al. Results of treatment with doxorubicin, bleomycin, vinblastine and dacarbazine and highly active antiretroviral therapy in advanced stage, human immunodeficiency virus-related Hodgkin’s lymphoma. Haematologica 2007; 92: 191–198. 94. Castillo JJ, Bower M, Bruhlmann J et al. Prognostic factors for advanced-stage human immunodeficiency virus-associated classical Hodgkin lymphoma treated | Spano et al. Annals of Oncology 95. 96. 97. 98. 99. 100. 101. 102. 103. 104. 105. 106. 107. 108. 109. 110. 111. 112. 113. with doxorubicin, bleomycin, vinblastine, and dacarbazine plus combined antiretroviral therapy: a multi-institutional retrospective study. Cancer 2015; 121: 423–431. Gabarre J, Marcelin AG, Azar N et al. High-dose therapy plus autologous hematopoietic stem cell transplantation for human immunodeficiency virus (HIV)related lymphoma: results and impact on HIV disease. Haematologica 2004; 89: 1100–1108. Gandhi M, Petrich A. Brentuximab vedotin in patients with relapsed HIV-related lymphoma. J Natl Compr Canc Netw 2014; 12: 16–19; quiz 19. Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents. Department of Health and Human Services. http://www.aidsinfo.nih.gov/ContentFiles/Adultand Adoles-centGL.pdf (26 November 2015, date last accessed). Hoen B, Bonnet F, Delaugerre C et al. French 2013 guidelines for antiretroviral therapy of HIV-1 infection in adults. J Int AIDS Soc 2014; 17: 19034. European Aids Clinical Society Guidelines In Edition Version 7.1. European AIDS Clinical Society (EACS) 2014. Lennox JL, Landovitz RJ, Ribaudo HJ et al. Efficacy and tolerability of 3 nonnucleoside reverse transcriptase inhibitor-sparing antiretroviral regimens for treatment-naive volunteers infected with HIV-1: a randomized, controlled equivalence trial. Ann Intern Med 2014; 161: 461–471. Raffi F, Babiker AG, Richert L et al. Ritonavir-boosted darunavir combined with raltegravir or tenofovir-emtricitabine in antiretroviral-naive adults infected with HIV-1: 96 week results from the NEAT001/ANRS143 randomised non-inferiority trial. Lancet 2014; 384: 1942–1951. Clotet B, Feinberg J, van Lunzen J et al. Once-daily dolutegravir versus darunavir plus ritonavir in antiretroviral-naive adults with HIV-1 infection (FLAMINGO): 48 week results from the randomised open-label phase 3b study. Lancet 2014; 383: 2222–2231. Deeken JF, Pantanowitz L, Dezube BJ. Targeted therapies to treat non-AIDSdefining cancers in patients with HIV on HAART therapy: treatment considerations and research outlook. Curr Opin Oncol 2009; 21: 445–454. Brown KC, Paul S, Kashuba AD. Drug interactions with new and investigational antiretrovirals. Clin Pharmacokinet 2009; 48: 211–241. Dickinson L, Khoo S, Back D. Pharmacokinetics and drug-drug interactions of antiretrovirals: an update. Antiviral Res 2010; 85: 176–189. Cianfrocca M, Lee S, Von Roenn J et al. Pilot study evaluating the interaction between paclitaxel and protease inhibitors in patients with human immunodeficiency virus-associated Kaposi’s sarcoma: an Eastern Cooperative Oncology Group (ECOG) and AIDS Malignancy Consortium (AMC) trial. Cancer Chemother Pharmacol 2011; 68: 827–833. Corona G, Vaccher E, Sandron S et al. Lopinavir-ritonavir dramatically affects the pharmacokinetics of irinotecan in HIV patients with Kaposi’s sarcoma. Clin Pharmacol Ther 2008; 83: 601–606. Rudek MA, Moore PC, Mitsuyasu RT et al. A phase 1/pharmacokinetic study of sunitinib in combination with highly active antiretroviral therapy in human immunodeficiency virus-positive patients with cancer: AIDS Malignancy Consortium trial AMC 061. Cancer 2014; 120: 1194–1202. Perez-Gracia JL, Labiano S, Rodriguez-Ruiz ME et al. Orchestrating immune check-point blockade for cancer immunotherapy in combinations. Curr Opin Immunol 2014; 27: 89–97. Westin JR, Chu F, Zhang M et al. Safety and activity of PD1 blockade by pidilizumab in combination with rituximab in patients with relapsed follicular lymphoma: a single group, open-label, phase 2 trial. Lancet Oncol 2014; 15: 69–77. Taube JM, Klein A, Brahmer JR et al. Association of PD-1, PD-1 ligands, and other features of the tumor immune microenvironment with response to anti-PD1 therapy. Clin Cancer Res 2014; 20: 5064–5074. Day CL, Kaufmann DE, Kiepiela P et al. PD-1 expression on HIV-specific T cells is associated with T-cell exhaustion and disease progression. Nature 2006; 443: 350–354. Trautmann L, Janbazian L, Chomont N et al. Upregulation of PD-1 expression on HIV-specific CD8+ T cells leads to reversible immune dysfunction. Nat Med 2006; 12: 1198–1202. Volume 27 | No. 3 | March 2016