Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Body fat percentage wikipedia , lookup
Adipose tissue wikipedia , lookup
Food choice wikipedia , lookup
Fat acceptance movement wikipedia , lookup
Epidemiology of metabolic syndrome wikipedia , lookup
Diet-induced obesity model wikipedia , lookup
Abdominal obesity wikipedia , lookup
Human nutrition wikipedia , lookup
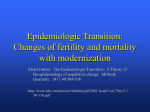
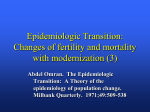
2771 Differences in Coronary Mortalit Can Be Explained by Differences in Cholesterol and Saturated Fat Intakes in 40 Countries but Not in France and Finland A Paradox Sabine M. Artaud-Wild, BS, RD; Sonja L. Connor, MS, RD; Gary Sexton, PhD; William E. Connor, MD Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 Background. For decades, the coronary heart disease (CHD) mortality rate has been four or more times higher in Finland than in France despite comparable intakes of dietary cholesterol and saturated fat. A potential answer to this paradox is provided by this study of 40 countries and the analyses of other nutrients in the diets besides cholesterol and saturated fat. Medhds and Resuls. CHD death rates for men aged 55 to 64 years were derived from the World Health Organization annual vital statistics. Dietary intakes were gathered from the Food and Agriculture Organization of the United Nations database. Forty countries at various levels of economic development and 40 dietary variables were investigated, including a lipid score that combined the intakes of cholesterol and saturated fat (Cholesterol-Saturated Fat Index (CSIJ). The CSI was significantly and positively related to CHD mortality in the 40 countries. The countries with low CSIs had low CHD death rates. Countries with high CSIs had a wide range of CHD death rates. France, Finland, and other Western industrialized countries had similar CSIs. After adjusting for cholesterol and saturated fat, milk and many components of milk (butterfat, milk protein, calcium from milk, and riboflavin) and total calcium remained positively related to CHD mortality for all 40 countries. There were differences in the consumption of these foods and nutrients in France and Finland. Milk and butterfat (fat from milk, cream, cheese, and butter) consumption was higher in Finland than in France. The consumption of plant foods, recently shown to be protective against CHD (vegetables and vegetable oils containing monounsaturated and polyunsaturated fatty acids), was greater in France than in Finland. Conchusions. Over the years, France and Finland, with similar intakes of cholesterol and saturated fat, consistently have had very different CHI) mortality rates. This paradox may be explained as follows. Given a high intake of cholesterol and saturated fat, the country in which people also consume more plant foods, including small amounts of liquid vegetable oils, and more vegetables (more antioxidants) had lower rates of CHD mortality. On the other hand, milk and butterfat were associated with increased CHD mortality, possibly through their effects on thrombosis as well as on atherosclerosis. (Ciulaion. 1993;88:2771-2779.) KEY WORDs * thrombosis * diet * cholesterol * heart disease * mortality In the late 1950s, an epidemiological paradox was observed. There were large geographical differences in mortality from coronary heart disease (CHD) among European countries, particularly between France and Finland, despite their having comparable intakes of dietary fat.' Finland had the highest rate of CHD mortality, and France was at the lower end of the range. Finland also stood out as having the highest CHD mortality in the Seven Countries Study.2 In a study of 24 countries in 1961, the correlation between dietary cholesterol and CHD was high (r=.83). Received January 12, 1993; revision accepted July 26, 1993. From the Division of Endocrinology, Diabetes, and Clinical Nutrition, Department of Medicine, The Oregon Health Sciences University, Portland, Ore. Correspondence to Dr William E. Connor, Department of Medicine, L-465, Oregon Health Sciences University, 3181 SW Sam Jackson Park Rd, Portland, OR 97201-3098. However, with comparable intakes of dietary cholesterol in France and Finland, the CHD mortality rate for men aged 55 to 59 was four times higher in Finland than in France.3 The same mortality difference was reported in 1982 by Liu et a14 using data from 1954 and 1965 and a lipid score based on the Keys equation. Dietary cholesterol and saturated fat are the two nutrients most associated with CHD. We combined their impact into a lipid score, the Cholesterol-Saturated Fat Index (CSI) and then compared the relation of this index with the coronary mortality in 40 countries as previously published.5 France and Finland continued to exhibit very different coronary mortality rates while having comparable CSIs. The CHD mortality in France, strikingly lower than observed in comparably developed countries, has been noted by others as well.6'7 Whenever epidemiological paradoxes exist, a reason should ultimately be found for them. A classic example 2772 Circulation Vol 88, No 6 December 1993 Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 is that of marine oils and the Eskimos. Early Arctic explorers and subsequent medical observers found that cardiovascular disease was rare in the Eskimos despite their consuming a diet almost exclusively derived from animal foods, which clearly had a very high fat and cholesterol content.8 Bang and Dyerberg9 later explained this discrepancy by noting the differences in the types of dietary fat eaten by the Eskimos and by the people in Western countries. The fat consumed by the Eskimos was almost completely derived from food from the sea: seal, whale, and fish. These fats all contain large quantities of the highly polyunsaturated w-3 fatty acids, which are both hypolipidemic and antithrombotic. A popular view is that the French have a lower coronary mortality because of their consumption of red wine, goose liver pate, and cheese. In our view, this hypothesis requires scientific validation. Using data that represent the 1950s through the 1980s, we examined the relations of coronary mortality to the intakes of foods and nutrients in 40 countries. We focused specifically on France, with a relatively low coronary mortality, and Finland, with the highest coronary mortality. There was a greater consumption of vegetables and unsaturated fat in France. There was greater consumption of milk and butterfat in Finland. These relations occurred after appropriate adjustment for the intakes of cholesterol and saturated fat and suggested the possibility of effects of other dietary factors in influencing the development of CHD. Methods All countries with populations of more than 1 million and for which both CHD mortality rates and food supply data could be obtained were included in the study. The 40 countries meeting these criteria covered all areas of the globe and nations in differing stages of industrial development: Austria, Belgium, Denmark, Finland, France, Hungary, Ireland, The Netherlands, Norway, Poland, Sweden, Switzerland, the United Kingdom, West Germany, Bulgaria, Egypt, Greece, Israel, Italy, Portugal, Romania, Spain, Yugoslavia, Canada, the United States, Argentina, Chile, Costa Rica, Cuba, the Dominican Republic, Ecuador, Mexico, Nicaragua, Paraguay, Uruguay, Venezuela, Australia, New Zealand, Hong Kong, and Japan. We did not consider other risk factors for CHD such as cigarette smoking or hypertension. However, it is generally accepted that cigarette smoking is prevalent in many of the countries where a low-fat diet is consumed and that people in these countries generally have low plasma lipid and lipoprotein levels. Also, Japan, with a low-fat diet and a low CHD mortality rate, has a high incidence of hypertension. Still, the fact that the data from analyses presented in this article fit so well with metabolic data from both human and animal studies suggests that diet is a major factor in determining coronary mortality rates throughout the world.10 World Health Organization reports were used as the source of CHD mortality statistics, ischemic heart disease (International Classification of Diseases, 410-414, "A" list, A83, 8th revision) being taken as the term equal to CHD.1" Mortality data were collected for 1977 before the latest changes in the international classification of diseases were introduced.12 These data represent the more typical picture for the 1950s through the 1980s. CHD mortality rates were expressed as deaths 100 000 population in men aged 55 to 64 years in the 40 countries. To determine the consistency over time, we compared CHD mortality rates in women and men at different ages in France and Finland for 1977 as well as in men age 55 to 64 for every year between 1961 and 1988. Average food disappearance data for years 1975 through 1977 were collected for each country from the Food Balance Sheets of the Food and Agriculture Organization (FAO) of the United Nations.13 Correlation coefficients computed using food data from either 1967 or 1977 and coronary mortality yielded similar results. Because there were food data for more countries in 1977, we elected to use that year. The FAO data listing the amounts of specific food items in grams available per day per inhabitant for each country were used in this study. Food Balance Sheets provide a reasonable picture of food or nutrients available for consumption. No allowance is made for spoilage and table waste, nor are indications given about differences that may exist in the diet consumed by different age, sex, or socioeconomic groups within a country. However, these data (based on food produced plus food imported minus food exported and divided by the number of inhabitants and by the number of days in the year) provide an estimate of per person per day food supply for each country. While it is recognized that they may give only crude approximations of actual individual intake, food disappearance data are useful for allowing intercountry comparisons of dietary patterns. Furthermore, food disappearance data are useful in generating hypotheses about dietary factors associated with disease' and have been widely used in published studies.3,415-'7 Imputed intakes taken directly from the FAO books were used as the basis for dietary intake in the analyses for fish, cheese, milk, rice, eggs, wine, and calories from both animal and vegetable foods. Because we wanted to examine the relation of nutrients known to be associated with coronary mortality, we used the extensive database of the Nutrition Coordinating Center (NCC) at the University of Minnesota to compute nutrient intakes using the amounts of foods consumed by each of the 40 countries as listed in the FAO books.'819 The energy, fat, and protein intakes estimated for each country using the NCC database were similar to the intakes listed in the FAO tables, which led us to think that other nutrient intakes computed using the NCC database were reliable. The saturated fat and other nutrient intakes in France were similar to those reported in a number of studies.4'6'7 Because of the wide range of energy intakes among the countries, we elected to express all nutrients as some function of energy intake, either as a percentage of calories or as an amount per 1000 kcal. We considered two lipid scores. One was computed using the Hegsted equation,20 which includes saturated and polyunsaturated fat as well as cholesterol (as does the Keys equation21'22). The second was computed using the equation for the CSI: CSI=(1.01xg saturated fat)+ (0.05 xmg cholesterol).5 The correlation of the two lipid scores for all 40 countries was .98. The lipid score computed using the CSI was selected for the analyses instead of the score using the Hegsted equation for three reasons. First, a high CSI indicates a high intake per Artaud-Wild et al Coronary Mortality in France and Finland of cholesterol and saturated fat. These nutrients have the greatest elevating effect on the total plasma and low-density lipoprotein (LDL) cholesterol through their effects in decreasing LDL receptor activity in the liver.2324 Second, the primary effect of polyunsaturated fat is to lower plasma total and LDL cholesterol by enhancing excretion of sterols from the body.25 These fatty acids do not affect LDL receptor activity. Third, the powerful effects of cholesterol and saturated fat might mask any effect of polyunsaturated and monounsaturated fat on CHD mortality. Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 Statistical Analysis The raw nutrient data for 40 countries were converted into nutrient density data, and Pearson productmoment correlation coefficients were calculated between CHD mortality and each of the nutrients. In a study such as this, one might expect to find strong intercorrelations among variables known from previous studies to be strongly related. In this context, the 40 dietary and food variables presented do not represent variables that are unrelated. Intercorrelations among groups of food-related variables were strong enough to suggest multicollinearity. For example, calories from animal and vegetable sources were strongly and inversely correlated (r= -.98). Intercorrelations between milk and components of milk (calcium, protein, and butterfat) were .85 and higher. This was also true for the components of meat as well as total fat and its components (saturated, monounsaturated, and polyunsaturated). Except for polyunsaturated fat, the measures of fat intake were also strongly related to CSI (r>.76). To account for interrelations among these variables, further analyses were completed. Partial correlation coefficients were computed relating CHD mortality and dietary variables including foods as well as nutrients as independent variables.26'27 Dietary cholesterol and saturated fat are such strong determinants of CHD mortality that they could mask any other dietary effects. To examine relations between CHD mortality and dietary variables apart from cholesterol and saturated fat, we first adjusted the data for cholesterol and saturated fat (CSI per 1000 kcal) by computing partial correlation coefficients between CHD mortality and dietary variables. The primary correlation analyses were done using data from all 40 countries. Because France and Finland may be regarded as anomalies and might unduly influence the relations of dietary factors and CHD mortality, the correlational studies were repeated using the data from 38 countries excluding France and Finland. The results of these analyses were similar to those of the 40 countries. Differences that occurred when France and Finland were excluded from the analysis are discussed in the text. Even though calories from vegetable foods and calories from animal foods were highly correlated with CHD mortality, both of these were excluded from further analyses to allow for the identification of specific foods and nutrients related to CHD mortality. The data presented in Tables 1 and 2 and Fig 2A and 2B include all 40 countries. The data presented in Table 3 include France, West Germany, the United Kingdom, and Finland. The data presented in Fig 1 include only France and Finland. A somewhat surprising finding, based on simple correlation coefficients, was a positive association with 2773 TABLE 1. Relation of Coronary Heart Disease Mortality Rates and 40 Dietary Variables In Men Aged 55 to 64 Years for 40 Countries (Year 1977) Significant Item Calories from animal foods Cholesterol-saturated fat index/1 000 kcal Cholesterol, mg/1000 kcal Saturated fat, % kcal Monounsaturated fat, % kcal Total fat, % kcal Total protein, % koal Alcohol, g/1 000 kcal Milk, g/1000 koal Milk calcium, mg/1000 kcal Milk protein, g/1000 kcal Butterfat, g/1000 kcal Eggs, g/1 000 kcal Meat calcium, mg/1 000 kcal Meat protein, g/1 000 kcal Meat fat, g/1 000 kcal Riboflavin, mg/1000 kcal Sodium, mg/1000 kcal Calcium, mg/1000 kcal Phosphorus, mg/1000 kcal Calories from vegetable foods Total carbohydrates, % kcal Starch, g/1 000 kcal Rice, g/1 000 kcal Fiber, g/1 000 kcal Thiamin, mg/1000 kcal Folic acid, ,ug/1 000 kcal Vitamin E, mg/1000 kcal Iron, mg/1000 kcal co-3 Fatty acids, % kcal Polyunsaturated fat, % kcal Sucrose, g/1 000 kcal Fish, seafood, g/1000 kcal Cheese, g/1 000 kcal Wine, g/1000 kcal Vitamin C, mg/1000 kcal Niacin, mg/1000 kcal Vitamin A, IU/1000 kcal Magnesium, mg/1000 kcal Potassium, mg/1000 kcal *P<.001; tP<.01; 4P<.05. Positive Correlations .79* .78* .69* .77* .46t .62* .37* .35* .76* .83* .77* .80* .35* .56* .62* .64* .51t .63* .68* .39* Significant Negative Correlations -80* -.62* -.69* -.48t -44t -48t -46t -.44t -72* Nonsignificant Correlations -.12 -.03 .19 -.10 +27 -.16 -.19 -23 -.14 +.26 -.05 Circulation Vol 88, No 6 December 1993 2774 Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 TABLE 2. All Significant Associations of Nutrients and Foods With CHD Mortality After Adjustment for Cholesterol and Saturated Fat (CSI/1000 kcal) for 40 Countries CHD Mortality, r Food or Nutrient .51 * Milk, 9/1000 kcal .44* Butterfat, g/1 000 kcal .58t Calcium from milk, mg/1 000 kcal .41 * Protein from milk, g/1000 kcal .38* Riboflavin, mg/1000 kcal kcal .36* Calcium, mg/1000 -.34* Fat, % kcal -.33* Monounsaturated fat, % kcal Polyunsaturated fat, % kcal -.33* CHD indicates coronary heart disease and CSI, CholesterolSaturated Fat Index. *P<.01; tP<.001; *P<.05. A CHD mortality and alcohol consumption. To examine an interaction between alcohol and dietary fat and cholesterol, we subdivided the 40 countries into those with CSI per 1000 kcal less than 20 and those with CSI per 1000 kcal more than or equal to 20. Partial correlation coefficients were again calculated (adjusting for CSI per 1000 kcal) specifically looking for a relation between alcohol consumption and CHD mortality within each group. All analyses were done using SAS version 6.04 (SAS Institute, Cary, NC). B Results We looked at coronary mortality over time and by sex in France and Finland. In 1977, the mortality from CHD in Finland was three to five times higher than in France. This was true for all age groups for both men and women, even though women in both countries had a lower coronary mortality rate than men (Fig 1). Data from prospective studies have established that the lower coronary mortality in France was not the result of 300 _ 0 Ca5200 a 2000 b. or0 ;;CL 1000 'E 0 40 50 l Finland in) 0 o 0 1- 1000 .0 0 0ID 800 0.0*0 0 L 0 In 0 .;0 =4 O L 0 0 60 600 0 400 00 oX U 1.: c 00 0a 200 France 0. r=0.78 X0 o0 -200 0 15 20 25 10 5 Cholesterol Saturated Fat Index per 1000 kcal/day 0 1200mr t Finland * 1000- 0 0 0 800- to 0 0 o 0% 00 ° 6200- Z0 0CD ~ o 00 C;0200- France 0 / 8P&0 06, 0 0 In$ 0 00 0000 0 0 to 00 0 000 400- r=0.76 0 0 0- 0 0 0 0 in 0 30 0 4 0 0 0 -200~ __1 .50 0 1 100 150 200 250 Milk Intake g per 1000 keal/day 50 300 FIG 2. A, Plot of death rate from coronary heart disease (1977) correlated with daily dietary intake (1976 through 1978) of cholesterol and saturated fat as expressed by the Cholesterol-Saturated Fat Index (CSI) per 1000 kcal. (To convert to amounts per MJ, divide values by 4.184.) The death rate is expressed as deaths per 100000 population for men aged 55 to 64 for 40 countries. CSI was computed from Food and Agriculture Organization Food Balance Sheets. B, Plot of death rate from coronary heart disease correlated with daily milk consumption in grams per 1000 kcal. Finnish men o Finnish women * French men French women * a 1200 CD 60 70 80 Age in years FIG 1. Plot of comparison of coronary heart disease mortalities in France and Finland at different ages in both sexes. The death rate is expressed as deaths per 100 000 population. Values chosen for age are midpoints of each 10-year period as listed in the World Health Organization Annual Vital Statistics. inadequate or incomplete certification of the cause of death.1s Comparable differences in coronary mortality persisted from 1950 through 1987 even though there were changes in the international classification of death from CHD. This dispels the possibility that 1977 was an anomalous year.3 Over a span of 27 years, from 1960 to 1987, the mean ratio of coronary mortality per 100 000 men 55 to 64 years old in Finland versus France was 4.6±0.4 (SD). Between 1961 and the mid 1970s, the Artaud-Wild et al Coronary Mortality in France and Finland 2775 TABLE 3. Consumption of Foods in France, West Germany, the United Kingdom, and Finland Based on Nutrients and Foods That Were Correlated With CHD Mortality After Adjustment for CSI In 40 Countries West France 198 24 Germany 463 United Kingdom 710 24 Finland Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 CHD mortality* 1031 CSIt, per 1000 kcalt 24 26 Food Items§ 74 Milk, g/1000 kcal 69 136 254 Milk protein, g/1000 kcal 7 6 5 12 Butterfat, g/1000 kcal11 12 9 12 18 1 1 Olives, olive oil, peanuts, 3 0.1 peanut oil, g/1 000 kcal¶ Liquid vegetable oils, 8 4 5 1 g/1 000 kcal** Vegetables, g/1000 kcal 81 45 51 19 CHD indicates coronary heart disease and CSI, Cholesterol-Saturated Fat Index. *Per 100 000 men ages 55-64 years.'1 tCholesterol-Saturated Fat Index (CS1).5 *To convert to amounts per MJ, divide by 4.184. §include those with significant correlations with CHD mortality (adjusted for CSI) and vegetables. IlFat from milk, cream, cheese, and butter. ¶Foods containing mostly monounsaturated fats. **Oils containing mostly polyunsaturated fats. coronary mortality rate per 100 000 men rose from 193 to 227 in France and from 837 to 1037 in Finland. For both countries, the rates decreased steadily to a level of 166 for France and 687 for Finland in 1987, but the ratio of mortality between the two countries remained constant during those years. Of the 40 dietary variables considered for the univariate analysis in the 40 countries, 20 dietary variables had significant positive correlations, 9 had significant negative correlations; and 11 had no significant correlations with CHD mortality (Table 1). The variables that had significant positive correlations with CHD mortality generally consisted of animal foods and nutrients associated with animal foods. Significant negative correlations occurred from either plant foods or nutrients found predominantly in plant foods (total carbohydrate, fiber, starch, rice, thiamin, folic acid, and vitamin E). Iron, which is found in both animal and plant foods, was negatively correlated. Calories from vegetable foods were negatively correlated with CHD mortality, whereas calories from animal foods were positively correlated. Alcohol had a significant positive correlation with coronary mortality (r=.35, P=.03), but wine was not significantly correlated (r= -.16, P=.32). When France and Finland were excluded from the analyses, cheese was positively related (r=.35, P=.03) and phosphorus was not related to CHD mortality (r=.30, P=.07). The paradox of the vastly different coronary mortality rates between France and Finland is displayed in Fig 2. The relation between the CSI and CHD mortality (per 100 000 men aged 55 to 64) for all 40 countries is shown in Fig 2A. Countries with CSIs of less than 15 per 1000 kcal had CHD mortality rates of 90 to 190. The Mediterranean countries had CSIs of approximately 15 per 1000 kcal and had CHD mortality rates from 200 to 350. Countries that had CSIs of 24 to 26 per 1000 kcal had very divergent rates of CHD mortality. France had a Ratio Finland/France 5.2 1.1 3.4 2.0 1.5 0.03 0.13 0.23 CSI of 24 per 1000 kcal and a CHD mortality rate of 198. Finland had a CSI of 26 per 1000 kcal and a CHD mortality rate of 1031. Eating styles currently proposed to treat and prevent CHD would have a CSI of 8 to 17 per 1000 kcal.5,14,29.30 The differences in CHD mortality rates between France and Finland could not be explained by their CSIs because they were almost the same. Could they be explained by other dietary factors? The correlation of milk intake with CHD mortality was r=.76 (Fig 2B). Note the new relative positions of France and Finland for CHD mortality rates in relation to milk consumption; these two countries no longer stood apart from the other countries. The difference in milk intakes better explained the differences in CHD mortality for these two countries than did the CSI. Dietary cholesterol and saturated fat were such strong determinants of CHD mortality that they could mask any other dietary effects. When we adjusted for dietary cholesterol and saturated fat intakes for all 40 countries, nine nutrients and foods were significantly associated with CHD mortality (Table 2). Positive associations with CHD mortality included butterfat (fat from milk, cream, cheese, and butter), milk, milk protein, riboflavin, calcium, and calcium from milk. These items were all highly intercorrelated, both before and after adjustment for CSI. Monounsaturated, polyunsaturated, and total fats were negatively associated with CHD mortality. Alcohol was not related to CHD mortality after adjustment for CSI. The strong association of milk and many of its components with CHD mortality, both before and after adjustment for CSI, suggested that something about milk must be strongly related to CHD mortality. This was especially convincing because all variables related to milk except riboflavin were significantly correlated with CSI (r=.75 to .84); yet, they remained significantly correlated with CHD mortality after adjustment for 2776 Circulation Vol 88, No 6 December 1993 Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 CSI. Was it possible to determine the components most likely to be associated with CHD mortality? We then adjusted for CSI and butterfat. Only milk and calcium from milk remained positively associated with CHD mortality. When we adjusted for CSI and milk, only calcium from meat was positively associated with CHD mortality. France and Finland were then excluded, and the analyses adjusting for CSI per 1000 kcal were repeated. Butterfat, riboflavin, calcium, calcium from milk, and meat protein remained positively related to CHD mortality. Then, w-3 fatty acids were inversely related to CHD mortality (r= -.38, P=.02). Milk (r=.30, P=.08) and milk protein (r=.23, P=.18) appeared to have a lesser effect on CHD mortality. To examine the question about the interaction of alcohol and fat intakes with CHD mortality, the 40 countries were divided into two groups: (1) the countries with CSIs of 20 or more per 1000 kcal and (2) the countries with CSIs of less than 20 per 1000 kcal. For the countries with the higher CSIs, the relation of milk and its components and fat and its components with CHD mortality after adjustment for CSI were largely unchanged. The relation of wine (r= -.67, P=.003) and alcohol (r= -.43, P=.09) was strengthened. In addition, cheese was inversely related (r= -.69, P=.002). The interrelation of wine and alcohol was r=.60, P=.01, and for wine and cheese was r=.48, P=.05. The relations of milk and its components with CHD mortality (after adjustment for CSI) were unchanged in the countries with the lower CSIs. The notable exceptions were total fat (r=.02), monounsaturated fat (r= -.06), polyunsaturated fat (r= -.02), to-3 fatty acids (r= -.55, P=.01), wine (r=.18), and alcohol (r=.03). We then looked at differences in the consumption of foods and nutrients that were significantly associated with CHD mortality in the 40 countries after adjustment for CSI. We included France, Finland, and two other countries with similar CSIs -the United Kingdom and West Germany (Table 3). Milk consumption was three times larger in Finland than in France. There was also a larger intake of milk protein and butterfat in Finland. The consumption of liquid vegetable oils, rich in monounsaturated and polyunsaturated fatty acids, was eight times greater in France. The consumption of olives, peanuts, olive oil, and peanut oil was 30 times larger in France than in Finland. The consumption of these foods in the United Kingdom and West Germany was intermediate between those of France and Finland; so were their CHD mortality rates: 463 and 710 per 100 000 men, respectively. Vegetable foods were strongly and negatively correlated with CHD mortality observed on univariate analysis (r= -.80, P<.001). Thus, we examined the consumption of vegetables among the four countries. There was four times greater consumption of vegetables in France than in Finland and intermediate consumptions for the United Kingdom and West Germany. Discussion Dietary cholesterol and saturated fat were clearly important determinants of coronary mortality, as might be expected from the well-known effects of these two variables on plasma lipids, lipoproteins, and coronary disease. However, differences in cholesterol and satu- rated fat intakes, since they were similar, could not explain why Finland has had a four to five times higher CHD mortality rate than France. Only differences in the consumption of other nutrients and foods might help explain this disparity. We were initially surprised that alcohol was positively related to CHD mortality, because of the common perception that the decreased mortality from CHD in France may be ascribed to alcohol intake and, in particular, to the intake of wine.31,32 Also, the results of some epidemiological studies have shown negative associations for moderate intakes of alcohol and positive associations for higher intakes.33-35 Although alcohol was positively associated with CHD mortality univariately, this relation did not remain significant after adjustment for cholesterol and saturated fat. The countries in our study that had the greatest intakes of cholesterol and saturated fat generally had the greatest intakes of alcohol, and the differences in alcohol consumption could not explain the disparity between coronary mortality rates in France and Finland. However, when we considered only the 18 countries with the higher CSIs and adjusted for CSI, a different picture emerged. Wine and alcohol were then inversely and wine was significantly related to CHD mortality. This finding is in keeping with other reports of studies involving similar countries.33-35 The picture is not complete without considering the fact that in the 22 countries with the lower CSIs in which many of the countries had lower intakes of alcohol, neither wine nor alcohol was related to CHD mortality even after adjustment for CSI. Our interpretation of these findings is that wine (containing antioxidants and possibly other beneficial factors) and alcohol may be somewhat protective against CHD mortality when people also consume larger amounts of cholesterol and saturated fat and smaller amounts of plant foods. Nevertheless, when people consume less cholesterol and saturated fat and more plant foods (more antioxidants), drinking wine appears to be unrelated to CHD mortality. This low-CSI, high-plant food pattern is similar to the eating style proposed to protect people, nutritionally, against coronary disease.5,14,29,30 There were striking differences between France and Finland in the consumption of major classes of foods and nutrients that this study showed to be significantly associated with CHD mortality after adjustments for cholesterol and saturated fat in the 40 countries: they were milk, butterfat, monounsaturated and polyunsaturated fats, and, finally, vegetables. Milk and butterfat were associated with a higher coronary mortality rate, and plant foods containing the unsaturated fats and vegetables were associated with a lower coronary mortality rate. Milk intake was 3.5 times greater in Finland than in France. The analyses showed that several of the constituents of milk (butterfat, protein, calcium, etc.) were strongly associated and suggested that milk must be related in some way to CHD mortality. There are scattered epidemiological, animal, and human studies about constituents in milk and coronary disease. Causal inferences cannot be made from these few studies. Turpeinen36 previously showed a correlation between dairy fat and CHD mortality rates (r=.75) for 22 industrialized countries. There was a positive correla- Artaud-Wild et al Coronary Mortality in France and Finland Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 tion (r=.78) between coronary mortality rates and the consumption of dairy fat (excluding fat from cheese) in 19 countries reported by Renaud and de Lorgeril.37 In our study of 40 countries, the correlation coefficients between coronary mortality and the consumption of butterfat including or excluding cheese fat were comparable: r=.80 versus r=.79. Joossems and colleagues38 found a distinct difference in CHD mortality between southern Belgium and northern Belgium. In southern Belgium, butterfat consumption was far lower than in northern Belgium. The coronary mortality was lower in southern Belgium.38 Likewise, France had a contrasting pattern of cultures regarding food. Butter consumption was high in the northern regions such as Moselle, where the incidence of cardiovascular disease was high.37 Olive oil was the chief fat consumed in southern France (along with some peanut oil), and the cardiovascular disease incidence was low in the South of France, department of Var.39 In experimental animals, butterfat has been the fat par excellence that produced thrombosis, a major event in coronary disease. The experiments of Thomas and Hartroft4O and Hornstra41 in rats demonstrated that butterfat in the diet induced myocardial infarction from the thrombotic obstruction of coronary arteries without much atherosclerosis. Impairment of fibrinolysis from butterfat has also occurred in humans.42 The aggregating activity of platelets has been shown to be directly related to the intake of saturated fatty acids (12 to 18 carbon atoms in length) in free living populations.43 Saturated fatty acids constitute more than 50% of total fatty acids in butterfat. The potential of butterfat to increase the arachidonic acid content of platelets in rabbits may be a significant factor in its thrombogenic effect since arachidonic acid is a precursor to thromboxane A2.44 Similarly, soft atherosclerotic plaques, which are more inclined to rupture and thrombose, developed in monkeys and rabbits fed butterfat.45 Therefore, the high CHD mortality observed in Finland might have been related to two factors: (1) the hypercholesterolemic and atherogenic effect of the cholesterol and saturated fat in milk and (2) the thrombotic tendency produced by the saturated fat in milk. As for milk protein, there are studies showing that casein was hypercholesterolemic in animals compared with soy protein.46 However, the positive correlation of milk protein with CHD mortality was no longer significant after adjusting for the combination of cholesterol, saturated fat, and butterfat in the 40 countries. The correlation remained positive for milk per se. The high intake of milk in Finland as shown in Table 3 may have been contributory to CHD; France had a low intake of milk. France had a higher consumption of olives, olive oil, peanuts, and peanut oil than Finland; its position was close to that of the other Mediterranean countries that consumed substantial amounts of monounsaturated fatty acids and had relatively low rates of CHD mortality. In most epidemiological studies,15-17'47 including the present one, monounsaturated fat was positively associated with coronary mortality using univariate analysis. However, in metabolic studies, monounsaturated fatty acids have an LDL cholesterol-lowering effect similar to that of polyunsaturated fatty acids but without a corresponding lowering of high-density lipoprotein choles- 2777 terol when substituted for saturated fatty acids48'49 or complex carbohydrates.50'51 After adjusting for saturated fat and cholesterol, as we have done in our analyses, there was a significant negative association of monounsaturated fat with CHD mortality. Keys and colleagues in the Seven Countries Study also showed, with multiple regression analyses, that the CHD death rate was negatively correlated with the percentage of calories from monounsaturated fatty acids.52 The consumption of polyunsaturated fatty acids contained in liquid vegetable oils was eight times larger in France than in Finland. However, most epidemiological studies have not shown a significant inverse correlation between polyunsaturated fat consumption and CHD mortality rates.15-17'47 Metabolic studies have shown that polyunsaturated fat in the diet has a plasma total and LDL cholesterol-lowering effect49 and that it tends to prevent thrombosis,5354 thus potentially providing a protective role against CHD. The narrow range of polyunsaturated fat intakes the world over and the overwhelming influence of cholesterol and saturated fat may mask any significant connection between this nutrient and coronary mortality. In our study, however, the negative correlation between polyunsaturated fat and CHD mortality was significant after adjusting for cholesterol and saturated fat intakes. This observation may help account for the divergent rates of CHD mortality. There was a marked difference between the consumption of liquid vegetable oils between France and Finland. Interestingly, West Germany and the United Kingdom occupy intermediate positions with regard to both consumption of liquid vegetable oils and coronary mortality. The consumption of w-3 fatty acids from seafood was related to coronary disease in Greenland Eskimos, the Dutch, and the Japanese.55-57 In our study, the amount of dietary co-3 fatty acids had an inverse relation to CHD mortality in 38 countries (France and Finland excluded). This same relation occurred in the 22 countries with CSIs less than 20 per 1000 kcal. For the 40 countries, calories from animal foods correlated positively with CHD mortality rates, r=.79 (P<.001), and calories from vegetable foods correlated negatively, r= -.80 (P<.001); this replicates earlier findings.10 We also found that, generally, nutrients associated with animal foods correlated positively with CHD mortality rates, whereas nutrients associated with vegetable foods and vegetable oils correlated negatively. These results are in accordance with earlier international data using assorted food commodities and CHD mortality.15'16'47 Diets high in cereals, legumes, and vegetables have been consistently associated with low plasma cholesterol levels and a low incidence of CHD. Keys reported, "Fruits and vegetables other than roots and tubers are much more prominent in the average diets in Italy and Greece than in those of Finland, the Netherlands, and the United States."2 This has been shown in populations as diverse as American vegetarians,59-61 Japanese,62'63 the Tarahumara Indians of Mexico,64 or the Ugandans of East Africa.65 Some support for a cardiovascular protective role of vegetable foods comes from clinical trials and feeding studies as well.66-68 Our data suggest that the higher consumption of vegetables in France may also have helped to account for a lower CHD mortality rate compared with Finland. 2778 Circulation Vol 88, No 6 December 1993 Factors in plants that might be protective have not been fully identified but could include soluble fiber,69 saponins,70 and antioxidants.71,72 Soluble fiber promotes plasma cholesterol lowering by binding bile acids in the gut and promoting their excretion in the stool.69 Saponins block absorption of cholesterol.70 Antioxidants such as beta carotene, ascorbic acid, a-tocopherol, and phenolic compounds could help prevent LDL from becoming oxidized; the strong atherogenicity of oxidized LDL has been demonstrated.71-73 A recent study suggests that CHD mortality rates in middle-aged men from 16 European countries were inversely related to plasma vitamin E levels.74 Summary and Conclusions Differences in coronary mortality rates the world could largely be explained by differences in dietary cholesterol and saturated fat intakes. However, the difference in coronary mortality rates between France and Finland has, over many decades, puzzled scientists because both have had similar intakes of cholesterol and saturated fat. This paradox led us to take as broad a look as possible at other dietary factors and CHD mortality. Our study of 40 countries suggested that disparate CHD mortality rates could be partly explained in 1977 by intakes of milk, butterfat, and vegetable foods (particularly, vegetable oils and vegetables). The greater consumption of vegetable foods in France compared with Finland illustrated that point. Current scientific evidence gives credence to these associations in 1993, although further studies are needed to test the hypotheses suggested by this study. Finally, this study has stressed that the association of dietary factors with CHD mortality is very complex, and differences in coronary mortality cannot be ascribed to one nutrient or to one food only. It is necessary to consider the total diet. over Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 Acknowledgments This study was supported by research grants HL-20910, HL-37940, and DK-40566 (Clinical Nutrition Research Unit) and RR-334 (Clinical Research Center), all from the National Institutes of Health. References 1. Bronte-Stewart B. The effect of dietary fats on the blood lipids and their relation to ischemic heart disease. Br Med Bull. 1958;14: 243-252. 2. Keys A, with 15 collaborators. Seven Countries-A Multivariate Analysis of Death and Coronary Heart Disease. A Commonwealth Fund Book. Cambridge, Mass: Harvard University Press; 1980: 1-381. 3. Connor WE. Dietary cholesterol and the pathogenesis of atherosclerosis. Geriatrics. 1961;16:407-415. 4. Liu K, Stamler J, Trevisan M, Moss D. Dietary lipids, sugar, fiber, and mortality from coronary heart disease-bivariate analysis of international data. Atherosclerosis. 1982;2:221-227. 5. Connor SL, Gustafson JR, Artaud-Wild SM, Flavell DP, Classick-Kohn CJ, Hatcher LF, Connor WE. The cholesterol/ saturated fat index: an indication of the hypercholesterolaemic and atherogenic potential of food. Lancet. 1986;1:1229-1232. 6. Ducimetiere P, Richard JL, Cambien F, Rakotovao R, Claude JR. Coronary heart disease in middle aged Frenchmen, comparison between Paris Prospective Study, Seven Countries Study and Pooling Project. Lancet. 1980;2:1346-1350. 7. Richard JL, Cambien F, Ducimetiere P. Particularites epidemiologiques de la maladie coronarienne en France. La Nouvelle Presse Med. 1981;10:1111-1114. Editorial. 8. Bang HO, Dyerberg J, Hjorne N. The composition of foods consumed by Greenland Eskimos. Acta Med Scand. 1976;200: 69-73. 9. Bang HO, Dyerberg J. Plasma lipids and lipoproteins in Greenlandic West Coast Eskimos. Acta Med Scand. 1972;192:85-94. 10. Connor WE, Connor SL. The key role of nutritional factors in the prevention of coronary heart disease. Prev Med. 1972;1:49-83. 11. World Health Organization. World Health Statistics Annuals 1977. Geneva, Switzerland: WHO; 1980. 12. Manual of the Statistical Classification of Diseases, Injuries and Causes of Death, Ninth Revision, Vol 1. Geneva, Switzerland: 1981: 746-755. 13. Food and Agricultural Organization of the United Nations. Food Balance Sheets and per Caput Food Supplies. Rome, Italy: 1980: 1967-1977. 14. The Surgeon General's Report on Nutrition and Health. Washington, DC: US Department of Health and Human Services; DHHS publication No. (PHS)88-50210, 1988. 15. WHO Monica Project Principal Investigators. The World Health Organization Monica Project (monitoring of trends and determinants in cardiovascular disease): a major international collaboration. J Chron Dis. 1988;41:105-114. 16. Stamler J. Population studies. In: Levy R, Rifkind B, Dennis B, Ernst N, eds. Nutrition, Lipids, and Coronary Heart Disease: A Global View. New York: Raven Press; 1979:25-88. 17. Byington R, Dyer AR, Garside D, et al. Recent trends of major coronary risk factors and coronary heart disease mortality in the United States and other industrialized countries. In: Havlik RJ, Feinleib M, eds. Proceedings of the Conference on the Decline in Coronary Heart Disease. US Department of Health Education and Welfare; PHS, NIH (DHEW publication No. 79-1610); 1979. 18. Dennis B, Ernst N, Hjortland M, Tillotson J, Grambsch V. The NHLBI Nutrition Data System. JAm Diet Assoc. 1980;77:641-647. 19. Food Table Version 13.0. NHLBI Database. Nutrition Coordinating Center (NCC). Minneapolis: University of Minnesota, 1986. 20. Hegsted DM, McGandy RB, Myers ML, Stare FJ. Quantitative effects of dietary fat on serum cholesterol in man. Am J Clin Nutr. 1965;17:281-295. 21. Keys A, Anderson JT, Grande F. Serum cholesterol response to changes in the diet. 1-5. Metabolism. 1965;14:747-787. 22. Grande F. Predicting change in serum cholesterol from change in composition of the diet. In: Lauer RM, Shekelle RB, eds. Childhood Prevention of Atherosclerosis and Hypertension. New York: Raven Press; 1980:145-153. 23. Brown MS, Goldstein JL. A receptor-mediated pathway for cholesterol homeostasis. Science. 1986;232:34-47. 24. Spady DK, Dietschy M. Interaction of dietary cholesterol and triglycerides in the regulation of hepatic low density lipoprotein transport in the hamster. J Clin Invest. 1988;81:300-309. 25. Connor WE, Witiak DT, Stone DB, Armstrong ML. Cholesterol balance and fecal neutral steroid and bile acid excretion in normal men fed dietary fats of different fatty acid composition. J Clin Invest. 1969;48:1363-1375. 26. Niter J, Wasserman W, Kutner MH. Applied Linear Regression Models. Homewood, Ill: Richard D Irwin; 1983. 27. Cohen J, Cohen P.Applied Multiple Regression Correlation Analysis for Behavioral Sciences. 2nd ed. Hillsdale, NJ: Lawrence Erlbaum Assoc; 1983. 28. World Health Organization. World Health Statistics Annuals 1977 Through 1988. Geneva, Switzerland. 29. National Research Council. Diet and Health, Implications for Reducing Chronic Disease Risk. Washington, DC: National Academy Press; 1989. 30. National Cholesterol Education Program. Report of the Expert Panel on Population Strategies for Blood Cholesterol Reduction. US Department of Health and Human Services, NIH publication No. 90-3046, 1990. 31. Renaud S, de Lorgeril M. Wine, alcohol, platelets and the French paradox for coronary heart disease. Lancet. 1992;339:1523-1526. 32. St Leger AS, Cochrane AL, Moore F. Factors associated with cardiac mortality in developed countries with particular reference to the consumption of wine. Lancet. 1979;1:1017-1020, 1294. 33. Marmot M, Brunner E. Alcohol and cardiovascular disease: the status of the U shaped curve. BMJ. 1991;303:565-568. 34. Moore RD, Pearson TA. Moderate alcohol consumption and coronary artery disease: a review. Medicine. 1986;65:242-267. 35. Hegsted DM, Ausman LM. Diet, alcohol and coronary heart disease in men. JNutr. 1988;118:1184-1189. 36. Turpeinen 0. Effect of cholesterol-lowering diet on mortality from coronary heart disease and other causes. Circulation. 1979;59:1-8. Artaud-Wild et al Coronary Mortality in France and Finland Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 37. Renaud S, de Lorgeril M. Dietary lipids and their relation to ischaemic heart disease: from epidemiology to prevention. J Intern Med. 1989;225:1-8. 38. Joossens JV, Brems-Heyns E, Claes JH, et al. The pattern of food and mortality in Belgium. Lancet. 1977;1:1069-1072. 39. Statistiques des causes medicales de deces. INSERM. Tome II. Resultats par region. 1972;187:327. 40. Thomas W, Hartroft W. Myocardial infarction in rats fed diets containing high fat, cholesterol, thiouracil, and sodium cholate. Circulation. 1959;19:65-72. 41. Hornstra G. Dietary lipids, platelet function and arterial thrombosis in animals and man. Proc Nutr Soc. 1985;44:371-378. 42. Merigan TC, Farquhar JW, Williams JH, Sokolone M. Effect of chylomicrons on the fibrinolytic activity of normal human plasma in vitro. Circulation. 1959;7:205-209. 43. Renaud S, Morazain R, Godsey F, et al. Nutrients, platelet function and composition in nine groups of French and British farmers. Atherosclerosis. 1986;60:37-48. 44. Berlin E, Shapiro SG, Kliman PG. Influence of saturated and unsaturated fats on platelet fatty acids in cholesterol-fed rabbits. Atherosclerosis. 1987;63:85 -96. 45. Vesselinovitch D, Getz GS, Hughes RH, Wissler RW. Atherosclerosis in the rhesus monkey fed three food fats. Atherosclerosis. 1974;20:303-321. 46. Kurowska EM, Carroll KK. Essential amino acids in relation to hypercholesterolemia induced in rabbits by dietary casein. J Nutr. 1990;120:831-836. 47. Stamler J, Stamler R, Shekelle RB. Regional differences in prevalence, incidence and mortality from atherosclerotic coronary heart disease. In: deHaas JH, Hemker HC, Snellen HA, eds. Ischaemic Heart Disease. Leiden, The Netherlands: Leiden University Press; 1970;84. 48. Becker N, Illingworth DR, Alaupovic P, Connor WE, Sundberg EE. Effects of saturated, monounsaturated and n-6 polyunsaturated fatty acids on plasma lipids, lipoproteins and apoproteins in humans. Am J Clin Nutr. 1983;37:355-360. 49. Mattson FH, Grundy SM. Comparison of effects of dietary saturated, monounsaturated, and polyunsaturated fatty acids on plasma lipids and lipoproteins in man. JLipid Res. 1985;26:194-202. 50. Grundy SM. Comparison of monounsaturated fatty acids and carbohydrates for lowering plasma cholesterol. N EngI J Med. 1986; 314:745-748. 51. Mensink RP, Katan MB. Effect of monounsaturated fatty acids versus complex carbohydrates on high density lipoproteins in healthy men and women. Lancet. 1987;1:122-125. 52. Keys A, Menotti A, Karvonen M, et al. The diet and 15-year death rate in the Seven Countries Study. Am J Epidemiol. 1986;124: 903-915. 53. Hornstra G, Lewis B, Chait A, Turpeinen 0, Karvonen MJ, Vergroesen AJ. Influence of dietary fat on platelet function in men. Lancet. 1973;1:1155-1157. 54. Goodnight SJ Jr, Harris WS, Connor WE, Illingworth DR. Polyunsaturated fatty acids, hyperlipidemia, and thrombosis. Arteriosclerosis. 1982;2:87-113. 55. Kromann N, Green A. Epidemiological studies in the Upernavik district, Greenland: incidence of some chronic diseases 1950-1974. Acta Med Scand. 1980;208:401-406. 2779 56. Kromhout D, Bosschieter EB, Coulander CdeL. The inverse relation between fish consumption and 20-year mortality from coronary heart disease. N Engl J Med. 1985;312:1205-1209. 57. Kazawa Y, Niskizawa M, Suzuki M, et al. Eicosapentaenoic acid of serum lipids of Japanese islanders with low incidence of cardiovascular diseases. J Nutr Sci Vitaminol. 1982;28:441-453. 58. Brown VW, Karmally W. Coronary heart disease and the consumption of diets high in wheat and other grains. Am J Clin Nutr. 1985;41:1163-1171. 59. Hardinge MG, Stare FJ. Nutritional studies of vegetarians, II: dietary and serum levels of cholesterol. Am J Clin Nutr. 1954;2: 83-88. 60. Burslem J, Schonfeld G, Howard MA, Weidman SW, Miller JP. Plasma apoprotein and lipoprotein lipid levels in vegetarians. Metabolism. 1987;27:711-719. 61. Sacks FM, Castelli WP, Donner A, Kass EH. Plasma lipids and lipoproteins in vegetarians and controls. N Engl J Med. 1975;292: 1148-1151. 62. Kagan A, Harris BR, Winkelstein W Jr. Epidemiologic studies of coronary heart disease and stroke in Japanese men living in Japan, Hawaii and California: demographic, physical, dietary and biochemical characteristics. J Chron Dis. 1974;27:345-364. 63. Worth RM, Kato H, Rhoads GG, Kagan S, Syme SL. Epidemiologic studies of coronary heart disease and stroke in Japanese men living in Japan, Hawaii and California: mortality. Am J Epidemiol. 1975;102:481-490. 64. Connor WE, Cerqueira MT, Connor RW, Wallace RB, Malinow MR, Casdorph HR. The plasma lipids, lipoproteins and diet of the Tarahumara Indians of Mexico.Am J Clin Nutr. 1978;31:1131-1142. 65. Shaper AG, Jones KW. Serum cholesterol, diet and coronary heart disease in Africans and Asians in Uganda. Lancet. 1959;2:534. 66. Arntzenius AC, Kromhout D, Barth JD, et al. Diet, lipoproteins and the progression of coronary atherosclerosis: the Leiden Intervention Trial. N Engl J Med. 1985;312:805-812. 67. Sirtori CR, Agradi E, Conti F, Mantero 0. Soybean protein diet in the treatment of Type II hyperlipoproteinemia. Lancet. 1977;1: 275-277. 68. Ornish D, Brown SE, Scherwitz LW, et al. Can lifestyle changes reverse coronary heart disease? Lancet. 1990;336:129-133. 69. Anderson JW, Chen W, Sieling B. Hypolipidemic effect of high carbohydrate, high fiber diet. Metabolism. 1980;29:551-558. 70. Malinow MR, Connor WE, McLaughlin P, et al. Sterol balance in Macaca fascicularis: effects of alfalfa saponins. J Clin Invest. 1981; 67:156-162. 71. Luc G, Fruchart JC. Oxidation of lipoproteins and atherosclerosis. Am J Clin Nutr. 1991;53:206S-209S. 72. Frankel EN, Kanner J, German JB, Parks E, Kinsella JE. Inhibition of oxidation of human low-density lipoprotein by phenolic substances in red wine. Lancet. 1993;341:454-457. 73. Esterbauer H, Dieber-Rotheneder M, Striegl G, Waeg G. Role of vitamin E in preventing the oxidation of low density lipoprotein. Am J Clin Nutr. 1991;53:314S-321S. 74. Gey FK, Puska P, Jordan P, Moser UK Inverse correlation between plasma vitamin E and mortality from ischemic heart disease in cross-cultural epidemiology. Am J Clin Nutr. 1991;53: 326S-334S. Differences in coronary mortality can be explained by differences in cholesterol and saturated fat intakes in 40 countries but not in France and Finland. A paradox. S M Artaud-Wild, S L Connor, G Sexton and W E Connor Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 Circulation. 1993;88:2771-2779 doi: 10.1161/01.CIR.88.6.2771 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1993 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/88/6/2771 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/