Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
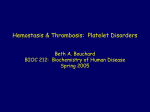
Platelet Glycoprotein IIb/IIIa Inhibitors Basic and Clinical Aspects Alan T. Nurden, Christel Poujol, Catherine Durrieu-Jais, Paquita Nurden G Downloaded from http://atvb.ahajournals.org/ by guest on May 2, 2017 recovery of platelet function is gradual after the infusion is stopped. Whereas plasma levels quickly fall, platelet-bound abciximab can be detected for up to 15 days after treatment. Flow cytometry shows that histograms representing bound drug within the total platelet population remain homogeneous while decreasing in intensity.5 EPIC6 and EPILOG7 trials, among others, showed a beneficial effect of sustained blockade of the GPIIb-IIIa receptor by abciximab in patients undergoing high-risk percutaneous transluminal coronary angioplasty (PTCA) or directional coronary atherectomy. The effect was defined in EPIC as a 35% relative risk reduction of death, myocardial infarction, or urgent revascularization within 30 days. An extended follow-up has since shown that abciximab also improves the probability of event-free survival over a long period.8 Although the risk of excessive bleeding was highlighted in the EPIC trial, weight-adjusted heparin dosing and early sheath removal in subsequent trials led to improved safety.7,9 The occasional need for emergency coronary bypass surgery is helped by the rapid clearance of abciximab from plasma, and platelet transfusion will provide functional platelets, lower the free plasma levels of the drug further, and promote the antibody exchange that has been suggested to occur between circulating platelets.5 Abciximab also substantially improves the safety of coronary stenting, now used in .60% of percutaneous revascularization procedures in the United States.10 Stenting can itself promote GPIIb-IIIa complex activation and predispose to coronary thrombus formation. The combination of aspirin and ticlopidine inhibits the thromboxane A2 and ADP-dependent pathways of platelet activation11 (Figure). However, multiple intracellular pathways appear to be involved in platelet activation, and these include serine and threonine phosphorylation of proteins by protein kinase C and phosphorylation of tyrosine residues on proteins by tyrosine kinase enzymes.3 However, different agonists use different pathways, and by blocking the end step of platelet aggregation common to all physiological agonists, anti–GPIIb-IIIa drugs provide a theoretically wider range of protection. GPIIb-IIIa inhibition is also now often considered as part of a last resort “rescue” therapy in the case of abrupt coronary occlusion or the failure of PTCA to restore the circulation.12 The concept is that this facilitates the dispersion of platelet-rich thrombi in difficult lycoprotein IIb/IIIa (GPIIb-IIIa) complexes (integrin aIIbb3) mediate platelet aggregation by binding fibrinogen or von Willebrand factor (vWF), protein cofactors that form bridges between adjacent platelets. The cross-linked adhesive proteins assemble platelets into the aggregate. Agents that block the function of the GPIIb-IIIa complex of platelets constitute a powerful new generation of antithrombotic drugs.1 Among the short- and long-term aims of such drugs are (1) to provide immediate relief in the case of ongoing arterial thrombosis and (2) to eliminate excessive platelet reactivity in diseased vessels so that occlusive thrombi and restenosis do not occur, while allowing sufficient hemostasis to prevent spontaneous bleeding. It should be emphasized that stenosis and partial occlusion are both prothrombotic, with increased shear stress promoting platelet activation. Under these conditions, vWF plays a major role in the mediation of thrombus formation, interacting with GPIIbIIIa and the adhesion receptor GPIb.2 Otherwise, fibrinogen is the major cofactor of platelet aggregation, essentially binding through a dodecapeptide sequence (aa400 to aa411) present at the carboxy terminus of each g chain. Binding of vWF and other adhesive proteins, such as fibronectin, to GPIIb-IIIa is mediated by the Arg-Gly-Asp (RGD) sequence, a universal mediator of cellular interactions with the extracellular matrix.1–3 Anti–GPIIb-IIIa drugs block this final step of the platelet aggregation process. They also block the “outside-in” signaling that follows the binding of adhesive proteins to activated GPIIb-IIIa and the onset of platelet aggregation.3 This signaling may promote events such as secretion, clot retraction, and the expression of procoagulant activity; therefore, its inhibition extends the influence of anti–GPIIb-IIIa drugs beyond the blocking of platelet-to-platelet cohesion. GPIIb-IIIa Inhibitors Constitute a Wide Class of Drugs The present review will mostly be illustrated by results obtained with abciximab (c7E3 Fab, ReoPro), a chimeric antibody fragment that is the most widely used of the new inhibitors.1 Abciximab acts rapidly; .80% of platelet receptors are blocked within 2 hours of the administration of a 0.25 mg/kg bolus in humans.4 Saturation is maintained during a 10-mg/min infusion (mostly between 12 and 24 hours), and Received February 25, 1999; revision accepted April 28, 1999. From the UMR 5533 CNRS and the Unité des Soins Intensifs (C.D.-J.), Institut Fédératif de Recherche “Cœur-Vaisseaux-Thrombose,” Hôpital Cardiologique, Pessac, France. Correspondence to Alan T. Nurden, Director, UMR 5533 CNRS, Hôpital Cardiologique, 33604 Pessac, France. E-mail Alan.Nurden@ cnrshl.u-bordeaux2.fr (Arterioscler Thromb Vasc Biol. 1999;19:2835-2840.) © 1999 American Heart Association, Inc. Arterioscler Thromb Vasc Biol. is available at http://www.atvbaha.org 2835 2836 Arterioscler Thromb Vasc Biol. December 1999 Downloaded from http://atvb.ahajournals.org/ by guest on May 2, 2017 Schematic diagram showing the target for GPIIb-IIIa inhibitors. Platelet activation can be initiated by adhesion to immobilized substrates in the vessel wall or to a fibrin clot or by soluble agonists such as ADP and thrombin. Antiplatelet therapies can target individual receptor-linked activation pathways. For example, ticlopidine and clopidogrel act on an ADP-induced activation pathway. Aspirin dampens the platelet response by inactivating cyclooxygenase enzyme (Cox-1) and preventing thromboxane A2 (TXA2) formation. GPIIb-IIIa inhibitors block the final step of platelet aggregation common to all agonists, the binding of fibrinogen or vWF to activated GPIIb-IIIa complexes. Such inhibitors include an antibody, abciximab (c7E3 Fab fragments), a cyclic peptide (eptifibatide), and 2 peptidomimetics (lamifiban and tirofiban), all of which require intravenous injection (left side of Figure). Orally bioavailable inhibitors include xemilofiban, DMP 802, and SR 121787 (right side of Figure). These are just selected examples of the anti-integrin therapies being tested. cases by tissue plasminogen activator or even by PTCA by halting the incorporation of incoming platelets. However, the association of abciximab or other anti–GPIIb-IIIa agents with powerful anticoagulants or with thrombolytics increases the risk of bleeding. The fabrication of synthetic small-molecule inhibitors (some are called peptidomimetics because they mimic RGD peptides) designed for intravenous administration, such as eptifibatide (integrelin), lamifiban, and tirofiban, means that alternative anti–GPIIb-IIIa therapies are now available.13–15 Eptifibatide is a small cyclic heptapeptide, and lamifiban and tirofiban are nonpeptide peptidomimetics. These compounds, which circulate for shorter times than does abciximab, have also been found to be beneficial in acute situations, such as after PTCA or stenting. Another family of synthetic inhibitors, such as xemilofiban, DMP 802, and SR 121787, may be taken orally and are being assessed for long duration use in patients with coronary artery disease who are considered vulnerable for major thrombotic episodes.16 –18 This latter group consists mostly of prodrugs that are biologically transformed into active metabolites. However, it remains to be seen whether safety parameters will allow their use chronically, in view of the fact that some compounds have already been withdrawn because of a higher than acceptable bleeding risk and/or thrombocytopenia (see below). Another concern is that the apparent potency of some smallmolecular-mass GPIIb-IIIa antagonists can be enhanced by citrate and that microaggregates can still often be detected by platelet counting, thus hampering the interpretation of drug efficacy in in vitro tests.19 Effects on Circulating Platelet Count Thrombocytopenia is an often-cited complication of the use of GPIIb-IIIa receptor antagonists. In one study, it has recently been estimated that profound thrombocytopenia (,203109/L) during abciximab therapy affects '0.5% of patients.20 Often, though, administration of the drug is interrupted before such low counts are reached. The mechanisms responsible for the thrombocytopenia are not known, although different causes may be evoked. With abciximab, one possible explanation involves naturally occurring antibodies that recognize epitopes on mouse IgG still present on the chimeric Fab fragments. The binding of immune complexes to platelets will be followed by their clearance by way of the reticuloendothelial system and the spleen. The pressure for the repeated use of abciximab will increase as the previously treated patient is confronted with more problems later, and anaphylaxis could yet become a more important worry. Another explanation for the thrombocytopenia is that host immunoglobulins could recognize neoepitopes expressed on GPIIb-IIIa after a drug has bound (the so-called ligandinduced binding sites).21 Such a mechanism could explain the rapid thrombocytopenia induced by small-molecular-mass inhibitors of GPIIb-IIIa, including the orally bioavailable drugs. Another relevant question is whether anti–GPIIb-IIIa drugs can penetrate into the marrow and interfere with thrombopoiesis. We have looked for abciximab in the sternal marrow aspirate of a patient who received a bolus followed by a 10-mg/mL infusion for 3 hours before the stopping of therapy because of bleeding. Thrombocytopenia was noted, and this continued to develop (C. Poujol, C. Durrieu-Jais, B. Larrue, A.T. Nurden, P. Nurden, unpublished data, 1999). At 15 hours, the time at which the marrow cells were obtained, proplatelet fragments in the vascular sinuses were heavily labeled with abciximab, but megakaryocytes within the marrow were only weakly labeled. Thus, it would seem unlikely that abciximab penetrates into the marrow in such quantities to interfere with megakaryocyte maturation and stem cell proliferation, and certainly, this would not bring about major falls in platelet count within 24 hours. Nevertheless, marrowrelated changes must remain a major concern for prolonged therapy with small-molecular-mass inhibitors. There is abundant evidence pointing to a role for RGD-binding integrins during hematopoiesis and angiogenesis. Recently, accutin, a 5-kDa snake venom disintegrin that blocks GPIIb-IIIa and binds competitively with c7E3 for avb3 on human umbilical cord endothelial cells, has been shown to inhibit angiogenesis and to induce apoptotic fragmentation of endothelial cells.22 Similar results have been obtained for other RGD peptides.23 These findings imply caution in the long-term use of RGDbased drugs, while confirming a potential role for them as antimetastatic agents. Effect on Platelet Activation Platelet activation is known to occur episodically in coronary syndromes, and elevated levels of circulating activated platelets, as detected by flow cytometry, have been said to be predictive for increased risk of acute ischemic events after PTCA or stenting, although the interpretation of such measurements remains controversial.24,25 We have recently compared the expression of activation-dependent markers on platelets during abciximab therapy given according to the CAPTURE protocol9 to patients with unstable angina undergoing PTCA.26 Before the onset of therapy, the percentage of Nurden et al Downloaded from http://atvb.ahajournals.org/ by guest on May 2, 2017 platelets positive for one or more of the monoclonal antibodies directed against GPIIb-IIIa complexes that are “activated and unoccupied” (PAC-1) or “activated and occupied with fibrinogen” (AP6 and F26) were elevated for 5 of 6 patients studied. Abciximab therapy reduced these levels appreciably, presumably through the blockade of the active site of GPIIbIIIa. Testing of samples taken after the bolus and 3 hours into the infusion confirmed that for most patients near-maximal inhibition of platelet aggregation was already achieved. This inhibition continued during the duration of the abciximab infusion (up to 24 hours). However, for one patient, a residual irreversible aggregation response was seen with ADP. Interestingly, it was for this patient that activation-dependent markers on GPIIb-IIIa continued to be detected, suggesting continued platelet hyperactivity and a resistance to abciximab. Peter et al27 have recently shown that the binding of abciximab itself induced conformation changes in GPIIb-IIIa and, in so doing, mimicked the changes previously shown for some RGD peptides. According to these authors, the changes were such that when abciximab dissociated from the complex, a process facilitated in their experimentation by the large-scale dilution of the platelet suspensions, fibrinogen was able to bind without the normal requirement for platelet stimulation by an agonist. Peter et al27 also showed that 2 small-molecular-mass inhibitors were able to activate GPIIbIIIa but that aspirin prevented “aggregation” induced by the anti–GPIIb-IIIa drugs. Further studies are required to confirm that such events occur in vivo and to determine whether this can lead to clinical drawbacks. In our previous study,26 activated platelets progressively reappeared in the circulation after the stopping of the abciximab, but this can be due to the fact that the cause of increased platelet stimulation had not been removed (eg, fissured atherosclerotic plaques, stenosis, and resistant fibrin-rich thrombi). Intersubject heterogeneity in the extent and duration of inhibition of platelet aggregation has been previously shown in patients with coronary artery disease receiving abciximab.4,9,26 Among the other factors that may influence the recovery rate after anti–GPIIb-IIIa therapy are (1) variations in the plasma levels of free drug, (2) the rate at which surface-bound drug dissociates from circulating platelets,5 and (3) the extent to which GPIIb-IIIa receptors are exchanged between surface and internal pools.28 Therefore, it is reasonable to suggest that biological surveillance, with testing of platelet function and flexibility with regard both to the doses used and the duration of therapy, may help to improve the success rate with anti–GPIIb-IIIa inhibitors in acute situations. This may also be so with orally bioavailable drugs that are used chronically and for which the degree of sustained receptor inhibition may be lower.16 –18 Internal Pools of GPIIb-IIIa and Trafficking of Abciximab Although ADP-induced platelet aggregation was extensively inhibited by abciximab in our previous study,26 platelet responses to thrombin receptor–activating peptide (14mer) during abciximab infusion ranged from 28% to 71% of pretreatment levels. Similar results have previously been reported for patients after a single bolus injection of abciximab.29 Estimates suggest that between 35 000 and 100 000 Anti–GPIIb-IIIa Therapy 2837 copies of GPIIb-IIIa are to be found on the surface of resting platelets and that a pool of similar proportions is to be found inside the platelet (data reviewed in Reference 30). Using the monoclonal antibody AP-2, competitive for GPIIb-IIIa with c7E3, in flow cytometry or immunoelectron microscopy, we have shown that unblocked (with abciximab) GPIIb-IIIa receptors from the internal pool do indeed become exposed after thrombin stimulation of platelets taken from patients during abciximab infusion.26 A residual aggregation with thrombin receptor–activating peptide during the infusion and after the administration of the abciximab bolus suggests that the concentration of free abciximab in plasma is insufficient to block these newly exposed receptors within the time scale of platelet aggregation, which will occur in seconds. The ability of peptides, peptidomimetics, and orally bioavailable drugs to inhibit aggregation with strong agonists will therefore depend on their affinity for GPIIb-IIIa and their sustained concentration in plasma. Furthermore, some GPIIb-IIIa complexes of the internal pool may be surface-expressed with the already active site occupied with fibrinogen being secreted from a-granules, as has been shown for platelets stimulated in vitro with thrombin.21 The ability of anti–GPIIb-IIIa drugs to gain access to internal pools of GPIIb-IIIa complexes of circulating platelets is therefore an important question to address. We have examined the trafficking of abciximab within platelets at different time points during therapeutic infusion by immunoelectron microscopy using a rabbit antibody specific for c7E3.31 It appears that abciximab gains access to the internal membrane subpopulations of GPIIb-IIIa by 2 mechanisms: (1) through thin channels of the surface-connected canalicular system and (2) by way of clathrin-coated pits and endocytosis. However, there is not a continuous accumulation and storage of the antibody within a-granules as is seen, for example, for fibrinogen.28 This means that internal pools of GPIIb-IIIa do not become saturated with the drug. Furthermore, the fact that abciximab is a Fab fragment and monovalent raises the possibility that we are visualizing natural recycling of GPIIb-IIIa between the surface and internal pools. Such recycling has previously been implied from studies performed with an RGD-based peptide28; thus, smallmolecular-mass inhibitors of GPIIb-IIIa may be expected to behave similarly. The difference in the functional response between platelets from patients receiving abciximab and those from patients with Glanzmann’s thrombasthenia is important to emphasize. In the latter, an inherited GPIIb-IIIa deficiency extends to all membrane systems,32 whereas at the present therapeutic doses of abciximab, a residual pool of functional GPIIb-IIIa complexes can be expressed after a strong hemostatic challenge. Whether this limits the efficacy of abciximab or provides a protective backup to limit the tendency for hemorrhage is an essential question to address both for abciximab and for other anti–GPIIb-IIIa drugs. Interindividual Variability in the Response to Treatment The inhibition provided by abciximab continues at various levels for several days after the infusion has stopped. Possible explanations for its durability include the combined effects of a high affinity for GPIIb-IIIa and a frequent association/ 2838 Arterioscler Thromb Vasc Biol. December 1999 Some of the Factors That May Influence the Efficacy of GpIIb-IIIa Inhibitors in Different Individuals 1. Platelet count High: low level of GPIIb-IIIa occupancy Low (including enlarged spleen): increased bleeding risk 2. Plasma antibodies To mouse immunoglobulin determinants (abciximab) To neonantigens on GPIIb-IIIa (type anti-LIBS) 3. Presence of circulating activated platelets 4. Capacity for the inhibition of the internal pool of GPIIb-IIIa complexes no such thing as a standard patient. Thus, increased biological testing to assess whether platelet function is adequately inhibited might improve the success rate with all anti–GPIIbIIIa drugs. Although platelet aggregometry or flow cytometry are of proven use, simple and rapid point-of-care tests may provide the answer. Among such tests is an automated and quantitative cartridge-based method assessing the competence of the GPIIb-IIIa receptor, as reflected in the ability of platelets to agglutinate fibrinogen-coated beads.35 An alternative system looks at the activated clotting time of whole blood.36 In circulating resting platelets During secretion and surface expression 5. Interindividual variations in the reactivity of the drug with GPIIb-IIIa Polymorphisms of GPIIb and/or GPIIIa Influence of high or low GPIIb-IIIa density Downloaded from http://atvb.ahajournals.org/ by guest on May 2, 2017 6. Different rates of drug metabolism or in the rate of elimination from the blood stream 7. Presence of other thrombotic risk factors (eg, high cholesterol may influence membrane fluidity; diabetes, factor V Leiden, or prothrombin gene G 20210 A variants, polymorphisms of other platelet receptors) 8. Degree of atherosclerosis or variations in the size of the PTCA lesion and the frequency of platelet/vessel wall interactions 9. Variations in the reactivity of platelets with other drugs used during therapy (eg, aspirin, heparin) LIBS indicates ligand-induced binding sites. dissociation cycle, which means that the c7E3 Fab fragments simply move from one platelet to another and are not cleared.5 Smaller inhibitors of GPIIb-IIIa are eliminated from the bloodstream more rapidly than is abciximab. This can be considered to be a safety benefit in the case of untoward bleeding but may lead to a lower efficacy unless the drugs are infused for longer periods. Such factors are critical in that at 80% receptor occupancy, ADP-induced platelet aggregation is severely reduced, whereas at 50% occupancy, aggregation can be more or less normal.4,5 Thus, the “window” for successful therapy is fairly narrow, and for some donors, recovery of platelet function after the drug has been stopped can be quick, even with abciximab.26 The additional inhibition of thromboxane A2 synthesis by aspirin can influence platelet aggregate stability and permit a more rapid dissolution of thrombi in vivo, a potentially important factor in “rescue” therapy.12,33 It is plausible that some individuals possess GPIIb-IIIa complexes, where abciximab (or other anti–GPIIb-IIIa drugs) bind with an altered affinity or where there is an increased propensity for fibrinogen to bind (Table). Polymorphisms in the cytoplasmic domains of GPIIb and GPIIb, implicated in controlling the activation state of the complex,3 are a potential field for study here. Furthermore, a higher than usual density of GPIIb-IIIa complexes could render a standard dose of drug unsuccessful. Variations in patient reactivity to heparin or other medications received by patients with unstable angina (nitrates, calcium antagonists, and/or b-blockers) may also influence the end result. The activating potential of heparin on platelets is well known, and its ability to potentiate the expression of activation-dependent markers has recently been reported.34 Whereas there is a standard dose of drug, there is Other Potential Actions of GPIIb-IIIa Inhibitors That Influence Their Activity Abciximab not only reacts with GPIIb-IIIa but also demonstrates equivalent affinity and functional blockade of the avb3 integrin.37 This latter integrin is widespread, being found on endothelial cells, osteoclasts, and smooth muscle cells, among others. We have recently confirmed the reactivity of this drug with the luminal surface of endothelial cells lining the vascular sinuses in the bone marrow (C. Poujol, C. Durrieu-Jais, B. Larrue, A.T. Nurden, P. Nurden, unpublished data, 1999). Abciximab also interacts with an activationdependent neoantigen present on the leukocyte integrin Mac1.38 These findings are explained through the presence of subunit structural homology and a common epitope recognized by the antibody, which blocked the binding of Mac-1– bearing cells to fibrinogen and intercellular adhesion molecule-1, both ligands of Mac-1.38 The implication is that the drug can interfere with the recruitment of monocytes to sites of vessel injury and inflammation. Although whether these properties provide an additional in vivo benefit of abciximab therapy remains controversial, an inhibitory action of antiplatelet drugs on Mac-1 and avb3 may potentially reduce neointimal hyperplasia after vessel injury and participate in the long-term benefits of their use. In this respect, abciximab contrasts, for example, with eptifibatide, which is specific for GPIIb-IIIa.13 The finding by Reverter et al39 that abciximab has a dampening effect on platelet-mediated thrombin generation may also help explain its antithrombotic efficacy. In that study, the evidence from in vitro experiments suggested that blocking ligand binding to GPIIb-IIIa and avb3 on platelets can inhibit tissue factor–induced thrombin generation by up to 50%. This was caused by inhibition of the expression of procoagulant activity on platelets and the release of procoagulant microparticles (surface exposure of aminophospholipids is followed by a Ca21-dependent binding of factor Va, factor Xa, and prothrombin and a process of microvesiculation). This unexpected dampening of platelet reactivity may be due to the inhibition of “outside-in” signaling promoted by GPIIb-IIIa occupancy and platelet aggregation.3 Prothrombin has also been shown to bind to GPIIb-IIIa directly but by a mechanism different from that of fibrinogen.40 Reduced thrombin generation in the area of vessel injury may also mean less smooth muscle migration and hyperplasia (and restenosis), and less fibrin-bound thrombin within the clot can reduce resistance to thrombolysis via activation of factor XIII. Finally, there is evidence that fibrin can also interact with Nurden et al additional sites on GPIIb-IIIa complexes compared with soluble fibrinogen.41 Because fibrin is a component of most thrombi, the ability of drugs to inhibit platelet attachment to fibrin may be another factor in controlling their antithrombotic potential. Thus, there is a great deal yet to learn about the mode of action of anti–GPIIb-IIIa drugs, and new inhibitors must be tested as comprehensively as possible. Not least, our understanding of the mechanisms underlying those ischemic events that continue despite the use of the anti–GPIIb-IIIa inhibitors must be increased, because these drugs, although representing a major step forward in the control of arterial thrombosis, do not provide a total protection. Acknowledgment 16. 17. 18. 19. This study was financed by funding from the CNRS, Université de Bordeaux II (DRED), the Conseil Régional d’Aquitaine. Downloaded from http://atvb.ahajournals.org/ by guest on May 2, 2017 References 1. Coller BS. Platelet GPIIb/IIIa antagonists: the first anti-integrin receptor therapeutics. J Clin Invest. 1997;100(suppl 11):S57–S60. 2. Goto S, Ikeda Y, Saldivar E, Ruggeri ZM. Distinct mechanisms of platelet aggregation as a consequence of different shearing flow conditions. J Clin Invest. 1998;101:479 – 486. 3. Shattil SJ, Kashiwagi H, Pampori N. Integrin signaling: the platelet paradigm. Blood. 1998;91:2645–2657. 4. Tcheng JE, Ellis SG, George BS, Kereiakes DJ, Kleiman NS, Talley JD, Wang AL, Weisman HF, Califf RM, Topol EJ. Pharmacodynamics of chimeric glycoprotein IIb/IIIa integrin antiplatelet antibody Fab 7E3 in high-risk coronary angioplasty. Circulation. 1994;90: 1757–1764. 5. Mascelli MA, Lance ET, Damaraju L, Wagner CL, Weisman HF, Jordan RE. Pharmacodynamic profile of short-term abciximab treatment demonstrates prolonged platelet inhibition with gradual recovery from GP IIb/IIIa receptor blockade. Circulation. 1998;97: 1680 –1688. 6. The EPIC Investigators. Use of monoclonal antibody directed against the platelet glycoprotein IIb-IIIa receptor in high-risk coronary angioplasty. N Engl J Med. 1994;330:956 –961. 7. The EPILOG Investigators. Platelet glycoprotein IIb/IIIa receptor blockade and low-dose heparin during percutaneous coronary revascularization. N Engl J Med. 1997;336:1689 –1696. 8. Topol E, Ferguson J, Weisman H, Tcheng J, Ellis S, Kleimen N, Ivanhoe R, Wang A, Miller D, Anderson K, Califf R, on behalf of the EPIC Investigators. Long-term protection from myocardial ischemic events in a randomized trial of brief integrin b3 blockade with percutaneous intervention. JAMA. 1997;278:479 – 484. 9. The Capture investigators. Randomised placebo-controlled trial of abciximab before and during coronary intervention in refractory unstable angina: the CAPTURE study. Lancet. 1997;349:1429 –1435. 10. The Epistent Investigators. Randomized placebo-controlled and balloon-angioplasty-controlled trial to assess safety of coronary stenting with use of platelet glycoprotein IIb/IIIa blockade. Lancet. 1998;352:87–92. 11. Schomig A, Neumann F-J, Kastrati A, Schuhlen H, Blasini R, Hadamitzky M, Walter H, Zitzmann-Roth E-M, Richardt G, Alt E, Schmitt C, Ulm K. A randomized comparison of antiplatelet and anticoagulant therapy after the placement of coronary-artery stents. N Engl J Med. 1996;334:1084 –1089. 12. Gold HK, Garabedian HD, Dinsmore RE, Guerrero LJ, Cigarroa JE, Palacios IF, Leinbach RC. Restoration of coronary flow in myocardial infarction by intravenous chimeric 7E3 antibody without exogenous plasminogen activators: observations in animals and humans. Circulation. 1997;95:1755–1759. 13. The IMPACT-II investigators. Randomized placebo-controlled trial of effect of eptifibatide on complications of percutaneous coronary intervention: IMPACT-II. Lancet. 1997;349:1422–1428. 14. The PARAGON investigators. International, randomized, controlled trial of lamifiban (a platelet glycoprotein IIb/IIIa inhibitor), heparin, or both in unstable angina. Circulation. 1998;97:2386 –2395. 15. The RESTORE investigators. Effects of platelet glycoprotein IIb/IIIa blockade with tirofiban on adverse cardiac events in patients with 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. Anti–GPIIb-IIIa Therapy 2839 unstable angina or acute myocardial infarction undergoing coronary angioplasty. Circulation. 1997;96:1445–1453. Kereiakes DJ, Kleiman NS, Ferguson JJ, Masud ARZ, Boderick TM, Abbottsmith CW, Runyan JP, Anderson LC, Anders RJ, Dreiling RJ, Hantsbarger GL, Bryzinski B, Topol EJ. Pharmacodynamic efficacy, clinical safety, and outcomes after prolonged platelet glycoprotein IIb/IIIa receptor blockade with oral xemilofiban. Circulation. 1998; 98:1268 –1278. Mousa SA, Olson RE, Bozarth JM, Lorelli W, Forsythe MS, Racanelli A, Gibbs S, Schlingman K, Bozarth T, Kapil R, Wityak J, Sielecki TM, Wexler RR, Thoolen MJ, Slee A, Reilly TM, Anderson PS, Friedman PA. Oral antiplatelet efficacy and specificity of a novel nonpeptide platelet GP IIb/IIIa receptor antagonist, DMP 802. J Cardiovasc Pharmacol. 1998;32:169 –176. Savi P, Badore A, Lale A, Bordes MF, Bornia J, Labouret C, Bernat A, de Cointet P, Hoffmann P, Maffrand JP, Herbert JM. SR 121787, a new orally active fibrinogen receptor antagonist. Thromb Haemost. 1998;80:469 – 476. Storey RF, Wilcox RG, Heptinstall S. Differential effects of glycoprotein IIb/IIIa antagonists on platelet microaggregate and macroaggregate formation and effect of anticoagulant on antagonist potency: implications for assay methodology and comparison of different antagonists. Circulation. 1998;98:1616 –1621. Berkowitz SD, Harrington RA, Rund MM, Tcheng JE. Acute profound thrombocytopenia after c7E3 Fab (abciximab) therapy. Circulation. 1997;96:809 – 813. Nurden P, Humbert M, Piotrowicz RS, Bihour C, Poujol C, Nurden AT, Kunicki TJ. The distribution of ligand-occupied aIIbb3 in resting and activated human platelets determined by expression of a novel class of ligand-induced binding site (LIBS) recognized by monoclonal antibody AP-6. Blood. 1996;88:887– 899. Yeh CH, Peng HC, Huang TF. Accutin, a new disintegrin, inhibits angiogenesis in vitro and in vivo by acting as integrin avb3 antagonist and inducing apoptosis. Blood. 1998;92:3268 –3276. Buckley CD, Pilling D, Henriquez NV, Parsonage G, Threlfall K, Scheel-Toellner D, Simmons DL, Akbar AN, Lord JM, Salmon M. RGD peptides induce apoptosis by direct caspase-3 activation. Nature. 1999;397:534 –539. Tschoepe D, Schultheiss HP, Kolarov P, Schwippert B, Dannehl K, Volksw D, Nieuwenhuis HK, Kehrel B, Strauer B, Gries FA. Platelet membrane activation markers are predictive for increased risk of acute ischemic events after PTCA. Circulation. 1993;88:37– 42. Scharf RE, Tomer A, Marzec UM, Teirstein PS, Ruggeri ZR, Harker LA. Activation of platelets in blood perfusing angioplasty-damaged coronary arteries: flow cytometric detection. Arterioscler Thromb. 1992;12:1475–1487. Bihour C, Durrieu-Jaı̈s C, Macchi L, Poujol C, Coste P, Besse P, Nurden P, Nurden AT. Expression of markers of platelet activation and the interpatient variation in response to abciximab. Arterioscler Thromb Vasc Biol. 1999;19:212–219. Peter K, Schwarz M, Ylänne J, Kohler B, Moser M, Nordt T, Salbach P, Kübler W, Bode W. Induction of fibrinogen binding and platelet aggregation as a potential intrinsic property of various glycoprotein IIb/IIIa (aIIbb3) inhibitors. Blood. 1998;92:3240 –3249. Wencel-Drake JD, Frelinger AL III, Dieter MG, Lam SC-T. Arg-GlyAsp-dependent occupancy of GP IIb/IIIa by applaggin: evidence for internalization and cycling of a platelet integrin. Blood. 1995;81: 62– 69. Kleimann NS, Raizner AE, Jordan R, Wang AL, Norton D, Mace KF, Joshi A, Coller BS, Weisman HF. Differential inhibition of platelet aggregation induced by adenosine diphosphate or a thrombin receptoractivating peptide in patients treated with bolus chimeric 7E3 Fab: implications for inhibition of the internal pool of GP IIb-IIIa receptors. J Am Coll Cardiol. 1995;26:1665–1671. Nurden P. Bidirectional trafficking of membrane glycoproteins following platelet activation in suspension. Thromb Haemost. 1997;78: 1305–1315. Nurden P, Poujol C, Durrieu-Jais C, Winckler J, Combrié R, Macchi L, Bihour C, Wagner C, Jordan R, Nurden AT. Labeling of the internal pool of GP IIb-IIIa in platelets of patients receiving c7E3 Fab fragments (abciximab, ReoPro): flow and endocytic mechanisms contribute to the transport. Blood. 1999;93:212–219. George JN, Nurden AT, Phillips DR. Molecular defects in interaction of platelets with the vessel wall. N Engl J Med. 1984;311:1094 –1098. Muhlestein JB, Karagounis LA, Treehan S, Anderson JL. ‘Rescue’ utilization of abciximab for the dissolution of coronary thrombus 2840 34. 35. 36. 37. Arterioscler Thromb Vasc Biol. December 1999 developing as a complication of coronary angioplasty. J Am Coll Cardiol. 1997;30:1729 –1734. Knight CJ, Panesar M, Wilson DJ, Patrineli A, Chronos N, Wright C, Clarke D, Patel D, Fox K, Goodall AH. Increased platelet responsiveness following coronary stenting: heparin as a possible aetiological factor in stent thrombosis. Eur Heart J. 1998;19:1239 –1248. Smith JW, Steinhubl SR, Lincoff AM, Coleman JC, Lee TT, Hillman RS, Coller BS. Rapid platelet-function assay: an automated and quantitative cartridge-based method. Circulation. 1999;99:620 – 625. Coiffic A, Cazes E, Janvier G, Lanza F, Nurden A, Nurden P. Inhibition of platelet aggregation by abciximab but not by aspirin can be detected by a new point-of-care test the HemoSTATUS. Thromb Res. 1999;95:83–91. Tam SH, Sassoli PM, Jordan RE, Nakada MT. Abciximab (ReoPro, chimeric 7E3 Fab) demonstrates equivalent affinity and functional blockade of glycoprotein IIb/IIIa and avb3 integrins. Circulation. 1998;98:1085–1091. 38. Simon DI, Xu H, Ortlepp S, Rogers C, Rao NK. 7E3 monoclonal antibody directed against the platelet glycoprotein IIb/IIIa cross reacts with the leukocyte integrin Mac-1 and blocks adhesion to fibrinogen and ICAM-1. Arterioscler Thromb Vasc Biol. 1997;17:528 –535. 39. Reverter JC, Béguin S, Kessels H, Kumar R, Hemker HC, Coller BS. Inhibition of platelet-mediated, tissue factor-induced thrombin generation by the mouse/human chimeric 7E3 antibody: potential implications for the effect of c7E3 Fab treatment on acute thrombosis and ‘clinical restenosis.’ J Clin Invest. 1996;98:863– 874. 40. Byzova TV, Plow EF. Networking in the hemostatic system: integrin aIIbb3 binds prothrombin and influences its activation. J Biol Chem. 1997;272:183–188. 41. Hantgen RR, Mousa SA. Inhibition of platelet-mediated clot retraction by integrin antagonists. Thromb Res. 1998;89:271–279. KEY WORDS: glycoproteins drugs n abciximab n platelet aggregation n antithrombotic Downloaded from http://atvb.ahajournals.org/ by guest on May 2, 2017 Downloaded from http://atvb.ahajournals.org/ by guest on May 2, 2017 Platelet Glycoprotein IIb/IIIa Inhibitors: Basic and Clinical Aspects Alan T. Nurden, Christel Poujol, Catherine Durrieu-Jais and Paquita Nurden Arterioscler Thromb Vasc Biol. 1999;19:2835-2840 doi: 10.1161/01.ATV.19.12.2835 Arteriosclerosis, Thrombosis, and Vascular Biology is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1999 American Heart Association, Inc. All rights reserved. Print ISSN: 1079-5642. Online ISSN: 1524-4636 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://atvb.ahajournals.org/content/19/12/2835 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Arteriosclerosis, Thrombosis, and Vascular Biology can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Arteriosclerosis, Thrombosis, and Vascular Biology is online at: http://atvb.ahajournals.org//subscriptions/