Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Audiology and hearing health professionals in developed and developing countries wikipedia , lookup
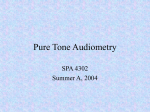
Auditory system wikipedia , lookup
Sound localization wikipedia , lookup
Noise-induced hearing loss wikipedia , lookup
Evolution of mammalian auditory ossicles wikipedia , lookup
Sensorineural hearing loss wikipedia , lookup
White noise wikipedia , lookup
COMD 3700 Basic Audiology Week 8 Masking II Highlighted information refers to a change between the audio recording (using 10th edition) and the 11th edition of the textbook 1. COMD 3700 for distance education. This is lesson 8, Masking II. This is the second part of a discussion on masking. We will be covering page 133-145 in your textbook. Up to this point we have discussed cross hearing, test ear, non-test ear, interaural attenuation and the need to mask whenever we have cross hearing. Basically, the idea is to test the air conduction and bone conduction on the test ear. Then look at that audiogram when you're finished and ask yourself the question. Do we have to retest the patient and find a threshold in either ear via air conduction while we are masking the non-test ear? Then do the same with bone conduction. We look at the audiogram and say; do we need to retest bone conduction in either ear or both ears while we are masking the non-test ear? Then when we're finished, if we did proceed with masking procedures, when we're finished with the masked audiogram, we should have a true picture of the patient's threshold, the degree of the hearing loss, and the type of hearing loss (normal, mixed, sensorineural, or conductive hearing loss). At this point you should have a good understanding of these concepts. However, we don't know how to mask yet. We haven’t discussed the actual procedures. All we've talked about is the need to mask. So in this section, we'll talk about the stimulus we use for masking. Audiometers use several kinds of masking noise. We will discuss several of the more common masking noises. We also cover how we actually perform the masking procedures when it is needed and then review some audiograms before and after masking. 2. The first step in clinical masking is to explain to the patient exactly what is going to happen and how they are to respond. It can be confusing to the patient if they are just told that there will be some noise in their ears. If not properly counseled, the patient will respond to the masking noise rather than the stimulus. They should be told that they will hear some noise similar to static in one ear, but that they should respond only when they hear the tone in addition to the noise. It can also be explained that this is similar to the optometrist 1 covering one eye while testing the other. You need to let the patient know to respond whenever they hear the tone, no matter which ear they hears it in. They may hear it in the non-test ear sometimes (thus the need for masking). If you tell the patient to respond only when the tone is heard in the TE, your results may be invalid. So for example, you could say to the patient: You will hear some tones again. Every time you hear a tone, push the button/raise your hand. You will hear some noise in the LEFT/RIGHT ear (describe it as static or running water and tell the patient which ear it will be heard in.) Ignore the noise, and listen for the tone. It doesn’t matter which ear you hear the tone in, go ahead and respond. Do you have any questions? 3. So now that the patient is properly prepared, what kind of noise should be used to keep the NTE busy so that it will not respond to the stimulus? The answer to this depends on the signal being masked. When masking pure tones, one type of masking noise is white noise. It is also known more accurately as broadband or wideband noise. In looking at this figure representing white noise, you are looking at a sound spectrum with the frequency along the abscissa and the intensity in dB SPL along the ordinate. What you are actually seeing here are all of the frequencies from 125-8000 Hz to cover the testing spectrum. Each individual frequency is represented equally. This term white noise is borrowed from the light spectrum people, where white lights are a representation of all of the light frequencies equally. White noise is a broad band of noise that contains equal amounts of energy at all frequencies. White noise is reasonably effective for both pure tone and speech testing, although listening to the noise is fatiguing for any length of time. White noise is not as efficient in the lower frequencies as it is in the higher frequencies because of the upward spread of masking. So, while we could use white noise as a masking stimulus, there are some drawbacks. Wide band noise is a poor choice for masking pure tones because it is both inefficient and unnecessarily loud. Since all of the frequencies are represented, but only 1 single frequency is being tested at a time (ex 1000 Hz) why present extra energy to the patient with white noise when you only need to mask out 1 single frequency? Why not filter that down so you have bands of noise that surround a particular frequency and then the patient has been relieved from all of the energy involved from the other frequencies. 2 4. Well, this can be done and it is known as Narrow Band Noise or NBN. NBN consists of a narrow range of frequencies of equal intensity. What has taken place here is that we have taken the White Noise spectrum initially and have identified the central frequencies that might be used in testing (250-8K). You can see those along the bottom. Then notice the dark line running up through in the center of the cones that represent the central frequency. So the dark line on the left is 500 Hz, and the dark line in the next cone is 2K Hz and the next cone is 8000 Hz. We can do this for each frequency. Then you notice the skirt coming off of the top central frequency. So there are some components of noise coming off of the individual noise frequencies. These are called noise bands & they are identified by their central frequency. So the cone on the left is a NBN with a central frequency of 500 Hz and the cone on the right is a NBN with a central frequency of 8000 Hz. This is the best noise to use when masking in pure tone audiometry. For instance, if you were testing 500 Hz then you would only need to use the cone to the left (there would not be any other cones) rather than the entire spectrum like white noise. If we are then testing with a pure tone stimulus of 2000 Hz & we want to mask the NTE then we would need to change the corresponding NBN with a central frequency of 2000 Hz. So each time we change the frequency we need to change the NBN so it is the same. This is done automatically on a diagnostic audiometer. The range of frequencies making the masking noise changes is in direct relationship to the frequency dial on the audiometer. For instance, when testing 250 Hz, the narrow band masking automatically centers around 250 Hz. Changing to 500 Hz centers the NBN at 500 Hz. Narrow Band Noise is more effective and easily tolerated than white noise for pure tones. 5. The appropriate type of masking depends of the signal being masked. If the signal has a wide spectrum (Speech or Clicks) then the masking noise must also have a wide spectrum. We will not be discussing masking for speech testing in this course. But just so you are aware, other masking noises for speech tests include: Pink Noise, Speech Shaped Noise and Multitalker babble 6. Before we begin to discuss the methods to masking appropriately there are some terms you should be familiar with. Effective Masking (EM) eliminates crossover from occurring. EM determines how much 3 noise is appropriate to ‘cover up’ or ‘keep busy’ the better ear or NTE from taking part in the test. We have discussed the formulas to determine EM levels. Undermasking occurs when the masking noise presented to the better or NTE is not loud enough to eliminate crossover or Interaural Attenuation. The patient hears the tone in the same ear as the masking noise, the NTE. An increase in the masking noise causes the false threshold to shift from the NTE, and drop to the true threshold of the TE. Undermasking occurs more commonly in air conduction testing. Overmasking is the condition when the noise presented to the NTE is intense enough to cross over to the TE and mask it. You will know that this is occurring when each 10 dB increase in masking shifts the hearing threshold 10 dB or more above the plateau. Overmasking occurs more commonly in bone conduction testing. When using a controlled masking stimulus, ideally, our noise is effective throughout the test. Undermasking allows a false, better hearing threshold, while overmasking drives the true threshold lower. 7. So, we have established that masking must be completed whenever the possibility of cross hearing exists. Interestingly enough, a survey of clinical audiologists showed more disagreement on masking methods, and greater insecurity, than on any other clinical procedure. (So, if you are feeling overwhelmed, you are not alone). Due to this, I am not going to go into detail about all of the various approaches to masking. You can review the shotgun approach, the minimum noise method and the maximum noise method in your textbook. There is also a method known as the step masking method. However, we will discuss the Plateau Method because it is often employed in clinical masking. 8. In the plateau method, basically the non-test ear is masked by progressively greater amounts of sound until the threshold of the test ear does not continue to increase. This indicates the "true" threshold of the test ear and masking may be discontinued. Hood described this method in 1960. It is sometimes called the threshold shift method. Before we start it is important to know what plateau is referring to in this method. The plateau is a range of masking levels in which there is no increase in threshold of the TE. In this method, 5 or 10 dB steps at a time are used. When an adequate level of masking has been reached, there are generally several successive levels of masking that yield the same PT threshold in the TE. In other words, it produces no 4 threshold shift in the TE. Most audiologists use 3 consecutive masked levels (5 or 10 dB steps) with the same response to be a threshold. 9. This might be easier to understand by looking at this graph. A similar graph is found on Figure 6.4 on page 140 in your book. This shows the results of a hypothetical test. The ordinate is the threshold of the tone in the TE when various levels of masking noise are being presented to the NTE. The abscissa shows the level of the masking noise in the NTE. In this example, let’s say the apparent threshold of the test ear unmasked was 35 dB. However, after masking is presented at the lowest level used of 20dB it caused the threshold to shift to 45dB. Notice the rest of the graph breaks down into 3 distinct ranges: undermasking, plateau and overmasking. We defined these earlier. So, in undermasking, when a tone is really being heard by the NTE via cross hearing, then raising the level of the masking noise will cause the masked threshold to increase. This occurs because the noise and tone are both in the same NTE. In the graph it shows that raising the masking noise from 20-40 dB HL caused the apparent TE threshold to rise from 45 to 65 dB HL. The one-for-one elevation occurs because masking increases linearly with the masking level. This indicates that the tone is still being heard by the NTE. The plateau occurs when the NTE is effectively masked by the noise so that the tone is heard by the TE only. So, only the TE hears the tone stimulus and the noise stimulus is heard only by the NTE. When the tone is really being heard in the TE, then raising the masking noise level will not cause the threshold to change. This is what is happening in the middle of the graph where the threshold stays at 65 dB, despite the masking noise level being raised from 40 to 60 dB HL. This plateau reveals the true masked thresholds for the TE. The width of the plateau is called the range of effective masking. The plateau occurs because the noise is effectively masking the non-test ear so that the TE can hear the tone. Raising the noise in the NTE continues to keep it effectively masked. This means that the TE can respond to the tone at its own threshold. Once the noise is effectively masking the non-test ear, you can add more noise without affecting the threshold because the amount of noise covering the NTE has nothing to do with the TE. However, this has limits. If the level of the noise presented to the NTE becomes too loud, then it can cross over and mask the TE. Once this occurs then the threshold in the TE will start 5 to rise again as the masking level is increased. This is the overmasking range. 10. The procedure to properly use masking during AC testing with the plateau method is as follows: Obtain and record the AC threshold of the TE unmasked. Then compare the AC threshold of the TE with AC and BC thresholds of NTE to determine if masking is needed. Remember the rules for masking state that masking is required in the better ear when the difference between AC thresholds of the TE and the BC thresholds of the NTE is 40 dB or more if using supra-aural headphones and 70 dB or more if using insert earphones. Next you need to select the initial amount of masking (IM) using Narrow band noise on the audiometer for the NTE. To determine the initial amount of masking, most audiologists use this formula. The IM = AC NTE+ 10 dB EML. Remember when I said that there is a lot of variation when it comes to masking methods? Well, some audiologists use 5dB and others use 15 dB effective masking level (EML). But take for example if the threshold for AC NTE =10 dB, then you would present 20 dB of NBN to the NTE. This is due to 10 dB from the threshold +10 dB for the EML. Then you must reestablish threshold in the TE with this initial amount of masking in the NTE. 11. Now, each time the patient responds to the PT signal presented to the TE, increase masking noise in the NTE by 10 dB. Each time the patient does not respond to the PT signal in the TE, increase the tone in the TE in 5 dB steps until the patient responds again. This procedure is continued until the masking noise can be increased over a 30 dB interval (3 consecutive 10 dB steps) without producing a shift in the threshold level of the TE. Then you know that you have reached the “Plateau” and the AC pure tone intensity level you reached is the actual threshold of the TE. 12. When masking for pure tone bone conduction thresholds the methods are very similar. However, there are a few considerations that must be taken into account. First, the headphone placement is different. The earphone produces the masking noise in the NTE. So it needs to be placed over the ear of the patient. However, the test ear, with the bone vibrator on the mastoid process must not be occluded in any way with the earphone, so the earphone should be placed on the head of the patient, but not over the ear. You can see how that is 6 done in this picture. It is important that you tell the patient that this strange arrangement is being done on purpose. (I can’t tell you how many times a patient has told me that the earphone is not on their ear or tried to move it back onto their ear). The patient should also be told to sit as still as possible so that the equipment does not move and that if it does, they should let you know. This set up is then reversed when it is time to test for the other ear’s masked BC thresholds. Keep in mind that because the earphone is placed over the NTE, then the occlusion effect, which we talked about earlier, may be created in that ear. The occlusion effect may cause BC thresholds to shift once headphones are placed on the head. 13. The plateau masking procedures also apply to BC testing. We will discuss how to use this method when masking for BC. Remember that stimulus delivered via BC can crossover with 0dB difference between ears. The first step is to obtain and record the BC threshold of the TE unmasked and unoccluded. Once this is complete, you compare the AC thresholds with the BC thresholds. We discussed that this is known as the air bone gap. This will determine if masking is needed. If there is a difference of 10 dB or more between the AC and BC results, then masking is required. So to begin, you select the initial amount of masking (IM) for the NTE using NBN. A good formula for this is IM = AC NTE+ 10 dB EML (effective masking level) + the amount needed to overcome the OE (occlusion effect). Remember that the OC is the enhancement of BC produced by closing off the external ear canal. So in low frequencies, additional masking should be added to the starting levels at low frequencies. 15 dB should be added to 250 Hz and 500 Hz and 10 dB should be added at 1000 Hz. Then you must reestablish threshold in the TE with this initial amount of masking in the NTE. Each time the patient responds to the PT signal presented to the TE, increase masking noise in the NTE by 10 dB. Each time the patient does not respond to the PT signal in the TE, increase the tone in the TE in 5 dB steps until the patient responds again. Continue this procedure until the masking noise can be increased over a 30 dB interval (3 consecutive 10 dB steps) without producing a shift in the threshold level of the TE. This is the “Plateau” and the BC pure tone intensity level you reached is the actual threshold of the TE. 7 14. As the masked thresholds are obtained, they need to be plotted on the audiogram. As you find masked thresholds, then they will replace unmasked thresholds on the audiogram. If all of the results are left on the audiogram it will become very cluttered and misleading. 15. Here are the correct symbols for masked and unmasked thresholds. 16. So now that we know how to mask, let’s look at some audiogram interpretation before and after properly masking. Hopefully this will help solidify what we have been learning. The first patient is Jenny Urry. This is her unmasked audiogram tested using supra-aural headphones. As you can see, Jenny has normal air and bone conduction thresholds in the left ear. However, when the right ear was tested, it was found that she had moderate air conduction thresholds and normal bone conduction thresholds, so it appears that she has a conductive hearing loss in the right ear. But before we can conclude this, we must decide if masking is needed. Are we suspicious that the AC stimulus crossed over and was heard by the NTE? Let’s look at the rules. If the AC threshold is 40 dB or greater than the BC of the NTE, then we need to mask. When we look at his, we are close. But we don’t need to mask for AC. The AC stimulus did not cross over from the right ear to be heard by the left ear. However, the other rule for BC is that masking is needed if there is a 10 dB or greater ABG in the TE (right ear). In this case the answer is yes. So we need to mask the NTE (Left) and retest the BC in the TE (Right) and we’ll see what happens. 17. In this slide we have now masked and retested the BC in the right ear. As you can see it is in fact a conductive hearing loss. The BC thresholds remained at 0-5 dB. Jenny has a normal inner ear in both the left & right ear. She has something happening in her outer or middle ear that is causing the conductive hearing loss in her right ear. If you go back to Jenny’s unmasked audiogram you would not be able to say for sure whether she had a conductive, mixed or SNHL in the right ear until you have masking appropriately. But now we know for sure that it is a conductive hearing loss. 18. The next patient, Rob Christianson, has a bilateral moderate SNHL unmasked. So, now think about the conditions to determine 8 whether or not we need masking. Is there a 40 dB difference between the AC in the left ear & BC in the right ear? No. Is there a 40 dB difference between the AC in the right ear & BC in the left ear? No, so AC does not need to be masked. Is there a 10 dB or greater ABG in the right ear? No. Is there a 10 dB or greater ABG in the left ear? No, so we do not need to retest BC with masking. This audiogram is complete. It truly is a symmetrical bilateral SNHL. 19. On our final patient, Rick Lambert, his unmasked audiogram appears that he has a normal to mild SNHL in the right ear & a mild to moderate mixed HL in the left ear. This is your classic mixed HL. He has some SNHL & some conductive HL. Where is the conductive portion of the HL? It is the area between the BC and AC symbols. The area above the BC symbols is the SN portion of the HL. So, do we need to mask this patient? Look at the right ear. Is there a 40 dB difference between AC in the right ear and BC in the left ear? No, so AC is fine. Is there a 10 dB or greater ABG between the AC & BC results? No, so the right ear does not need to be masked. So, now let’s make the left ear the TE. Are the AC thresholds in the left ear 40 dB or greater than BC in the right ear. At 500 Hz the AC thresholds of the left ear is 55 and the BC threshold of the right ear is 20. The difference is 35 dB, so we don’t need to mask. However, when you look at all of the frequencies, you should determine that we do need to mask for AC in the left ear. There is a 45 dB difference between the left ear AC thresholds and the right ear BC thresholds at 2000 Hz. At 4000 Hz there is a 40 dB difference. So, we will need to mask for AC. What about BC? Is there a 10 dB or greater ABG? Yes, so we will need to retest BC in the left ear while masking the right ear. 20. So, this is what the audiogram looks like after AC and BC masking have been completed. Because masking was needed for 2000 and 4000 Hz and the other frequencies were right on the edge, we decided to mask them all. When masking was placed in the right ear, the AC thresholds in the left ear dropped slightly. When BC was retested using masking, the BC symbols fall down very close to the AC. Note the symbols at 250 & 4000 Hz have the arrow coming out of the symbol. This means that we reached the limits of the audiometer and he did not respond. So his threshold must have been worse than that. So after masking, Rick Lambert, has a normal to mild SNHL in the right ear and a moderate to severe SNHL in the left ear. Go back & 9 compare the before and after masking audiograms on these patients so that you understand what a difference masking can make. Without masking, Rick would have been diagnosed with a mild to moderate mixed hearing loss instead of the actual moderate to severe SHNL that he has. 21. So, in conclusion, as a rule to remember- when it doubt, mask. It is better to mask and find out that it was not required. Test results obtained without masking when there is a need for masking, result in improper test results. So, why don’t we just use masking on every patient? Masking is time consuming and adds several steps to the test procedure, so it is important to understand the rules of when to mask. You should have those two rules or formula memorized. I know that masking can be a confusing concept. If you continue to study audiology, you will learn more concepts and tips about masking. But hopefully you all understand it well enough now to see how important it is in determining the true audiometric thresholds of a patient. 10