Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
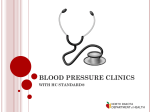
HEALTH EDUCATION RESEARCH Theory & Practice Vol.15 no.3 2000 Pages 317–326 The ‘Heart Attack Survival Kit’ project: an intervention designed to increase seniors’ intentions to respond appropriately to symptoms of acute myocardial infarction Hendrika Meischke, Mickey Eisenberg1, Sharon Schaeffer2 and Daniel K. Henwood2 Abstract The purpose of this study was to test the effectiveness of a ‘Heart Attack Survival Kit’, disseminated via two different delivery methods, designed to increase seniors’ intentions to call 911 and take an aspirin in response to a cardiac emergency. Twelve-hundred seniors were randomly assigned to (1) receiving a Kit via a home visit by an Emergency Medical Technician (EMT), (2) receiving a Kit via direct mail or (3) a control group. All participants were telephoned and asked how they would respond to a cardiac emergency. Results showed that respondents in the intervention group (EMT and direct mail group combined) reported a greater frequency of the recommended coping response to AMI (39%) than respondents in the control group (10%) (P ⬍ 0.000). Within intervention groups, 47% in the EMT group and 30% in the direct mail group (P ⬍ 0.000) reported intentions to take the appropriate response to AMI. The results suggest that a Heart Attack Survival Kit, especially when delivered door-to-door by EMTs, can be an effective way of educating seniors about cardiac emergencies. Introduction This year 1 500 000 Americans will have a new or recurrent acute myocardial infarction (AMI) and Department of Health Services and 1Department of Medicine, University of Washington, Seattle, WA 981956123, and 2King County Emergency Medical Services Division, Seattle, WA 98104-4039, USA © Oxford University Press 2000 about one-third of them will die (American Heart Association, 1996). The two most critical actions a patient can take when faced with AMI symptoms are: (1) seeking prompt medical care, preferably by calling 911, so therapy can begin soon after onset of AMI and (2) taking an aspirin at onset of a heart attack. These recommendations have been endorsed by the National Heart, Lung and Blood Institute as well as the American Heart Association (National Institute of Health, 1997; Hennekens et al., 1998). However, many AMI patients do not follow these life-saving actions. This paper reports on the results of an intervention designed to increase intentions among seniors 65 years and older to respond promptly and appropriately to symptoms of AMI. Seeking prompt medical care for symptoms of AMI Thrombolytic therapy can alter the course of AMI, reducing morbidity and mortality (Yusuf et al., 1985; Marder and Sherry, 1988). However, its efficacy decreases with increasing time between symptom onset and treatment (Second International Study of Infarct Survival Collaborative Group, 1988). Patient delay accounts for most of the delay in receiving thrombolytic therapy (Dracup et al., 1995). Quick use of emergency medical services (EMS) for AMI symptoms can dramatically shorten overall prehospital delay time (Grim et al., 1989; Weaver et al., 1990). Unfortunately, over half of all patients admitted to the hospital for possible AMI do not call 911 (Ho, 1991). Small- and large-scale interventions have been conducted to reduce prehospital delay time for symptoms of AMI and increase utilization of the 317 H. Meischke et al. emergency medical services for AMI patients (Ho et al., 1989; Herlitz et al., 1992; Blohm et al., 1994, 1996; Eppler et al., 1994; Gaspoz et al., 1996; Meischke et al., 1997). These interventions have been only moderately successful. It appears from these and other studies that it is inherently difficult to persuade people to take a seemingly ‘drastic’ action (i.e. call 911) for a seemingly nonemergent situation (i.e. chest pain). Focus group research with AMI patients showed that people prefer to wait and see before taking actions which could be embarrassing to them (Finnegan et al., submitted). It seems plausible that one way to ‘legitimize’ calling 911 for an often ambiguous situation is to have the people who are most immediately involved in people’s handling of emergencies, i.e. the local firefighters, persuade people that calling 911 is the best action to take in response to AMI symptoms. Aspirin use and AMI Experimental and clinical investigations have shown that early administration of aspirin during an AMI significantly reduces AMI mortality (Fuster et al., 1993; Hennekens et al., 1994; Collins et al., 1997). There are important reasons why patients should be encouraged to take an aspirin when they first experience symptoms of AMI. First, the sooner the aspirin is given, the more quickly the drug will have treatment benefits. Second, aspirin as a treatment for evolving AMI is still under-administered by health care providers even though ineligibility criteria are few (Eisenberg and Topol, 1996; Hennekens et al., 1998). For these reasons, patients’ self-administration of aspirin for symptoms of AMI may greatly benefit the patient when the aspirin ingestion is part of a ‘prompt’ coping response, including calling 911. In this project the objective was to test an intervention designed to increase seniors’ intentions to (1) call 911 and (2) take an aspirin in response to AMI symptoms. Theoretical foundation of intervention The conceptual foundation for the intervention was based on Leventhal’s self-regulatory model of 318 health and illness (Leventhal et al., 1984). According to this model a person assesses a symptom episode based on general knowledge as well as personal experience with illness episodes. The actual heart emergency is the initiating factor in the cascade of events in the model. Regardless of the timing or nature of this recognition, the person will do two things: react emotionally to the recognition and develop an internal understanding or mental representation of what the symptoms that s/he is experiencing mean to her. Results from focus group discussions with AMI patients revealed that fear and denial were frequently experienced during the cardiac emergency (Finnegan et al., submitted). This mental representation will then influence any future actions, such as taking aspirin, calling 911, asking someone for advice, denying the importance of the problem and/or avoiding thinking about one’s personal risk for a heart attack. Research shows that patients who believed that their symptoms were cardiac in origin sought medical care faster and used the EMS system more often than those who did not believe their symptoms were cardiac in origin (Johnson and King, 1995; Meischke et al., 1995). Shortening the cognitive and behavioral processes suggested by the self-regulatory model, and changing the kind of coping strategies heart attack patients apply during a heart emergency, could mean the difference between life and death. Educating older adults about the importance of being ‘prepared’ for this emergency (and giving them the tools to be prepared) will likely aid people in accurately assessing the representation of the health threat and reducing lengthy and unproductive coping strategies and appraisals. This ‘preparedness’ will be accomplished by the home delivery of a ‘Heart Attack Survival Kit’, which includes: (1) Eye-catching design and adhesive strips for ‘permanent’ placement in the home. (2) List of the warning signs of AMI. (3) Strong recommendation to call 911. (4) Strong recommendation to take an aspirin for chest pain. (5) One 325 mg uncoated adult aspirin. The ‘Heart Attack Survival Kit’ project (6) Basic steps of CPR. (7) Space for medications/allergies and important phone numbers. A home visit by an emergency medical technician was believed to provide the best opportunity for educating seniors about the importance of calling 911 and taking an aspirin in response to AMI symptoms. Development of the Heart Attack Survival Kit The Heart Attack Survival Kit was developed over a 1-year period with the help of a commercial marketing company. Several iterations of the Kit were tested with groups of seniors age 65 and older until the Kit was designed in a way that appeared useful and attractive to the target audience. Furthermore, the results of the focus groups suggested that seniors preferred direct mail, doctor’s offices or pharmacies for dissemination of the Kit. Although it was clear from the discussions with the focus group participants that firefighters were perceived as highly credible sources of health information, many seniors had reservations about a personal visit of any kind. Most believed they would not be home and if they were home they probably would not answer the door if they believed a stranger was calling. This prompted us to test two delivery methods: a home visit by an EMT and direct mail. Hypotheses We hypothesized that, compared to seniors who did not receive the Kit, those who did receive the Kit would more frequently report intentions to engage in the two recommended coping strategies in response to AMI symptoms: calling 911 and ingesting an aspirin. Second, we hypothesized that seniors randomized to the EMT-delivery group would be more likely to report intentions to engage in the recommended coping strategies than seniors randomized to the direct mail group. We also hypothesized that seniors who reported that they had actually received the Kit from a local firefighter would be (1) more likely to report intentions to engage in the recommended coping strategies and (2) more likely to have placed the kit in a visible place in their home than seniors who reported they had received the Kit via direct mail. Additionally, we investigated the relationship between intervention status (e.g. EMT-delivery, direct mail or control group) and the recommended coping strategies while accounting for demographic variables such as age, gender and education. Procedure In the spring of 1998, 1200 addresses and names of individuals age 65 years and older in the Kent, Washington area were obtained from a commercial mailing list. These 1200 individuals were randomly assigned to one of three groups: EMT door-todoor-delivery group, direct mail group and control group (no Kit). In the EMT door-to-door-delivery group, seniors received a passive consent letter in the mail informing them that a Kent firefighter would be stopping by in the near future to give out a valuable Heart Attack Survival Kit. All firefighters are trained as EMTs in King County, Washington. Twelve percent of participants in the EMT-delivery group mailed in a postcard indicating they did NOT want a visit by a firefighter, leaving 352 people available for a door-to-door contact. Firefighters filled out tracking forms indicating the type of contact made, the duration of the visit and the outcome of the visit. Firefighters had a script to guide their interactions but they were allowed to answer questions regarding the Kit’s contents. They were instructed to hang the Kit (which was placed in a plastic doorhanger bag) on the doorknob if nobody opened the door at the specific household. In the direct mail intervention seniors received the Heart Attack Survival Kit and a letter explaining the purpose of the Kit through the mail. The control group did not receive any intervention. This study was reviewed and approved by the Internal Review Board (IRB) of the University of Washington. Three firefighters from the Kent fire department completed 350 household contacts during day time hours (9 a.m. to 5 p.m.) over a 2-week period. From the tracking forms it appeared that (210) 60% of the 350 households that were approached by a firefighter had resulted in a contact with an 319 H. Meischke et al. Fig. 1. Flow chart of study participants. *All 400 participants in each group were contacted by telephone regardless of intervention delivery status. eligible study participant (i.e. person on mailing list or spouse). In 38% of cases firefighters put the Kit on the doorknob and in 2% of cases the address on the list was wrong or no eligible study participant was living at that address. All 1200 individuals were contacted by phone between 1 and 6 weeks after having the intervention, by one of five interviewers who were blinded to study interventions and hypotheses. (See Figure 1 for flow chart of study participants.) Survey instrument The telephone survey included questions regarding intentions to cope in response to symptoms of AMI, exposure and evaluation of the Heart Attack Survival Kit. To assess intentions to respond in a prompt and appropriate manner, interviewees were asked two 320 open-ended questions: ‘If you experienced symptoms of a heart attack, what would be the first thing you would do?’ and ‘What would be the second thing you would do?’. Answers were coded as (1) calling 911, (2) taking aspirin and (3) other. To make sure that we would obtain information from all participants on intentions to use the recommended coping strategies, interviewees were also asked to rate (‘1’ very likely, ‘2’ somewhat likely, ‘3’ somewhat unlikely’ and ‘4’ not at all likely) the following statements: ‘How likely is it that you would call 911 if you were experiencing symptoms of a heart attack?’ and ‘How likely is it that you would take an aspirin if you were experiencing symptoms of a heart attack?’. To assess exposure to the Heart Attack Survival Kit, respondents were asked: ‘Do you remember receiving a red flyer in the shape of a doorhanger The ‘Heart Attack Survival Kit’ project in the past month telling you how to respond to symptoms of a heart attack?’. Regardless of the response respondents were asked: ‘This flyer/doorhanger had the name Heart Attack Survival Kit written on the front. Do you remember receiving such a Kit?’. If respondents answered affirmatively they were asked: ‘How did you receive this Kit?’. To assess attention to and evaluation of the Heart Attack Survival Kit, we asked respondents who reported that they had received the Kit the following questions: (1) ‘Do you have the Heart Attack Survival Kit in your home?’. If no, ‘What did you do with it?’. If yes, ‘If you needed it right now would you be able to find the Heart Attack Survival Kit?’. Subsequently respondents were asked where they had placed the Kit and what they remembered about the content of the Kit. They were also asked if they liked the Kit and if they thought the Kit was useful or upsetting. The last part of the survey included questions about demographic characteristics such as age, gender, income and educational level. Methods Of the 1200 follow-up phone calls, 705 were completed interviews, 180 refusals, 125 no contact during study period, 89 ineligible (i.e. deceased, moved away, nobody over 65 years of age), 63 non-working number, 24 disabled (deaf, very ill, language difficulty) and 14 other (on vacation, etc.). The respondent refusal rate was 20% based on a formula by Lavraskas (Lavraskas, 1987). Results A total of 705 participants were interviewed, 268 from the EMT-delivery group, 214 from the direct mail group and 223 from the control group. Eighty percent (217) of people in the EMT-delivery group remembered the red doorhanger/flyer and 55% (118) of people in the direct mail intervention. Of the 217 seniors in the EMT-delivery group who reported receiving the Kit, 36% (79) had received the Heart Attack Survival Kit as a doorhanger on their doorknob. The demographic characteristics of the total sample was as follows: (51%) male, mean age of 73, with a standard deviation of 6.4. Education: 8% reported less than high school degree, 33% a high school degree, 30% some college and 29% a college degree or higher. Income: 19% reported income levels below $20 000, 34% reported income of $20 000–40 000, 15% reported income levels of $40 000–60 000, 7% reported income levels greater than $60 000 and 25% either did not know or refused to answer this question. In 84% of the interviews the person on the mailing list was reached. In 16% of the completed interviews the spouse of the person on the list was interviewed. There were no statistically significant differences in any of the demographic characteristics between the three study groups (i.e. EMT-delivery, direct mail or control). Intentions to respond to symptoms of AMI Since the main recommendation of the Heart Attack Survival Kit was to motivate seniors to (1) call 911 and (2) take an aspirin for heart attack symptoms, we investigated differences between groups for intentions to call 911 and taking aspirin (combined) as a coping strategy for AMI. To answer our first hypothesis we combined participants randomized to the EMT-delivery group with those randomized to the direct mail group (i.e. intervention group) and compared their responses to participants in the control group. Table I shows that respondents in the intervention group reported a greater frequency of the recommended coping response to AMI than respondents in the control group. It appears that this result was mostly caused by differences in intentions to ingest aspirin, as part of the coping response rather than calling 911. The two groups were equal in their intentions to call 911 as a first as well as second action in response to AMI. However, intentions to take an aspirin as a first or second action in response to AMI symptoms was significantly greater in the intervention than the control group. Responses to the forced-choice continuous likelihood questions resulted in similar outcomes. 321 H. Meischke et al. Table I. Main results for intervention status and intended coping response for symptoms of AMI Calling 911 and taking aspirin as response to AMI symptomsa Call 911 as first response to AMI symptomsa Call 911 as second action in response to AMI symptomsa Take aspirin as first response to AMI symptomsa Take aspirin as second action in response to AMI symptomsa Likelihood of calling 911b Likelihood of taking aspirinb aχ2 Intervention (N ⫽ 482) (%) Control (N ⫽ 223) (%) P value 39 75 18 13 28 1.2 1.8 10 72 15 3 9 1.2 2.6 0.00 0.28 0.26 0.00 0.00 0.87 0.00 analyses. bt-tests. Table II. Comparison of intervention groups: EMT-delivery versus direct mail Calling 911 and taking aspirin as response to AMI symptomsa Calling 911 and taking aspirin as response to AMI symptomsa Do you like the Kit? Do you have the Kit in your home? If you needed the Kit right now could you find it? How useful is the Kit? (‘very useful’) aThis bThis Seniors randomized to EMTdelivery groupa (N ⫽ 266) (%) Seniors randomized to direct mail group (N ⫽ 212) (%) P value 46.6 29.7 0.000 Seniors who remember receiving the Kit from a firefighter (N ⫽ 137) (%)b Seniors who remember receiving the Kit via mail (N ⫽ 116) (%) P value 56.9 98.5 97.1 93.8 75.4 42.2 89.6 91.5 90.4 73.7 0.014 0.002 0.088 0.561 0.437 group includes seniors who received the Kit via doorknob. group does not include seniors who received the Kit via doorknob. Table II shows the results of the second and third hypotheses. Within intervention groups, participants in the EMT-delivery group reported significantly greater intentions to use the recommended coping response to AMI symptoms than participants in the direct mail group. When the sample was limited to the participants who reported they had actually received the Kit, the results were similar; those participants who reported receiving the Kit from a firefighter were significantly more likely to report intentions to use the recommended coping strategy than those participants who reported receiving the Kit via direct mail. Addition- 322 ally, seniors who had received the Kit from a firefighter were significantly more likely to say they liked the Kit and slightly more likely to report they had the Kit in their home than seniors who reported they had received the Kit via direct mail. There were no differences in participants’ ability to locate the Kit during the interview or in their perceived usefulness of the Kit. Since our objective was to compare direct mail and EMT home delivery, and since the sample of people who reported receiving the Kit via doorknob was much smaller (N ⫽ 79) than the other two groups, we excluded this group from this analysis. The ‘Heart Attack Survival Kit’ project To assess the impact of demographic variables on intentions to take the appropriate response to AMI, we conducted a logistic regression analysis including age, gender, education and intervention status (i.e. EMT-delivery group, direct mail and control group) on appropriate response to AMI (i.e. take aspirin and call 911 as the first two action responses to AMI symptoms). The analysis showed that there were two variables significantly related to the outcome variable: gender and intervention status. Compared to women, men were less likely to intent to respond appropriately to AMI symptoms than women (odds ratio of 0.67, P ⬍ 0.03). Compared to the control group, respondents in the EMT-delivery group and direct mail group were significantly more likely to report intentions to call 911 and take aspirin as a response to AMI symptoms (odds ratios of 6.9 and 3.3, respectively, P ⬍ 0.000). Age and education were not significant in the model. Evaluation of Kit Most people who recalled receiving the Kit could locate the Kit in their home. Although no systematic tally was performed of the open-ended responses as to the location of the Kit, the responses seemed to indicate that the Kits were placed by the phone, on the refrigerator, kitchen cupboard or other place. Respondents remembered the main messages of the Kit. Respondents correctly identified the following messages as being part of the Kit: symptoms of AMI (71%), recommendation to call 911 for symptoms of AMI (78%), recommendation to take aspirin for AMI (80%), CPR instructions (54%) and packet of aspirin (88%). Ninety-one percent reported they liked the Kit and 71% reported the Kit was ‘very’ useful. Almost nobody thought the Kit was very upsetting (0.3%). Discussion The objective of the current study was to investigate the effectiveness of a Heart Attack Survival Kit, designed to increase intentions to respond appropriately to symptoms of acute myocardial infarction. We tested two delivery methods: door- to-door delivery by local firefighters and direct mail. Consistent with our hypotheses, seniors in the intervention groups (EMT-delivery or direct mail) were more likely to report intentions to use prompt and appropriate coping responses to AMI symptoms than seniors in the control group. Most of the difference appeared to stem from differences in intentions to ingest an aspirin for AMI symptoms, rather than differences in intentions to call 911. Intentions to call 911 for heart attack symptoms were high across the groups (around 75%) so a ceiling effect may have contributed to lack of differences among the groups. There were significant differences between intervention and control conditions in people’s intentions to take an aspirin for AMI symptoms. In a related study we found that few people know about the benefits of aspirin for AMI treatment (King County, EMS, unpublished data, 1997). Thus, this new information may have affected people’s intended coping responses. Seniors in the EMT-delivery group differed significantly from seniors in the direct mail group in their ability to recall receiving the Heart Attack Survival Kit. Some of the recall difference between the two groups may have been due to the fact that persons in the direct mail group were, on average, reached by phone several days later (mean of 3.4 weeks) than persons in the EMT-delivery group (mean of 2.4 weeks). However, the analyses which are limited to only those people who report actually having received the Kit show that seniors who received the Kit from a local firefighter were more likely to report intentions to comply with recommended coping strategies, liked the Kit better and were slightly more likely to report they had the Kit in their home than seniors who reported they had received the Kit via direct mail. This suggests that the interpersonal encounter with a firefighter has benefits above and beyond the information that was presented in the Kit itself. To assess the impact of the firefighter visits over time we called back the 138 seniors who reported they had received the kit via a firefighter, a full year after the intervention (i.e. the Spring of 1999). Of the 114 seniors who completed this follow-up 323 H. Meischke et al. survey, 75% recalled the firefighter visit and 76% were able to locate the Kit in their home upon request. Compared to other types of public education interventions in this and related areas (Meischke et al., 1995, 1999) the Heart Attack Survival Kit intervention seems to have a persuasive and lasting impact. Limitations Since this was a small field study it was not possible to obtain outcome data (i.e. actual 911 calls or aspirin use). To obtain such data would require a tremendous number of house visits and medical record surveillance in many hospitals. Thus, the reliance on self-reported intentions as a proxy for actual behavior during a heart emergency. Only a randomized community trial will be able to assess the impact of the Heart Attack Survival Kit and its delivery methods on actual behavior change. Since the labor intensity of the project might prohibit a large-scale program we interviewed the firefighters involved in the project about the potential benefits of such a project to them. Reports from the three participating firefighters were unanimously positive. The firefighters felt elated to meet and educate seniors in their community in a ‘non-crisis’ situation. In many cases firefighters were successful in actually taping the Kit in the seniors’ home in a visible place. Although door-to-door delivery of health information by firefighters may be labor intensive we believe this public education strategy is feasible and fits with the mission of EMS. Fire departments have been facing the dilemma of decreasing fire calls in the past decades, due to automatic sprinklers, improved fire-safe building design and construction, smoke detectors, tougher building and fire codes, better enforcement of those codes, and public fireeducation programs (Page, 1990; Gresham, 1994). However, most fire departments have adopted additional roles/services including fire prevention and education programs, and also with emergency responses (Page, 1990). In 1995, the National Highway Traffic Safety Administration (NHTSA), in partnership with the Health Resources and Services Administration (HRSA), Maternal and 324 Child Health Bureau (MCHB) commissioned the development of the EMS Agenda for the Future, in order to determine the most important directions for future EMS development (Delbridge et al., 1998). Of the 14 EMS attributes, identified as requiring continued development, two areas seem particularly relevant to the current project: (1) the continued and expanded role of EMS in public education, and (2) the role of EMS in prevention activities. We believe that the Heart Attack Survival Kit project is a public education activity that fits this agenda. Innovative techniques must be tried since the traditional public health interventions for heart disease have been largely ineffective. The consent procedures between the two intervention groups differed. Twelve percent of the study participants in the EMT-delivery group returned a post card indicating they did not want to receive a visit by a firefighter. We did not have such a procedure for participants in the direct mail intervention. Although this may have introduced a selection bias in our EMT-delivery group, we believe this bias is minimal for two reasons. First, 20% of the returned post cards included reasons for non-participation which did not reflect unwillingness to be visited, such as: too young, deceased, wrong address or to the fact that participants knew they would not be home (on vacation) in the next couple of weeks. Second, although we did not include the people who returned a post card in the intervention, these people were included in our follow-up telephone survey. If anything the inclusion of these participants may have diluted the intervention effect in the EMT-delivery group since they were excluded from the intervention. For future study consent procedures for differing intervention strategies need to as similar as possible to increase scientific rigor. The results of this study show that the Heart Attack Survival Kit was perceived as useful by the target audience and did affect seniors’ intentions to act in a prompt and appropriate response. It also shows that exposure to the Kit and intentions to act in the recommended ways were greatest in the EMT-delivered intervention group. The effects The ‘Heart Attack Survival Kit’ project were particularly strong for the message on aspirin ingestion during a heart emergency. The firefighters participating in this research project were extremely supportive and enthusiastic about the project. Other fire districts may not be as supportive. Thus, a larger scale study including multiple fire districts will teach us a great deal about the effectiveness of firefighters as public health educators in different systems. Acknowledgements We are grateful for the unequivocal support we received from Chief Angelo, Chief of Kent fire district in implementing this field study in a timely manner. We are also thankful for the enthusiastic help we received from the three firefighters (Brian Kingery, Brian Felczak and Mike Richardson) who participated in this project. We thank the Medic One Foundation for the financial support for this project. References American Heart Association (1996) Heart and Stroke Facts. Statistical Supplement. AHA, Dallas, TX. Blohm, M., Hartford, M., Karlson, B. W., Karlsson, T. and Herlitz, J. (1994) A media campaign aiming at reducing delay times and increasing the use of ambulance in AMI. American Journal of Emergency Medicine, 12, 315–318. Blohm, M. B., Hartford, M., Karlson, B. W., Leupker, R. V. and Herlitz, J. (1996) An evaluation of the results of media and educational campaigns designed to shorten the time taken by patients with acute myocardial infarction to decide to go to hospital. Heart, 76, 430–434. Collins, R., Peto, R., Baigent, C. and Sleight, P. (1997) Aspirin, heparin, and fibrinolytic therapy in suspected acute myocardial infarction. New England Journal of Medicine, 20, 847–860. Delbridge, T. R., Bailey, B., Chew, J. L., Conn, A. K. T., Krakeel, J. J., Manz, D., Miller, D. R., O’Malley, P. J., Ryan, S. D., Spaite, D. W., Stewart, R. D., Suter, R. E. and Wilson, E. M. (1998) EMS Agenda for the future: where we are... where we want to be. Prehospital Emergency Care, 2, 1–13. Dracup, K., Moser, D. K., Eisenberg, M. S., Meischke, H., Alonzo, A. and Braslow, A. (1995) Causes of delay in seeking treatment for heart attack symptoms. Social Science and Medicine, 40, 379–392. Eisenberg, M. J. and Topol, E. J. (1996) Prehospital administration of aspirin in patients with unstable angina or acute myocardial infarction. Archives of Internal Medicine, 156, 1506–1510. Eppler, E., Eisenberg, M. S., Schaeffer, S., Meischke, H. and Larsen, M. P. (1994) 911 and emergency department utilization for chest pain: results of a media campaign. Annals of Emergency Medicine, 24, 202–208. Fuster, V., Dyken, M. L., Vokonas, P. S. and Hennekens, C. (1993) Aspirin as a therapeutic agent in cardiovascular disease. Circulation, 87, 659–675. Gaspoz, J. M., Unger, P. F., Urban, P., Chevrolet, J. C., Rutishauser, W., Lovis, C., Goldman, L., Heliot, C., Sechaud, L., Mischler, S. and Waldvogel, F. A. (1996) Impact of a public campaign on pre-hospital delay in patients reporting chest pain. Heart, 76, 150–155. Gresham, R. (1994) Does EMS belong in the fire service? Emergency Medical Services, March, 47–55. Grim, P. S., Feldman, T. and Childers, R. W. (1989) Evaluation of patients for the need of thrombolytic therapy in the prehospital setting. Annals of Emergency Medicine, 18, 483–488. Hennekens, C. H., Dyken, M. L. and Fuster, V. (1997) Aspirin as a therapeutic agent in cardiovascular disease. A statement for healthcare professionals from the American Heart Association. Circulation, 96, 2751–2753. Hennekens, C. H., Jonas, M. A. and Buring, J. E. (1994) The benefits of aspirin in acute myocardial infarction. Still a well-kept secret in the United States. Archives of Internal Medicine, 154, 37–39. Herlitz, J., Blohm, M., Hartford, M., Karlson, B. W., Leupker, R., Holmberg, S., Risenfors, M. and Wennerblom, B. (1992) Follow-up of a 1-year media campaign on delay times and ambulance use in suspected acute myocardial infarction. European Heart Journal, 13, 172–177. Ho, M. T. (1991) Delays in treatment of acute myocardial infarction: an overview. Heart and Lung, 20, 566–570. Ho, M. T., Eisenberg, M. S., Litwin, P. E., Schaeffer, S. M. and Damon, S. K. (1989) Delay between onset of chest pain and seeking medical care: the effect of public education. Annals of Emergency Medicine, 18, 727–731. Johnson, J. A. and King, K. B. (1995) Influence of expectations about symptoms on delay in seeking treatment during a myocardial infarction. American Journal of Critical Care, 4, 29–35. Lavrakas, P. J. (1987) Telephone Survey Methods: Sampling, Selection and Supervision (Applied Social Research Methods Series 17). Sage, Newbury Park, CA. Leventhal, H, Nerenz, D. R. and Steele, D. J. (1984) Illness representations and coping with health threats. In Baum, A. and Singer, J. (ed.), A Handbook of Psychology and Health. Erlbaum, Hillsdale. NJ, pp. 219–252. Marder, V. J. and Sherry, S. (1988) Thrombolytic therapy: current status [second of two parts]. New England Journal of Medicine, 318, 1585–1595 Meischke, H., Eisenberg, M. S., Schaeffer, S. M., Damon, S. K., Larsen, M. P. and Henwood, D. K. (1995) Utilization of emergency medical services for symptoms of acute myocardial infarction. Heart and Lung, 24, 11–18. Meischke, H., Durlberg, E. M., Schaeffer, S. S., Henwood, D. K., Larsen, M. P. and Eisenberg, M. S. (1997) ‘Call Fast, Call 911’: a direct mail campaign to reduce patient delay in acute myocardial infarction. American Journal of Public Health, 87, 1705–1709. Meischke, H., Finnegan, J. and Eisenberg, M. S. (1999) What can you teach about cardiopulmonary resuscitation (CPR) in 30 seconds? Evaluation of a television campaign. Evaluation and the Health Professions, 22, 44–60. 325 H. Meischke et al. National Institute of Health (1997) Educational Strategies to Prevent Prehospital Delay in Patients are High Risk for Acute Myocardial Infarction. NHLBI publ. no. 97-3787. NIH, Bethesda, MD. Page, J. O. (1990) Spotting hot trends in Fire Service EMS. Journal of Emergency Medical Services, December, 42–52. Second International Study of Infarct Survival Collaborative Group (1988) Randomised trial of intravenous streptokinase, oral aspirin, both, or neither, among 17187 cases of suspected acute myocardial infarction: ISIS-2. Lancet, ii, 871–874. Weaver, W. D., Eisenberg, M. S., Martin, J. S., Litwin, P. E., Schaeffer, S. M., Ho, M. T., Kudenchuck, P., Hallstrom, A. P., Cerqueira, M. D. and Copass, M. K. (1990) Myocardial 326 Infarction Triage and Intervention Project—phase I: patient characteristics and feasibility of prehospital initiation of thrombolytic therapy. American Journal of Cardiology, 15, 925–931. Yusuf, S, Collins, R., Peto, R., Furberg, C., Stampfer, M. J., Goldhaber, S. Z. and Hennekens, C. H. (1985) Intravenous and intracoronary fibrinolytic therapy in acute myocardial infarction: overview of results on mortality, reinfarction and side effects from 33 randomized controlled trials. European Heart Journal, 6, 556. Received on October 2, 1998; accepted on May 20, 1999