Survey
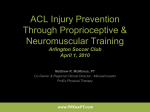
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
JCLB 817 17 March 2003 Disk used No. of Pages 8, DTD = 4.3.1 SPS-N, Chennai ARTICLE IN PRESS Clinical Biomechanics xxx (2003) xxx–xxx www.elsevier.com/locate/clinbiomech 3 Michael A. Hunt a, David J. Sanderson Helene Moffet c, J. Timothy Inglis a 5 6 7 8 c a,b School of Human Kinetics, The University of British Columbia, 210-6081 University Blvd, Vancouver, BC, Canada b ICORD––International Collaboration on Repair Discoveries, Canada Department of Rehabilitation, Faculty of Medicine, Laval University and CIRRIS Research Center, Quebec City, QC, Canada Received 9 October 2002; accepted 26 February 2003 DP 9 Abstract TE Objectives. To identify any changes to lower limb biomechanics during steady rate cycling as a result of an anterior cruciate ligament deficiency. Design. Comparative study in which healthy and anterior cruciate ligament injured individuals underwent biomechanical analysis during stationary cycling. Background. Individuals with an anterior cruciate ligament deficiency often exhibit reductions in the magnitude of quadriceps muscle activity and subsequent knee joint extensor moments during walking. It is not known whether these compensations are present during cycling, an exercise frequently used to retrain anterior cruciate ligament injured individuals. Methods. Ten healthy and 10 unilateral anterior cruciate ligament deficient individuals participated. All participants were required to cycle for approximately 30 s at each of six different cycling intensities while lower limb EMG, kinetics, and kinematics were collected bilaterally. Before riding, participants performed submaximal isometric contractions to generate normalizing data. Results. In addition to reduced quadriceps activation and net knee joint extensor moments, the anterior cruciate ligament deficient limbs exhibited decreases in linear impulse of the resultant pedal force, knee joint flexor moments, hip and ankle extensor moments, and muscle activity from gluteus maximus. These decreases were counteracted by an increase in output from the anterior cruciate ligament intact limb. Conclusion. Anterior cruciate ligament injured individuals exhibited a limb attenuation strategy during cycling activities. EC 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 a,b,* , RO 4 OF Biomechanical changes elicited by an anterior cruciate ligament deficiency during steady rate cycling 2 UN CO RR 25 Relevance This study reports lower limb kinetic and electromyographic data from anterior cruciate ligament deficient individuals 26 during stationary cycling, and shows that these individuals exhibit a limb attenuation strategy on the very leg that is undergoing 27 rehabilitation. 28 Ó 2003 Published by Elsevier Science Ltd. 29 Keywords: Cycling; Anterior cruciate ligament; Quadriceps avoidance 30 1. Introduction 31 32 33 34 35 36 The term ‘‘quadriceps avoidance’’ was coined by Berchuck et al. (1990), who reported a net knee joint flexor moment during the mid-stance phase of gait (10– 30% of the gait cycle) in anterior cruciate ligament (ACL) deficient limbs. This is in contrast to many publications that report that in non-injured individuals * Corresponding author. Address: School of Human Kinetics, The University of British Columbia, 210-6081 University Blvd, Vancouver, BC, Canada V6T 1Z1. E-mail address: [email protected] (D.J. Sanderson). 0268-0033/03/$ - see front matter Ó 2003 Published by Elsevier Science Ltd. doi:10.1016/S0268-0033(03)00046-9 the net knee joint moment during this phase is consistently extensor (e.g. Winter, 1983). Although electromyographic (EMG) data were not collected in the study, Berchuck et al. (1990) proposed that the net flexor moments were the result of a preferential decrease in the magnitude of activation of the quadriceps muscle group. That is, as a result of the injury to the ACL, the individual selectively de-recruited the knee extensor muscles, perhaps as a protection mechanism. Two studies have reported significant reductions in the magnitude of the net knee joint extensor moment (Devita et al., 1997; Chmielewski et al., 2001), while Roberts et al. (1999) reported no change in the magni- 37 38 39 40 41 42 43 44 45 46 47 48 49 JCLB 817 17 March 2003 Disk used 101 2.1. Participants 102 Twenty participants volunteered for the study and gave their informed consent in accordance with the University Ethical Review Board. Ten (five males and five females; mean age: 25.1 (SD 4.7) years) individuals with a unilateral deficiency of the ACL and 10 age and gender-matched healthy uninjured control individuals (mean age: 25.9 (SD 3.4) years) participated. Body proportions of the ACL group (68.9 (SD 10.8) kg body mass, 90.1 (SD 6.0) cm leg length) were similar to the controls (64.4 (SD 9.9) kg body mass, 86.2 (SD 3.1) cm leg length). ACL-injured individuals presented with a unilateral rupture of the ACL, as diagnosed by positive Lachman and anterior drawer tests, at a mean time of 10.7 (SD 13.9) months post-injury, were capable of full knee joint range of motion, and were pain-free during everyday activity. 103 104 105 106 107 108 109 110 111 112 113 114 115 116 117 118 2.2. Experimental task 119 Participants performed six randomized bouts of stationary cycling at intensities comprised of two cadences (60 and 90 rpm) and three power outputs generally used in an ACL injury rehabilitation program (75, 125, and 175 W). EMG, bi-directional pedal reaction force, and kinematic data were collected bilaterally for a total of 18 s after the participants reached the correct cadence and were able to maintain it (5%) at the pre-chosen power output. The total time required for each trial did not exceed 2 min and adequate rest was given between trials, negating any effects of fatigue for the riders. 120 121 122 123 124 125 126 127 128 129 130 2.3. Instrumentation 131 Participants rode on a standard racing bicycle mounted on a Velodyne Trainer (Schwinn, Chicago, IL, USA) which enabled manipulation of power output, while cadence was monitored using a Cateye cyclocomputer (Cateye Co., Boulder, CO, USA) attached to the bicycle. Seat height was manipulated such that the vertical distance from the seat to the pedal at bottomdead-center (BDC) was equal to the vertical distance from the subjectÕs greater trochanter to the floor (Nordeen-Snyder, 1977). Crank position data were collected using a photoelectric cell positioned at top-dead-center (TDC) for the left pedal, which gave an analog pulse when triggered. Pedal angle (with respect to the crank) data were collected continuously using a Dynapar digital encoder (Danaher Controls, Gurnee, IL, USA) attached to each pedal. EMG data were collected from the muscle belly of rectus femoris, vastus lateralis, biceps femoris, and semitendinosis using bipolar surface electrodes (Thera- 132 133 134 135 136 137 138 139 140 141 142 143 144 145 146 147 148 149 150 RO OF 2. Methods EC TE tude of the net knee joint moments in a similar design. Evidence of a preferential decrease in quadriceps muscle activation comes from EMG studies reporting significantly reduced quadriceps muscle activity in ACL-deficient individuals during gait (Limbird et al., 1988; van Lent et al., 1994). However, these reported decreases in quadriceps muscle activity did not always occur during the mid-stance phase associated with the reduced net knee joint extensor moments. Because calculated joint moments are net moments, they reflect the activity of agonist and antagonist muscles. Reported reduced net knee joint extensor moments may also occur as a consequence of increased flexor muscle activity. In fact, increases in hamstring muscle activation have also been reported in ACL-deficient individuals during gait (Limbird et al., 1988). However, the timing during which these increases occurred did not always coincide with the reductions in the net knee joint extensor moments. It would seem that these variations in joint moments and muscle activation reflect a more complex interaction of muscle strength, integrity, and neuromuscular control. One difficulty in exploring this phenomenon is the many degrees of freedom of movement associated with walking. Consequently, we considered an alternate model. Stationary cycling is an activity that is similar to walking in that both walking and cycling require––in alternating phases of propulsion and recovery––output from both limbs for forward propulsion. Similarity in the patterns of joint kinematics, joint moments of force (Winter, 1983; Gregor et al., 1985), and patterns of muscle activation for the quadriceps, hamstrings, and gluteus maximus (Winter, 1984; Mohr et al., 1981) lend strength to the efficacy of using cycling as a means to explore quadriceps avoidance. Coincidentally, stationary cycling is a common exercise used in rehabilitation programs for an ACL rupture as it has been proposed to increase cardiovascular endurance, knee joint range of motion, and lower limb muscular strength (McLeod and Blackburn, 1980). However, no studies have been published that have reported the biomechanical characteristics of ACL-deficient individuals during cycling exercise. The purpose of the present study was to examine the kinetic, EMG, and kinematic patterns in ACL-deficient individuals during stationary cycling. We propose that this model will provide an effective means to explore the notion of quadriceps avoidance. Further, it was postulated that ‘‘quadriceps avoidance’’, specifically, reduced net knee joint extensor moments and reduced quadriceps muscle activity, would be present during stationary cycling. UN CO RR 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65 66 67 68 69 70 71 72 73 74 75 76 77 78 79 80 81 82 83 84 85 86 87 88 89 90 91 92 93 94 95 96 97 98 99 100 M.A. Hunt et al. / Clinical Biomechanics xxx (2003) xxx–xxx DP 2 No. of Pages 8, DTD = 4.3.1 SPS-N, Chennai ARTICLE IN PRESS JCLB 817 17 March 2003 Disk used No. of Pages 8, DTD = 4.3.1 SPS-N, Chennai ARTICLE IN PRESS M.A. Hunt et al. / Clinical Biomechanics xxx (2003) xxx–xxx 205 206 207 208 209 210 2.5. Statistical analysis 211 OF complete cycle. Subject averages were computed as the average over 15 consecutive cycles. Group averages were then calculated for each of four limbs: control individuals right limb (CON R), control individuals left limb (CON L), ACL individuals intact (ACL I), and ACL individuals deficient limb (ACL D). 212 213 214 215 216 217 3. Results 218 DP RO All variables were analyzed separately using a 4 (limb) 2 (cadence) 3 (power output) mutifactorial analysis of variance (A N O V A ) with repeated measures on the last two factors. Significant F -ratios were further analyzed with a Tukey HSD post-hoc test and differences were classified based on a significance level of 0.05. 3.1. Muscle EMG 219 Average normalized iEMG values for a single cycle are shown in Fig. 1a–e. Significant differences were exhibited between limbs for rectus femoris (F3;36 ¼ 21:87, P < 0:001), vastus lateralis (F3;36 ¼ 14:53, P < 0:001), and gluteus maximus (F3;36 ¼ 5:65, P ¼ 0:003), while no differences existed for the two hamstring muscles: biceps femoris (F3;36 ¼ 1:84, P ¼ 0:157) and semitendinosis (F3;36 ¼ 1:13, P ¼ 0:348). Post-hoc analysis revealed that compared to control limbs, ACL intact limbs exhibited greater muscle activation for the rectus femoris and vastus lateralis muscles, while ACL-deficient limbs showed less activation for the rectus femoris, vastus lateralis, and gluteus maximus muscles. Although the magnitudes of EMG activation levels were different between limbs for certain muscles, the general pattern and timing of the activation were similar between limbs and across cycling intensities (Fig. 2a–e). 220 221 222 223 224 225 226 227 228 229 230 231 232 233 234 235 236 3.2. Pedal forces 237 Linear impulses, calculated from the resultant forces data, are summarized in Fig. 3. A significant limb effect was observed (F3;36 ¼ 15:87, P < 0:001), and post-hoc analysis revealed that for all intensities the impulse of the two control limbs were less than the ACL intact limbs (left limb: P ¼ 0:042, right limb: P ¼ 0:013), greater than the ACL-deficient limbs (left limb: P ¼ 0:001, right limb: P ¼ 0:005), while not being significantly different from each other. 238 239 240 241 242 243 244 245 246 3.3. Joint moments 247 EC TE peutics Unlimited, Iowa City, IA, USA). EMG data were also collected from the muscle belly of gluteus maximus using pre-gelled surface electrodes (Red Dot 2259, 3M Company, Borken, Germany) and an Octopus AMT-8 amplifier (Bortec, Calgary, AB, Canada). Prior to electrode application, the designated area was shaved and cleansed with alcohol to reduce electrical impedance. Raw EMG data were collected at 600 Hz using a Data Translation 3010 analog-to-digital (A/D) converter (Data Translation, Marlboro, MA, USA) and a Peak Performance Technologies Data Acquisition System (Peak Performance Inc., Denver, CO, USA). Prior to testing, participants were required to perform a submaximal isometric contraction with each muscle to generate normalizing data. With the participants seated, a strap was placed around the lower limb at the height of the lateral malleolus, and participants were instructed to maintain a force of 75 N with visual feedback as measured by a force transducer (Artech S-Beam, Riverside, CA, USA). Each bicycle pedal was instrumented with two force transducers (Kistler Instruments, Winterthur, Switzerland) capable of measuring normal (Fz ) and shear (Fy ) forces applied to the top of the pedal as has been previously used in the lab (Sanderson et al., 2000). Kinetic data were also collected using the Data Translation A/D converter and Peak acquisition system. Kinematic data were collected at a sampling rate of 60 Hz using the peak acquisition system and two cameras, positioned 3 m from the sagittal plane of the bicycle. Reflective markers were placed bilaterally on the skin overlying the greater trochanter, lateral femoral condyle, lateral malleolus, lateral aspect of the calcaneus, and the lateral aspect of the fifth metatarsal. Reflective markers were also placed over the lateral aspect of the force transducers to denote the center of pressure of force application. Raw coordinate data were acquired by digitizing each frame for each of the 18 second data collection periods. UN CO RR 151 152 153 154 155 156 157 158 159 160 161 162 163 164 165 166 167 168 169 170 171 172 173 174 175 176 177 178 179 180 181 182 183 184 185 186 187 188 189 3 190 2.4. Data reduction 191 192 193 194 195 196 197 198 199 200 201 202 203 204 All raw data (rectified EMG, kinetic, raw coordinate data) were filtered using a 4th-order low-pass Butterworth filter with a cut-off frequency of 4 Hz. Raw coordinate data were used to calculate segmental center of mass (COM) coordinates, joint angles, as well as segmental linear and angular velocities and accelerations to be combined with kinetic data to calculate joint moments of force using conventional inverse dynamics principles. Linear impulse was calculated from the resultant force vector applied to each pedal for a complete cycle (TDC to subsequent TDC). A ratio of filtered task EMG to filtered normalization EMG was calculated for each data point and then used to integrate the magnitude of the signal (iEMG) for each muscle for each Peak moments were analyzed for the hip, knee, and 248 ankle joints and are reported in Table 1. Significant limb 249 effects occurred for peak ankle extensor (F3;36 ¼ 25:03, 250 JCLB 817 17 March 2003 Disk used M.A. Hunt et al. / Clinical Biomechanics xxx (2003) xxx–xxx UN CO RR EC TE DP RO OF 4 No. of Pages 8, DTD = 4.3.1 SPS-N, Chennai ARTICLE IN PRESS Fig. 1. Group mean (SD) integrated EMG values for the 175 W and 60 rpm condition. Values shown are the ratio of EMG collected during riding to EMG collected during the normalizing contractions for rectus femoris (RF), vastus lateralis (VL), biceps femoris (BF), semitendinosis (ST), and gluteus maximus (GM) for each of the four limbs: CON L, control left; CON R, control right; ACL I, ACL intact; ACL D, ACL deficient. 251 252 253 254 255 256 257 258 259 P < 0:001), knee flexor (F3;36 ¼ 20:22, P < 0:001), and hip extensor (F3;36 ¼ 21:86, P < 0:001) moments. Posthoc analysis revealed that in all cases where significant limb effects were reported, no asymmetry was reported between control limbs, while significant asymmetries occurred between limbs of ACL-deficient individuals. All asymmetries exhibited in ACL injured individuals were the result of the peak joint moment in the ACL intact limb being significantly larger than the ACL-deficient limb. 260 3.4. Joint kinematics 261 Although there was a tendency for ACL individuals 262 to exhibit greater thigh extension, less knee extension, and less ankle plantarflexion, no significant differences were observed between limbs for maximum thigh extension (F3;36 ¼ 1:47, P ¼ 0:239), maximum knee extension (F3;36 ¼ 1:51, P ¼ 0:229), or maximum ankle plantarflexion (F3;36 ¼ 0:731, P ¼ 0:540). 263 264 265 266 267 4. Discussion 268 Results from the present study provide evidence for a quadriceps avoidance strategy in ACL-deficient limbs during cycling similar to that reported during walking (Berchuck et al., 1990). ACL-deficient limbs exhibited a measurable reduction (although not statistically signifi- 269 270 271 272 273 JCLB 817 17 March 2003 Disk used No. of Pages 8, DTD = 4.3.1 SPS-N, Chennai ARTICLE IN PRESS 5 UN CO RR EC TE DP RO OF M.A. Hunt et al. / Clinical Biomechanics xxx (2003) xxx–xxx Fig. 2. Group mean EMG ensemble averages with respect to crank angle for control (solid lines), ACL intact (dotted line), and ACL-deficient (dashed line) limbs for the 175 W and 60 rpm condition. Values on the vertical axis are the normalized data. Graphs correspond to rectus femoris (A), vastus lateralis (B), biceps femoris (C), semitendinosis (D), and gluteus maximus (E) muscles. 274 275 276 277 278 279 280 281 282 283 284 285 286 287 cant) in the magnitude of the peak net knee joint extensor moment. This occurred due to reductions in rectus femoris and vastus lateralis muscle activity and no change in hamstrings (biceps femoris and semitendinosis) activity. However, in contrast to walking, where increased hip or ankle extensor moments have been reported in ACL-deficient limbs to compensate for the reduced knee joint extensor moment (Berchuck et al., 1990; Chmielewski et al., 2001; Roberts et al., 1999), ACL-deficient individuals in the present study tended to reduce output across the entire injured limb. This apparent limb attenuation was manifested in significant decreases in the linear impulse of the resultant pedal force, maximum extensor moments at the hip and ankle and flexor moment at the knee, and magnitude of muscle activation in rectus femoris, vastus lateralis, and gluteus maximus in ACL-deficient limbs compared to uninjured limbs. The differences exhibited were not due a change in movement path since the ranges of motion about all three lower limb joints were similar between injured and uninjured limbs. Further, the timing and general pattern of muscle activation was similar for all limbs (Fig. 2), suggesting that a similar motor program was used for all limbs. It has been suggested that changes in knee joint biomechanics in ACL-deficient individuals during gait occur as a result of decreased stability within the knee joint due to increased anterior tibial translation (Ber- 288 289 290 291 292 293 294 295 296 297 298 299 300 301 JCLB 817 17 March 2003 Disk used M.A. Hunt et al. / Clinical Biomechanics xxx (2003) xxx–xxx RO OF Impulse (Ns) 6 No. of Pages 8, DTD = 4.3.1 SPS-N, Chennai ARTICLE IN PRESS Cycling Condition Table 1 Group mean (SD) peak extensor and flexor moments 125/60 88.5 (13.9) 92.9 (15.3) 106.3 (12.7) 76.1 (15.2) 114.4 (20.0) 116.4 (19.9) 135.3 (20.2) 90.5 (12.9) Knee CON L CON R ACL I ACL D 8.8 (3.6) 8.8 (4.5) 11.1 (3.4) 7.6 (4.7) 7.9 (6.6) 7.4 (6.4) 13.4 (5.6) 8.5 (6.3) Ankle CON L CON R ACL I ACL D 23.9 23.6 28.2 19.4 (3.3) (3.3) (3.1) (3.8) 33.6 32.0 37.3 25.5 Flexor Hip CON L CON R ACL I ACL D 15.2 18.1 21.1 12.6 (8.6) (11.0) (6.8) (9.6) Knee CON L CON R ACL I ACL D 42.7 42.6 44.4 26.3 Ankle CON L CON R ACL I ACL D -2.1 -2.0 -2.8 -2.5 175/60 75/90 TE 75/60 Extensor Hip CON L CON R ACL I ACL D DP Fig. 3. Group mean (SD) data for linear impulse for each of the six conditions. Symbols indicate control left (r), control right (j), ACL intact (N), and ACL-deficient () limbs. 125/90 175/90 72.7 (14.7) 83.7 (14.2) 105.7 (15.5) 70.3 (10.6) 108.5 (16.1) 115.5 (14.1) 129.3 (17.5) 84.1 (23.6) 138.6 139.5 153.3 109.1 12.5 (8.0) 16.4 (8.0) 13.6 (6.9) 9.2 (8.6) 9.3 (3.2) 10.6 (3.4) 15.3 (5.8) 11.4 (3.2) 13.8 14.9 17.9 12.1 (5.9) (6.1) (7.1) (5.1) 17.2 20.3 17.6 13.7 (5.5) (6.7) (6.3) (6.0) (4.9) (4.0) (4.3) (3.9) 40.3 39.2 45.1 30.6 (4.0) (3.3) (7.6) (7.1) 24.2 24.5 32.6 23.8 (3.2) (4.2) (5.5) (4.4) 31.7 30.7 35.3 25.1 (3.5) (1.7) (3.9) (3.8) 40.1 38.3 41.4 30.7 (5.7) (5.6) (8.8) (5.7) 17.3 20.4 23.2 20.6 (11.0) (10.3) (6.6) (13.9) 27.1 32.1 31.2 31.7 (15.3) (17.6) (15.3) (11.1) 16.1 27.1 27.5 20.0 (9.3) (11.2) (9.9) (6.6) 24.5 25.7 25.5 24.9 (16.1) (14.1) (12.0) (6.6) 27.3 35.7 29.8 20.5 (19.1) (12.7) (11.1) (9.3) (9.6) (9.2) (12.6) (6.4) 49.9 49.8 57.4 38.9 (9.0) (6.2) (11.8) (9.0) 59.3 58.4 56.9 33.8 (8.1) (7.6) (13.2) (10.2) 31.8 34.4 43.6 27.3 (5.4) (6.0) (11.9) (6.5) 42.2 43.6 51.6 32.8 (5.9) (6.0) (9.4) (8.1) 59.4 60.1 64.8 39.5 (11.1) (9.7) (9.0) (7.4) (0.9) (1.4) (2.1) (1.3) )0.9 )1.2 )1.0 )1.5 (0.7) (1.2) (2.0) (2.4) 0.8 0.3 0.8 0.4 )1.3 )0.1 )1.3 )0.2 (0.8) (1.4) (2.0) (1.4) )1.7 )1.5 )1.9 )0.9 (0.9) (2.6) (2.2) (1.5) )1.1 (1.0) 0.1 (1.0) )0.8 (2.3) )0.1 (2.1) UN CO RR EC 141.8 (18.1) 141.6 (20.2) 154.9 (9.1) 99.4 (9.3) (1.2) (2.2) (2.7) (2.7) Values are in N m. denotes a significantly decreased peak joint moment in ACL-deficient limbs compared to ACL intact limbs (P < 0:05). * (16.0) (16.5) (16.3) (15.5) JCLB 817 17 March 2003 Disk used No. of Pages 8, DTD = 4.3.1 SPS-N, Chennai ARTICLE IN PRESS M.A. Hunt et al. / Clinical Biomechanics xxx (2003) xxx–xxx 358 359 360 361 362 363 364 365 366 367 368 369 370 371 372 373 374 375 376 377 378 379 380 381 382 383 384 385 386 5. Conclusions 387 Results from the present study indicate that a pattern similar to the quadriceps avoidance strategy observed in gait (decreased quadriceps muscle activation, decreased knee joint extensor moment) also occurs during stationary cycling. However, during cycling injured individuals exhibited a limb attenuation of the entire ACLdeficient limb that was manifested in decreases in extensor moments at the hip, knee, and ankle, as well as muscle activity from the quadriceps and gluteus maximus muscles. We believe that this limb attenuation is unique to cycling and only possible because an increase in output from the contralateral limb can maintain output at the crank in light of decreased output from the injured limb. Understanding this phenomenon is important because this limb attenuation strategy occurs on the very leg that is undergoing rehabilitation. 388 389 390 391 392 393 394 395 396 397 398 399 400 401 402 403 6. Uncited reference 404 Winter (1980). 405 DP RO OF similar to all other limbs. This large asymmetry between limbs in the ACL group is in contrast to gait, where a decrease in output from the ACL intact limbs––in order to maintain symmetry with the decreased output from the injured limb––has been reported (van Lent et al., 1994). A decrease in output from both limbs in the ACL group was impossible in this study as the force imparted to the crank must have remained constant to maintain the proper power output at each cadence. One of the most important aspects of a rehabilitation program is the formation of new motor programs in order to compensate for the injury (Kvist and Gillquist, 2000). If an ACL-deficient individual learns a limb avoidance strategy early in their rehab program this strategy could somehow manifest itself to a lesser extent in other movements. Based on the results from the present study, there appears to be similar biomechanical compensations in ACL-deficient limbs during stationary cycling and walking suggesting that cycling may be an effective model to examine quadriceps avoidance. Since stationary cycling is an integral part of early rehabilitation for this injury, it is possible that the quadriceps avoidance pattern observed during walking may be associated with compensations made early during the rehabilitation period, and stationary cycling in particular. However, this is speculation and further research is required to examine this possible connection especially as the goal of any rehabilitation strategy is to return the limb to full function. EC TE chuck et al., 1990; Devita et al., 1997; Ferber et al., 2002). In order to decrease the tibial translation, it has been argued that individuals with an ACL deficiency reduce the quadriceps activation, which will act to pull the tibia forward, while increasing hamstrings activation (a known ACL synergist McNair et al., 1992; More et al., 1993; Imran and OÕConnor, 1998; Liu and Maitland, 2000), which will act to pull the tibia backward, at a time when anterior tibial translation is known to be largest during gait (Marans et al., 1989; Lafortune et al., 1992; Kvist and Gillquist, 2000). These strategies will, therefore, result in a more flexed knee and a decreased knee joint extensor moment. The amount of anterior tibial translation is not known during cycling, but can be estimated based on tibiofemoral shear force (Neptune and Kautz, 2000) and ACL strain (Fleming et al., 1998) data. It is known that both tibiofemoral shear force and ACL strain are largest during the propulsive phase of cycling, which would suggest that anterior tibial translation is also largest at that time. It is also known that larger forces at the pedal result in increased anterior translation (Fleming et al., 2001). Therefore, a simple strategy to decrease the amount of anterior tibial translation during stationary cycling would be to decrease the magnitude of the force exerted to the pedal by the ACL-deficient limb during propulsion, which is what was found in this study. If the extensor output at the knee joint is decreased during walking in ACL-deficient individuals in order to maintain tibial positioning, then compensations must be made at the other joints to maintain an adequate support moment as well as forward propulsion (Winter, 1983). It has been shown that ACL-deficient individuals increase the magnitude of the hip (Berchuck et al., 1990; Roberts et al., 1999) or ankle (Chmielewski et al., 2001) extensor moment during mid-stance to compensate for the decreased extensor moment about the knee. This prevents the individual from falling down and helps maintain adequate propulsion from the injured limb. That a compensation at the hip or ankle joint was not observed in the present study is likely due to two fundamental differences between walking and cycling. First, the weight of the body is supported by the bicycle seat. Therefore, the maintenance of a support moment is not necessary. Second, since both pedals are connected to the crank, it is possible for a lack of propulsion from one leg to be compensated for by an increase in propulsion from the other limb. In the present study, a limb attenuation in the ACLdeficient limbs, where output was decreased to limit the amount of anterior tibial translation, was possible because the decrease in output from the ACL-deficient limb was counteracted by increased output from the ACL intact limb. Significant increases were observed in the ACL intact limbs in all variables except for biceps femoris and semitendinosis activation levels, which were UN CO RR 302 303 304 305 306 307 308 309 310 311 312 313 314 315 316 317 318 319 320 321 322 323 324 325 326 327 328 329 330 331 332 333 334 335 336 337 338 339 340 341 342 343 344 345 346 347 348 349 350 351 352 353 354 355 356 357 7 JCLB 817 17 March 2003 Disk used 8 M.A. Hunt et al. / Clinical Biomechanics xxx (2003) xxx–xxx UN CO RR RO DP EC TE Berchuck, M., Andriacchi, T.P., Bach, B.R., Reider, B., 1990. Gait adaptations by patients who have a deficient anterior cruciate ligament. J. Bone Joint. Surg. 72-A, 871–877. Chmielewski, T.L., Rudolph, K.S., Fitzgerald, G.K., Axe, M.J., Snyder-Mackler, L., 2001. Biomechanical evidence supporting a differential response to acute ACL injury. Clin. Biomech. 16, 586– 591. Devita, P., Hortobagyi, T., Barrier, J., Torry, M., Glover, K.L., Speroni, D.L., Money, J., Mahar, M.T., 1997. Gait adaptations before and after anterior cruciate ligament reconstruction surgery. Med. Sci. Sports Exerc. 29, 853–859. Ferber, R., Osternig, L.R., Woollacott, M.H., Wasielewski, N.J., Lee, J., 2002. Gait mechanics in chronic ACL deficiency and subsequent repair. Clin. Biomech. 17, 274–285. Fleming, B.C., Beynnon, B.D., Renstrom, P.A., Peura, G.D., Nichols, C.E., Johnson, R.J., 1998. The strain behaviour of the anterior cruciate ligament during bicycling: an in vivo study. Am. J. Sports Med. 26, 109–118. Fleming, B.C., Renstrom, P.A., Beynnon, B.D., Engstrom, B., Peura, G.D., Badger, G.J., Johnson, R.J., 2001. The effect of weightbearing and external loading on anterior cruciate ligament strain. J. Biomech. 34, 163–170. Gregor, R.J., Cavanagh, P.R., Lafortune, M., 1985. Knee flexor moments during propulsion in cycling––A creative solution to LombardÕs paradox. J. Biomech. 18, 307–316. Imran, A., OÕConnor, J.J., 1998. Control of knee stability after ACL injury or repair: interaction between hamstrings contraction and tibial translation. Clin. Biomech. 13, 153–162. Kvist, J., Gillquist, J., 2000. Anterior positioning of tibia during motion after anterior cruciate ligament injury. Med. Sci. Sports Exerc. 33, 1063–1072. Lafortune, M.A., Cavanagh, P.A., Sommer, H.J., Kalenka, A., 1992. Three-dimensional kinematics of the human knee during walking. J. Biomech. 25, 347–357. Limbird, T.J., Shiavi, R., Frazer, M., Borra, H., 1988. EMG profiles of knee joint musculature during walking: changes induced by anterior cruciate ligament deficiency. J. Orthop. Res. 6, 630–688. Liu, W., Maitland, M.E., 2000. The effect of hamstring muscle compensation for anterior laxity in the ACL-deficient knee during gait. J. Biomech. 33, 871–879. Marans, H.J., Jackson, R.W., Glossop, N.D., Young, C., 1989. Anterior cruciate ligament insufficiency: a dynamic three-dimensional motion analysis. Am. J. Sports Med. 17, 325–332. McLeod, W.D., Blackburn, T.A., 1980. Biomechanics of knee rehabilitation with cycling. Am. J. Sports Med. 8, 175–180. McNair, P.J., Wood, G.A., Marshall, R.N., 1992. Stiffness of the hamstring muscles and its relationship to function in the anterior cruciate ligament deficient individuals. Clin. Biomech. 7, 131–137. Mohr, T.M., Allison, J.D., Patterson, R., 1981. Electromyographic analysis of the lower extremity during pedaling. J. Orthop. Sports Phys. Ther. 2, 163–170. More, R.C., Karras, B.T., Neiman, R., Fritschy, D., Woo, S.L., Daniel, D.M., 1993. Hamstrings––an anterior cruciate ligament protagonist. Am. J. Sports Med. 21, 231–237. Neptune, P.R., Kautz, S.A., 2000. Knee joint loading in forward versus backward pedaling: implications for rehabilitation strategies. Clin. Biomech. 15, 528–535. Nordeen-Snyder, K.S., 1977. The effect of bicycle seat height variations upon oxygen consumption and lower limb kinematics. Med. Sci. Sports Exerc. 9, 113–117. Roberts, C.S., Rash, G.S., Honaker, J.T., Wachowiak, M.P., Shaw, J.C., 1999. A deficient anterior cruciate ligament does not lead to quadriceps avoidance gait. Gait Posture 10, 189–199. Sanderson, D.J., Hennig, E.M., Black, A.H., 2000. The influence of cadence and power output on force application and in-shoe pressure distribution during cycling by competitive and recreational cyclists. J. Sports Sci. 18, 173–181. van Lent, M.E.T., Drost, M.R., Wildenberg, F.A.J.M., 1994. EMG profiles of ACL-deficient patients during walking: the influence of mild fatigue. Int. J. Sports Med. 15, 508–514. Winter, D.A., 1980. Overall principle of lower limb support during stance phase of gait. J. Biomech. 13, 923–927. Winter, D.A., 1983. Biomechanical motor patterns in normal walking. J. Mot. Behav. 15, 302–330. Winter, D.A., 1984. Pathologic gait diagnosis with computer-averaged electromyographic profiles. Arch. Phys. Med. Rehabil. 65, 393– 398. OF 406 References 407 408 409 410 411 412 413 414 415 416 417 418 419 420 421 422 423 424 425 426 427 428 429 430 431 432 433 434 435 436 437 438 439 440 441 442 443 No. of Pages 8, DTD = 4.3.1 SPS-N, Chennai ARTICLE IN PRESS 444 445 446 447 448 449 450 451 452 453 454 455 456 457 458 459 460 461 462 463 464 465 466 467 468 469 470 471 472 473 474 475 476 477 478 479 480 481 482 483