Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
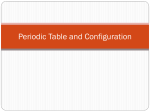
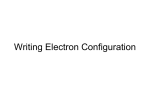
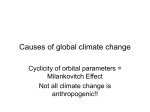
MRI of unilateral vertical retraction syndrome with atypical strabismus Chengyue ZHANG 1, Fengyuan MAN2, Zhenchang WANG2, Gang YU1, Qian WU1, Yonghong JIAO3 and Kanxing ZHAO4 1 Ophthalmology of Beijing children's hospital affiliated to capital university of medical science, China 2 Beijing Tongren Medical Imaging Centre, Beijing Tongren Hospital, Capital Medical University, China 3 Beijing Tongren Eye Centre, Beijing Tongren Hospital, Capital Medical University, Beijing Ophthalmology and Visual Science Key Lab, China Correspondence to: DongjiaoMinxiang, Dongcheng, District, Beijing, 100730, P.R.China. Tel: 0086 010 58268672 Fax: 0086 010 58269154 E-mail address: [email protected] 4 Tianjin Eye Hospital, Clinical College of ophthalmology, Tianjin Medical University, China BACKGROUND Complicated strabismus cases, especially those accompanied by abnormal eye movements and anomalous innervations often present diagnostic challenges. With the development of Magnetic Resonance Imaging (MRI), we can do more detailed study on the anatomy of ocular motor nerves and their corresponding extraocular muscles (EOMs) [1-3]. Vertical retraction syndrome is a rare kind of strabismus that consists of retraction of the globe with narrowing of the lid fissure in attempted elevation or depression, frequent elevation deficiency with variable retraction of the globe. Two patients with unilateral vertical retraction syndrome confirmed by images were discussed in this study. METHODS MRI was performed with a General Electric 1.5-T Twinspeed scanner. The study was performed in accordance with the declaration of Helsinki. Written informed consents were acquired before MRI. Imaging of the ocular motor nerves in the brainstem was performed by the 3D-FIESTA sequence. Nerves to EOMs, EOMs and their associated connective tissues in the orbits were imaged with a T1-weighted and T2-weighted FSE in triplanar scans by dual-phased coils. Intravenous gadodiamide contrast was administered. RESULTS Case 1 A 7-year-old boy was found to have limitation of elevation of the right eye since 2 years old. His parents denied swelling or bleeding in the orbits at birth. He had no family history of eye disease. The results of systemic and neurologic examination were negative. Cycloplegic refraction was +1. 25DS + 0.50 DC× 70 right eye and +1.25DS + 0.50 DC× 130 left eye. His corrected visual acuities were 12/20 bilaterally. Enophthalmos of the right eye was revealed in the primary position. Limitation of elevation of the right eye was seen in both adduction and abduction which was accompanied by significant narrowing of the palpebral fissure (Figure 1). In the primary position, when the right eye fixated, 10-diopter exotropia and 60-diopters hyperdeviation were present in the left eye. When the left eye fixated, a 25-diopters hypodeviation were present in the right eye. MRI of brainstem showed that CN3 and CN6 in the cistern were normal. Sagittal reconstruction shows a linear band originated from the orbital apex and inserted posteriorly to the equator of the globe in the lower outer quadrant, which appeared slightly lower signal intensity than that of extraocular muscle on T1-weighted images. Contiguous quasicoronal MRI of the right orbit showed the orbital structure was separated from the inferior rectus muscle (IR), the maximum cross-section diameter of the band was about 3mm, and the inferior division of CN3 sent out an enlarged branch to IR (Figure 2). Case 2 An 8-year-old girl which had been reported in another paper had a limitation of elevation of the left eye in both adduction and abduction [4]. She had an intermittent exotropia of 60 prism diopters in the primary position. MRI of the left orbit showed a linear band that originated from the orbital apex and insert on the posterior globe in the inferotemporal quadrant, which appeared slightly lower signal than muscle on T1-weighted images. The maximum cross-section diameter of the band was about 3mm. The inferior division of CN3 to the inferior oblique muscle was not constantly revealed. The abnormal band was indicated to originate from the inferior rectus (IR) at the orbital apex by MRI sagittal reconstruction (Figure 3). DISCUSSION The pathogenesis of the vertical retraction syndrome is still not clearly known. Recent reports including imaging findings revealed that an accessory extraocular muscle or a fibrous band appeared to cause restriction on elevation and globe retraction in their cases [5-7]. Detailed clincopathologic evidence of anomalous orbit structures resulting unusual strabismuses had been reviewed by Gregg T. Lueder [8], and were categorized into three types: 1. structures arise from the extraocular muscles themselves and insert in abnormal locations. 2. fibrous bands located beneath the rectus muscles. 3. discrete anomalous muscles that originate in the posterior orbit and insert in abnormal locations on the globe. In our study, MRI of the two cases showed similar size and location of the orbital structure but differed greatly in type of strabismus. The signal intensity of the linear band was slightly lower than that of extraocular muscle on T1-weighted images, reflecting the larger percentage of fibrous tissue. Tracing the EOMs from the orbital apex by contiguous quasicoronal MRI, the precise origin of the anomalous orbital structure of case 2 could not be ascertained, but the orbital structure of case 1 arising from the inferior rectus was showed clearly. However, MRI sagittal reconstruction shows the band arising from the inferior rectus muscle at the orbital apex in both cases. Normally, the larger inferior division of CN3 and branches to the target EOMs and CN6 could be well depicted in the orbit [1, 3].However, we found that inferior division of CN3 to the inferior oblique muscle could not demonstrated constantly in case 2, an anomalous enlarged branch to IR was revealed in case 1. These MRI observations implied that the anomalous orbital structure was anomalous muscle tissue and innervated by the inferior division of CN3 as Fleischer’s reported [9]. Vertical retraction syndrome caused by abnormal structures may appear as atypical strabismus. Imaging studies of the ocular motor nerves and their corresponding EOMs can play an extremely useful role in the diagnosis, and careful communication with the radiologist may help in their identification. MRI of the orbits of the two cases was originally interpreted similar size and location of the orbital structure in the inferotemporal quadrant. Reevaluation of these MRI studies in light of the type of strabismus differs dramatically showed that the insertions of the band of the two cases were different which might be related to the strabismus. In case 1 the band was inserted at the posterior of the equator of the globe. Ocular motility examination revealed marked enophthalmos in the primary position, large angle hypotropia, and significant limitation of elevation. Therefore the more anterior insertion of abnormal orbital band led to more limitation might explain, at least partially, the cause of hypotripia of this case. The insertion of the band of case 2 was approximately at the posterior pole of the globe which was near the optic nerve. Ocular motility examination showed slight enophthalmos and intermittent exotropia in the primary position. These findings indicated that the terminal of abnormal orbital band ending near the posterior pole of eyeball would cause slight limitation of elevation. In conclusion, anomalous orbital structures may partially explain the cause of vertical retraction syndrome and the anatomical differences of the orbital structures can lead to atypical strabismus. References: 1.Demer JL, Ortube MC, Engle EC, et al. High-resolution magnetic resonance imaging demonstrates abnormalities of motor nerves and extraocular muscles in patients with neuropathic strabismus. J AAPOS. 2006 Apr; 10(2):135-42. PMID:16678748 2.Demer JL, Ortube MC, Lim KH, et al. Magnetic resonance imaging evidence for widespread orbital dysinnervation in dominant Duane's retraction syndrome linked to the DURS2 locus. Invest Ophthalmol Vis Sci. 2007 Jan; 48(1):194-202. PMID: 17197533 3.Jiao YH, Zhao KX, Wang ZC, et al. Magnetic resonance imaging of the ocular motor nerves in normal volunteers. 89 Zhonghua Yan Ke Za Zhi. 2009 Mar;45(3):219-24. PMID:19575915 4. Man F, Wang Z, Wang J, et al. Unilateral vertical retraction syndrome with orbital band. J AAPOS. 2009 Aug; 13(4):419-21. PMID: 19482497 5.Lueder GT, Dunbar JA, Soltau JB, et al. Vertical strabismus resulting from an anomalous extraocular muscle. J AAPOS. 1998 Apr;2(2):126-8.PMID:10530977 6.Murthy R. Unilateral restrictive ophthalmoplegia and enophthalmos associated with an intraorbital tissue band. J AAPOS. 2007 Dec; 11(6):626-7.PMID: 17720574 7.Ozkan SB, Ozsunar Dayanir Y, Gökçe Balci Y. Hypoplastic inferior rectus muscle in association with accessory extraocular muscle and globe retraction. JAAPOS. 2007 Oct; 11(5):488-90.PMID:17933674 8. Lueder GT. Anomalous orbital structures resulting in unusual strabismus. Surv Ophthalmol. 2002 Jan-Feb; 47(1):27-35.PMID:11801267 9. Fleischer. Musculus retractor bulbi und drittes lid bei einer menschlichen missbildung. Anat Ant. 1907; 30:465-70. Figures and legends Figure1. Case 1. Ocular versions showed right hypotropia in the primary position. Limitation of elevation was seen in both adduction and abduction which was accompanied by significant narrowing of the palpebral fissure. Figure2. MRI, Case 1. Contiguous quasicoronal MR Images of the right orbit (A-D). A, The inferior division of CN3 in the orbital apex. B, An enlarged branch to the inferior rectus muscle (IR) was revealed. C, The IR is thickened in the orbital apex. D, the signal intensity of the band is slightly lower than that of the extraocular muscle, and separated from the IR. E, MRI sagittal reconstruction showed a linear band from the orbital apex and inserted on the posterior of the equator of the globe in the lower outer quadrant (black arrows), and the band arising from the inferior rectus muscle at the orbital apex (open arrow). Figure3. MRI, Case 1, 2. A, Quasi-sagittal image through the inferior rectus; B, Quasi-sagittal image through the optic nerve; C, Quasi-sagittal reconstruction of plane A and B, showed a linear band from the orbital apex and inserted on the posterior globe in the lower outer quadrant (arrows).