Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
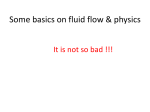
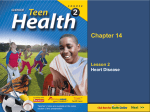
The Cardiovascular System: Anatomy, Physiology, Pathology T hough most of the systems that make up the human body are more or less necessary for normal, healthy function, if not for survival, the circulatory system is uniquely essential. Virtually all tissues except epidermis, cartilage, and dental enamel are richly supplied with blood vessels that deliver oxygen and nutrients and carry away carbon dioxide and other waste products. Significant or prolonged interruption of the blood supply to a tissue, organ, or limb usually results in irreversible damage to at least some cells, and may compromise the entire structure. If a vital organ such as the heart, brain, or kidney is involved, death may ensue. Diseases that affect the circulation are thus among the most significant and serious of all, and their prevention and treatment play a major role in the modern practice of medicine. Within recent years, biomedical research has clarified the intricacies of cardiovascular physiology; gained a fuller understanding of the mechanisms underlying hypertension, atherosclerosis, and congestive heart failure; developed sophisticated diagnostic methods for these and other conditions; and provided increasingly effective methods of prevention and treatment. A brief review of cardiac anatomy and physiology will pave the way for a clearer understanding of these issues. Cardiovascular Anatomy and Physiology The heart consists of two pumps working synchronously side by side and sharing an inner wall in common. Although these two pumps are intimately allied in structure and function, each handles a different component of the total blood volume, and (except in the presence of structural abnormality) mixing of the two circulations does not occur. Each pump consists of two chambers: a relatively thinwalled collecting chamber, or atrium, and the pump proper, or ventricle. Each contraction of a ventricle propels blood through a single large vessel, which branches into increasingly smaller vessels and eventually into vessels of microscopic caliber called capillaries. Each ventricle is equipped with two valves. One of these prevents backflow of blood into the atrium when the ventricle contracts, and the other prevents backflow of expelled blood into the ventricle while it is relaxed and refilling for the next contraction. Contraction of a chamber is called systole, and relaxation is called diastole. Systole occurs when a wave of electrical activity, beginning at the pacemaker (sinoatrial node) in the right atrium, spreads over the heart muscle, stimulating first by John H. Dirckx, M.D. the atria and then the ventricles to contract. During the fraction of a second that elapses before the next impulse from the pacemaker, the heart muscle relaxes in diastole and refilling of the chambers occurs. Venous blood, low in oxygen and high in carbon dioxide, is collected by the superior and inferior venae cavae and delivered to the right atrium and hence to the right ventricle. Right ventricular systole sends this blood through the pulmonary artery to the lungs, in whose capillaries the blood picks up fresh oxygen from inspired air and discharges excess carbon dioxide into air that is about to be expired. During systole the tricuspid valve prevents blood from leaking back into the right atrium, and during the succeeding diastole the pulmonic valve keeps blood from leaking back into the right ventricle. Oxygenated and purified blood is returned to the heart by the pulmonary veins, which deliver it to the left atrium. Passing from the left atrium to the left ventricle, the blood is now pumped through the aorta into the arteries of the systemic circulation. During left ventricular systole, the mitral valve prevents blood from being driven back into the left atrium; during diastole, the aortic valve prevents blood from leaking back into the ventricle. The arteries branch into increasingly smaller vessels and eventually break up into capillaries in the tissues, where oxygen is released and carbon dioxide and other wastes are taken up. The blood then passes through peripheral veins back to the venae cavae and the circuit is complete. Hypertension Hypertension means abnormal elevation of the blood pressure; specifically, a transitory or persistent elevation of the pressure of the blood in the arteries of the systemic circulation to a level that can induce cardiovascular damage. (Pulmonary hypertension, affecting the pulmonary arteries, which carry blood to the lungs from the right ventricle, is a separate disorder usually related to disease of the lungs, pulmonary vasculature, or mitral valve.) Hypertension is a major cause of cardiovascular disease and premature death in Western (industrialized) societies. The annual toll of deaths due directly to hypertension in the United States is about 35,000, and it is recognized as a contributing factor in another 180,000 deaths. Persons with hypertension have a 3-fold increase in the risk of heart attack and a 7- to 10-fold increase in the risk of stroke. One fourth of the population of the U.S. (and one half of persons over age 60) have John H. Dirckx, M.D., The Cardiovascular System: Anatomy, Physiology, Pathology The SUM Program Cardiology Transcription Unit, 2nd ed. ©2011, Health Professions Institute, www.hpisum.com The annual toll of deaths due directly to hypertension in the United States is about 35,000, and it is recognized as a contributing factor in another 180,000 deaths. significant elevation of blood pressure, but only about one third of persons so affected are aware of the condition and are receiving treatment. The prevalence of hypertension and the risk of complications are considerably higher in African Americans. Hypertension is defined arbitrarily as systolic blood pressure above 140 mmHg or diastolic blood pressure above 90 mmHg. The systolic pressure is the highest pressure reached by the blood in the large arteries with each beat of the heart, while the diastolic pressure is the lowest level to which the pressure drops between beats of the heart. The aorta and its branches and sub-branches—the named arteries of the body— are not rigid pipes, but are normally highly elastic structures. This helps to keep the blood flowing at a smoother rate instead of allowing it to be propelled through the arteries in a series of jerks. To put it another way, the elasticity of the arteries minimizes the difference (called the pulse pressure) between systolic and diastolic pressures. As each contraction of the left ventricle propels blood into the arterial system, the vessels expand to accommodate the sudden increased load of blood. (This rhythmic bulging accounts for the “pulse,” synchronous with the heartbeat, that can be felt in peripheral arteries.) Then, during diastole, as the left ventricle relaxes and refills, the stretched arterial walls rebound, keeping the blood moving forward through the circulation until the next systole occurs. In this way the aorta and larger arteries act as a sort of auxiliary heart, briefly storing some of the kinetic energy of each ventricular contraction and then releasing it while the ventricle is filling in preparation for its next contraction. The pressure of the blood depends on an interplay of many factors, but two of these are of primary importance: the rate and force of ventricular contractions and the resistance of the arteries against which the heart has to work in order to maintain adequate flow in tissue capillaries. Arterial resistance depends on the net cross-sectional area of the large and medium-sized arteries, and this net area varies with the tone or state of contraction of the muscular layers of these arteries. The maintenance of normal blood pressure depends on a complex interaction, not yet fully understood, of neural and hormonal control mechanisms. Hypertension results when these control mechanisms become dysregulated in any of various ways. The adrenergic system is concerned with maintaining normal blood flow to vital structures from minute to minute by meeting acute, short-term needs. Challenges as variable as standing up from a recumbent or sitting position, dehydration due to vomiting and diarrhea, and severe hemorrhage can all pose acute threats to the adequacy of blood flow to the brain and heart. When blood pressure sensors (baroreceptors) in large arteries detect a drop in pressure, sympathetic nerve fibers to the heart automatically increase the rate and force of cardiac contractions. Meanwhile, sympathomimetic hormones (epinephrine, norepinephrine, dopamine, serotonin) are released from the suprarenal glands and other glandlike structures to boost and regulate blood flow, not only by stimulating the heart but also by acting on the muscular layers of arteries, dilating those that supply vital organs while constricting or shutting down those to less critical areas such as the skin and the digestive system. A neoplasm that produces serotonin (carcinoid tumor) or epinephrine-like substances (pheochromocytoma) can cause intermittent or sustained elevation of blood pressure, but these are relatively rare causes of hypertension. The renin-angiotensin-aldosterone system provides longer-term regulation of blood pressure by offsetting less acute variations in blood flow to vital tissues. The action of this system involves a complex interaction of hormones and enzymes produced at widely differing sites. Angiotensinogen, a globulin formed in the liver, is normally present in blood and tissues but performs no physiologic function. That is, it is a precursor substance that must be chemically converted before it becomes active. The first step of this conversion takes place under the influence of renin, an enzyme produced in the kidney. The release of renin can be triggered in various ways: by a drop in systemic blood pressure, as detected by baroreceptors; by a decline in the amount of urine being processed by the renal tubules (an indirect indication of diminished renal blood flow); or even by a change in the sodium chloride concentration of renal tubular fluid. Under the action of renin, angiotensinogen is converted to angiotensin I. This substance, too, is just an intermediary metabolite. Only when angiotensin I is converted to angiotensin II does the system begin to have an impact on blood pressure and electrolyte balance. This conversion is triggered by angiotensin-converting enzyme (ACE), a glycoprotein produced in various tissues, principally the lung. Angiotensin II is a powerful and wide-ranging agent, which raises systemic blood pressure by acting directly on the peripheral circulation as a vasoconstrictor, and which also stimulates the cortices of the suprarenal glands to secrete aldosterone, a hormone that promotes retention of sodium. Angiotension II has other functions, such as promotion of cell proliferation and migration, that do not concern us here. Early in the twentieth century it was discovered that obstruction of a renal artery by disease (or ligation of a renal artery in an experimental animal) can induce hypertension. We now know that this abnormal elevation of blood pressure results from an overproduction of renin by the diseased kidney, which responds to local ischemia in the same way that it would respond to a sustained reduction in systemic blood pressure. An occasional case of hypertension is found to be due to a lesion in a renal artery. That is the reason why physicians listen with a stethoscope over the flanks for a bruit that might John H. Dirckx, M.D., The Cardiovascular System: Anatomy, Physiology, Pathology The SUM Program Cardiology Transcription Unit, 2nd ed. ©2011, Health Professions Institute, www.hpisum.com indicate stenosis (narrowing) of a renal artery, particularly when assessing a patient with hypertension. When chronic elevation of blood pressure is traced to renal ischemia or a hormone-producing tumor, the condition may be reversible by surgery. But such cases of secondary hypertension make up fewer than 10% of the total; the rest are termed essential hypertension. Essential hypertension is currently believed to result from a complex derangement, genetically induced, in the renin-angiotensin-aldosterone system. Persons with essential hypertension have elevated peripheral vascular resistance and they retain excessive sodium. Moreover, drugs that reduce peripheral resistance and enhance the renal excretion of sodium are useful in correcting essential hypertension. Drugs that block the action of angiotensin-converting enzyme (ACE inhibitors) or of angiotensin II (angiotensin II receptor inhibitors) work even better. It has been recognized for about one hundred years that uncontrolled chronic hypertension is associated with disease of both the heart and the arteries of the systemic circulation. Sustained elevation of systolic pressure overworks the heart and can lead to ventricular dilatation (stretching of the ventricular wall due to chronic overfilling), hypertrophy (compensatory overgrowth of ventricular muscle), or cardiac failure (discussed below). In addition, chronic hypertension leads to loss of tone and elasticity in arteries, and can aggravate arterial changes due to aging or atherosclerosis (also discussed below). Among the arteries that may be so affected are those of the retina. This is significant partly because uncontrolled hypertension can lead to visual impairment. But of broader importance is the fact that the retinal vessels can easily be examined with an ophthalmoscope, unless the patient has severe cataracts. Examination of the ocular fundi or “eye grounds” is part of the routine physical examination of an adult, and can yield important information about general vascular health as well as the presence and severity of hypertension. The four KeithWagener-Barker stages of hypertensive retinopathy are: Grade 1—Focal or diffuse narrowing of arteriolar caliber due to spasm. Grade 2—Arteriolar diameter less than 50% of that of corresponding venules; “silver wire,” “copper wire,” or “pipestem” appearance of arterioles, indicating structural changes in vessel walls. Grade 3—In addition to the above changes, retinal hemorrhages or exudates. (As used in this context, exudate is something of a misnomer. A retinal exudate is a whitish spot of variable size, shape, and composition—usually a deposit of lipid material at a site of old hemorrhage or infarction.) Grade 4—In addition to the above, papilledema (swelling of the optic nerve head). While the effects of hypertension on retinal vessels provide valuable diagnostic information, the impact of the disease on arteries supplying vital structures is of far greater importance. The adverse effects of chronic hypertension on the cardiovascular system are complex and cumulative. For example, Hypertension is defined arbitrarily as systolic blood pressure above 140 mmHg or diastolic blood pressure above 90 mmHg. damage to renal vasculature caused by hypertension can augment the overproduction of renin, leading to more severe hypertension and accelerated progression of disease. Known risk factors for essential hypertension include a family history of hypertension, African American ethnicity, age over 60, the postmenopausal state, overweight, a sedentary lifestyle, excessive intake of dietary sodium, excessive use of alcohol, and chronic emotional stress. It is currently recognized that, for many persons with essential hypertension, blood pressure elevation is just one feature of a complex disorder called the metabolic syndrome (discussed below). This syndrome, induced by an interplay of genetic and environmental factors, includes obesity, abnormal glucose and lipid metabolism, insulin resistance, diminished arterial compliance, accelerated atherogenesis, and renal disease. Although extremely high diastolic pressure can sometimes be associated with headache, dizziness, or even seizures and coma, uncomplicated hypertension seldom causes any symptoms at all. For that reason, the diagnosis is usually made incidentally, during screening of seemingly healthy persons or those who are being examined or treated for some other condition. Statistics show that the early detection and aggressive treatment of hypertension can reduce morbidity and mortality associated with this condition. For example, control of hypertension reduces the risk of stroke by 30-50%. Modern standards of medical practice require vigorous efforts to identify hypertension, particularly in persons at high risk, and early and aggressive treatment of the condition when it is found. Current treatment protocols favor a stepped approach: first lifestyle changes (weight loss if appropriate, regular aerobic exercise, restriction of sodium and alcohol intake, and reduction of emotional stress when possible), then drugs gradually increasing in potency (and price tag and potential side effects). Drugs used to treat hypertension include diuretics that promote renal excretion of sodium; beta-adrenergic and calcium channel blockers, which blunt the effects of sympathetic nerve stimuli and of circulating adrenergic agents on heart action and vascular tone; angiotensin-converting enzyme (ACE) inhibitors and angiotensin II receptor antagonists; alpha-1 adrenergic antagonists; centrally acting alpha-agonists; and others. Atherosclerosis As early as the nineteenth century, pathologists recognized that the arteries of older persons often lose their elasticity and become narrowed in caliber. They also observed that these degenerative changes, which they termed arteriosclerosis (literally ‘hardening of the arteries’), are often associated with ischemia of the tissues supplied, and are thus the underlying John H. Dirckx, M.D., The Cardiovascular System: Anatomy, Physiology, Pathology The SUM Program Cardiology Transcription Unit, 2nd ed. ©2011, Health Professions Institute, www.hpisum.com mechanism of many serious health problems, including myocardial ischemia (causing angina, cardiac failure, and myocardial infarction), cerebrovascular disease (causing stroke and dementia), and peripheral vascular disease (causing intermittent claudication and gangrene of extremities). During the twentieth century, advances in microscopy and biochemistry led to the discovery that most cases of arteriosclerosis are due to deposits of lipid material (cholesterol) in the walls of the arteries affected. This commonest type of arteriosclerosis was termed atherosclerosis (from a Greek word meaning ‘gruel’, referring to the gritty, pasty consistency of the lipid deposits). Atherosclerosis (Figure 1) is characterized by the occurrence of irregularly distributed lipid deposits (atheromata or atheromas; singular, atheroma) in the innermost layer (tunica intima) of large and medium-sized arteries. With the passage of time these lesions become fibrous, like scar tissue, and may even calcify; hence the progressive loss of elasticity. Atheromatous deposits tend to grow slowly and intermittently, but in time they can cause significant reduction in the caliber of affected arteries, with impairment of blood flow and clinical consequences that depend on the tissues supplied. Early theories of the causation of atherosclerosis viewed it as a degenerative process and traced it to an elevation of circulating cholesterol, which was assumed to result from excessive dietary intake of cholesterol. We now realize that inflammation plays a more important role than degeneration Figure 1 Atherosclerosis Source: National Heart Lung and Blood Institute, National Institutes of Health. Accessed from Wikipedia Commons. in the atherosclerotic process, and that elevation of the cholesterol level usually results from an inborn metabolic flaw rather than from consumption of too much cholesterol in the diet. Cholesterol is a complex lipid (fatty) molecule that serves as a building block for many important substances, including the steroid hormones (cortisol and the sex hormones), bile salts, and certain constituents of cell membranes. Some cholesterol is found in every cell in the body. But even though it is an essential component of all tissues, it is not considered a nutrient, because it is continually being synthesized from simpler substances by the liver and other tissues. Cholesterol is found in virtually all foods from animal sources—meats, poultry, fish, eggs, milk, and dairy products. It is especially abundant in fatty meats, whole milk, and egg yolk. Although a high intake of cholesterol-containing foods can raise the serum cholesterol to unhealthful levels, dietary cholesterol is probably not of major importance for most persons in the genesis of atherosclerosis. Moreover, dietary restrictions are only slightly helpful in reducing an abnormally high cholesterol level. Of far greater importance in the development of hypercholesterolemia and its treatment is the role of inherited imbalances in the proportion of low- and highdensity lipoproteins. As noted above, current theories regard atherosclerosis chiefly as an inflammatory rather than a degenerative process. Atheromata are more likely to develop at areas of turbulent flow within an artery, such as at a bifurcation. The earliest stage in the process that can be recognized on histopathologic study is the appearance, in the lining (tunica intima) of an artery, of so-called foam cells. These are macrophages (tissue cells that phagocytize dead cells and other debris) that look foamy because they are stuffed with cholesterol. The presence of this material in a place where it doesn’t belong elicits local inflammation, mediated by various tissue factors, including interleukins, cell adhesion molecules, and platelet factors. Circulating monocytes and lymphocytes stick to and penetrate the lining of the artery at the site of the cholesterol deposit. Smooth muscle cells in the underlying muscular coat (tunica media) of the artery proliferate to form a plaque, which continues to enlarge as more cholesterol is deposited. Fibrosis, a scar-like formation of connective tissue fibers within the plaque, eventually occurs, and as a final stage the plaque may calcify. The expansion of an atheromatous plaque leads to stenosis (reduction in caliber) of the artery, which can culminate in occlusion (complete obstruction to blood flow), with ischemia (impairment of blood supply) or infarction (irreversible damage) of tissues supplied by it. Besides blocking blood flow, a plaque can break down and ulcerate, releasing fragments (emboli) into the circulation, which can cause obstruction of a smaller arterial branch distally. An atheromatous plaque can also become the site of thrombosis (local formation of a blood clot), and besides further reducing vascular caliber this too can result in embolization of distal vessels. In addition, inflammatory and degenerative changes in and around the plaque can lead to local John H. Dirckx, M.D., The Cardiovascular System: Anatomy, Physiology, Pathology The SUM Program Cardiology Transcription Unit, 2nd ed. ©2011, Health Professions Institute, www.hpisum.com hemorrhage or dissection (separation or splitting of layers of the arterial wall as blood, under normal or elevated pressure, forces it way through damaged tissue). The diagnosis of atherosclerosis is based on history and physical examination, augmented by angiography, Doppler ultrasonography, and other imaging studies. Treatment is largely mechanical: balloon stretching, laser ablation, or surgical removal of plaques, and various bypass and grafting procedures. More specific information on the diagnosis and treatment of coronary atherosclerosis will be presented later. Well-established risk factors for atherosclerosis are male sex, advancing age, the postmenopausal state, a family history of atherosclerosis, cigarette smoking, elevation of plasma total cholesterol and low-density lipoprotein (LDL) cholesterol, hypertension, diabetes mellitus, overweight, and a sedentary lifestyle. Other risk factors detectable by biochemical testing include elevation of plasma triglycerides, fasting insulin, fibrinogen, C-reactive protein, amyloid A, interleukin-6, apolipoproteins A and B, lipoprotein (a), and homocysteine. The prevention of atherosclerosis is a high-priority objective for modern medicine. Measures of proven value include regular vigorous (anerobic) exercise, a diet low in fat and cholesterol, maintenance of a healthful weight, and avoidance of tobacco. Drug therapy is indicated for diabetes mellitus and hypercholesterolemia. Myocardial Infarction Myocardial infarction (MI), also known as coronary thrombosis and heart attack, is defined as death (irreversible damage) of a segment of heart muscle (myocardium) caused by obstruction to blood flow in one or more branches of the coronary system. Myocardial infarction is currently recognized as the most common cause of death in this country. About 800,000 persons annually sustain first heart attacks, with a mortality rate of 30%, and 450,000 persons sustain recurrent heart attacks, with a mortality rate of 50%. The usual cause of MI is formation of a thrombus in a coronary artery (Figure 2) at the site of an atherosclerotic plaque. Less frequent causes are anatomic anomalies or inflammatory disease (vasculitis) involving the coronary arteries and arterial spasm induced by drugs, particularly cocaine. At least 80% of persons sustaining myocardial infarction have no prior history of angina pectoris, and in 20% the diagnosis is missed because symptoms are either absent (“silent infarction”) or are blamed on something else. Some 20% of persons sustaining MI die before reaching a hospital. Nowadays everyone who has completed training in adult CPR knows the symptoms and signs of a heart attack. It may therefore seem surprising that the very first patient in whom myocardial infarction was diagnosed before death was reported as recently as 1912 by the American physician James B. Herrick. The classical symptoms of myocardial infarction are crushing anterior chest pain radiating into the neck, shoulder, or arm, lasting more than 30 minutes, and not relieved by nitroglycerin. The classical symptoms of myocardial infarction are crushing anterior chest pain radiating into the neck, shoulder, or arm, lasting more than 30 minutes, and not relieved by nitroglycerin. Recent studies have identified important gender differences in the collateral symptoms of MI. Although chest pain is the most common symptom reported by both men and women, diaphoresis is more likely to occur in men, while women are more likely to complain of neck, jaw, or back pain, nausea, vomiting, and dyspnea. Clear-cut evidence of acute infarction may not be obtainable during the first 6 hours in as many as one half of patients; hence the need for close observation even in cases where the diagnosis seems doubtful. Physical examination is often unremarkable but may detect soft heart sounds, an atrial gallop rhythm (4th heart sound), or a pericardial friction rub. Classical electrocardiographic signs are ST segment elevation (later changing to depression) and T wave inversion in leads recording electrical activity in the infarcted segment of myocardium. Deep Q waves indicate transmural (“all the way through the muscular wall”) damage and a graver prognosis. Diagnosis may be confirmed by elevation in serum levels of myoglobin, lactic dehydrogenase, the MB isoenzyme of creatine kinase, and troponins. Figure 2 Coronary Artery Source: National Heart Lung and Blood Institute, National Insti tutes of Health. Accessed from Wikipedia Commons. John H. Dirckx, M.D., The Cardiovascular System: Anatomy, Physiology, Pathology The SUM Program Cardiology Transcription Unit, 2nd ed. ©2011, Health Professions Institute, www.hpisum.com The full expression congestive heart failure refers to the elevation of central venous pressure that typically accompanies . . . reduction in pumping efficiency. Acute myocardial infarction can cause death by a variety of mechanisms: cardiac arrest, ventricular fibrillation (ineffectual twitching of damaged heart muscle instead of normal contractions), cardiogenic shock (inability of the heart to maintain adequate blood flow for vital functions), congestive heart failure (discussed below), rupture of a papillary muscle with resulting malfunction of the aortic or pulmonic valve, or even rupture of a ventricle (cardiorrhexis). The standard treatment of myocardial infarction includes admission to a coronary care unit with continuous cardiac monitoring and the administration of a narcotic analgesic for pain, oxygen by inhalation to boost myocardial oxygenation, a beta-blocker, an ACE inhibitor, an anticoagulant (aspirin orally and heparin by injection), and a thrombolytic agent. During the past decade, thrombolytic therapy (the intravenous administration of an agent intended to restore circulation by dissolving a thrombus in an artery) has reduced the mortality of acute myocardial infarction by 20-40%. Under favorable circumstances, about 50% of patients with acute MI will have patent coronary arteries 90 minutes after treatment. Best results are achieved when the agent is given within 100 minutes after the onset of symptoms. Thrombolytic agents break down the fibrin in a clot by activating plasminogen, a naturally occurring substance involved in clotting mechanisms. Agents most often used to treat MI are tissue plasminogen activator (TPA), which is synthesized by recombinant DNA, and streptokinase, an enzyme produced by streptococci. Although streptokinase is sometimes chosen instead of TPA because it is less expensive, TPA is more effective. Hemorrhage is a major risk with thrombolytic therapy. Contraindications include active or recent bleeding of any cause, recent surgery, prolonged or traumatic cardiopulmonary resuscitation, and pregnancy. When evidence of acute myocardial ischemia persists despite medical therapy, angiography may be done to confirm and localize coronary occlusion. Emergency PTCA performed within two hours after the onset of pain in acute myocardial infarction yields a lower mortality rate than thrombolytic therapy and lower rates of nonfatal reinfarction and hemorrhagic stroke. Congestive Heart Failure Congestive heart failure is an extremely common complication of a broad range of disorders, not all of them primarily affecting the heart. In this country alone, congestive heart failure is the reason for about one million hospital admissions annually, and ranks number one among discharge diagnoses for hospitalized patients over 65. In persons over 80, the prevalence of chronic heart failure is about 10%. The term heart failure (Figure 3) has a more restricted meaning than lay persons sometimes suppose; it certainly is not synonymous with cardiac arrest. But although physicians define heart failure as “an acute or chronic impairment of the ability of the heart to function efficiently as a pump,” it is becoming increasingly evident that this disorder is far more complex than if the failing heart were simply a piece of wornout machinery. Cardiologists now recognize that heart failure is a spectrum of clinical states having in common a reduction in the pumping efficiency of the heart but varying widely in symptoms, signs, and impact on normal function. The full expression congestive heart failure refers to the elevation of central venous pressure that typically accompanies this reduction in pumping efficiency. The many conditions that can culminate in congestive heart failure can be divided into two large classes: those that directly impair the contractile force of the heart, and those that Figure 3 Heart Failure Source: Wikipedia Commons. John H. Dirckx, M.D., The Cardiovascular System: Anatomy, Physiology, Pathology The SUM Program Cardiology Transcription Unit, 2nd ed. ©2011, Health Professions Institute, www.hpisum.com place an excessive burden on the heart. Both types can occur together in the same person. Among disorders that curtail the pumping power of heart muscle, coronary artery disease is by far the most common, but intrinsic disease of the myocardium due to infection, autoimmune disease, or deficiency states can also result in primary pump failure. Disorders that can induce failure by overworking a normal heart include hypertension, congenital or acquired disease of a heart valve, arteriovenous fistula (an abnormal communication somewhere in the circulation through which arterial blood is shunted directly into the venous circulation), severe anemia, and hyperthyroidism. In cardiac failure resulting from coronary artery disease and hypertension, cardiac output (that is, the amount of blood pumped into the aorta with each contraction of the left ventricle) is reduced; hence the resulting disturbance in cardiovascular dynamics is referred to as low-output failure. In contrast, cardiac output may be normal or increased in failure due to anemia, arteriovenous fistula, or thyrotoxicosis, hence the term high-output failure. Cardiac output can be assessed or measured in various ways. The stroke volume is the volume of blood expelled from the ventricle during systole; the ejection fraction (expressed as a percent) is that proportion of the blood in the ventricle at the end of diastole that is actually expelled during systole. The pulse pressure (which, as mentioned earlier, is the difference between systolic and diastolic blood pressures) is typically reduced in low-output failure and increased in high-output failure. Certain conditions (pulmonary hypertension, mitral stenosis, tricuspid regurgitation) are associated with primarily right ventricular failure. But most discussions of cardiac failure, including this one, emphasize the left ventricle, because impairment of pumping efficiency in the left side of the heart has more profound and serious effects on cardiovascular dynamics. It is nonetheless true that coronary artery disease, the commonest cause of congestive failure, can affect either ventricle separately, or both of them in varying degrees. Moreover, because the right and left ventricles operate in tandem and form parts of a single circuit, severe failure of one will eventually diminish the efficiency of the other. Fifty years ago, theories of the pathophysiology of heart failure made a sharp distinction between “forward” and “backward” failure. Forward failure denotes the inability of the left ventricle to pump enough blood to meet the needs of tissues; backward failure refers to the buildup of pressure in the ventricle that results from its inability to distend adequately during diastolic filling. This rise of pressure in the left ventricle, extending “backward” to raise the pressure within the pulmonary venous circulation, is responsible for the dyspnea and reduction in exercise tolerance that are among the most conspicuous features of heart failure. Similarly, backward failure of the right ventricle raises the pressure in the peripheral venous system, causing venous distention and edema of the viscera and extremities. Hence it is this backward component of the process that results in the congestive aspect of heart failure. Even with aggressive treatment, the fiveyear survival rate for persons with congestive heart failure is only 50%. Death most commonly results from progressive ventricular dysfunction, arrhythmia, or thromboembolism. In modern cardiology, the distinction between forward and backward failure is viewed as a purely conceptual one. The fully developed syndrome of heart failure includes both of these elements as coordinate and interactive aspects of the same basic phenomenon. Similarly, the validity of older distinctions between right and left heart failure and between systolic and diastolic heart failure have been called into question. A syndrome of isolated or predominantly diastolic failure does, however, occur in some persons. In this disorder, affecting particularly elderly patients with hypertension and atherosclerosis, the ejection fraction may be normal, but left atrial and pulmonary venous pressures are elevated because diastolic filling of the left ventricle is impaired. Whereas older concepts of congestive heart failure tended to view the failing heart as a faltering or deteriorating mechanism in isolation from other bodily systems, we now know that neural and hormonal factors play a crucial role in the development of the syndrome. The drop in systemic blood flow that occurs with low-output failure triggers sympathetic responses (increase in heart rate and myocardial contractility, peripheral vasoconstriction) that only add to the burden of the failing heart. The renin-angiotensin-aldosterone system, discussed earlier in connection with hypertension, also plays an important role in the pathophysiology of congestive heart failure. Reduction in renal blood flow leads to activation of this system, with resultant further peripheral vasoconstriction and retention of sodium and water. Symptoms typical of left ventricular failure are dyspnea, cough, and reduced exercise tolerance. Shortness of breath may occur at rest or only with exertion. Two types of dyspnea are especially characteristic of left heart failure, though they can also occur in other conditions. Orthopnea is shortness of breath in the recumbent position, relieved by sitting up; paroxysmal nocturnal dyspnea (PND) is an attack of shortness of breath that awakens the patient from sleep during the night. These symptoms result from the rise of back-pressure in the pulmonary venous system, which causes pulmonary congestion (vascular engorgement) and interstitial edema (excess fluid in lung tissues). Severe left ventricular failure can cause acute pulmonary edema, with transudation of watery fluid into pulmonary air sacs. This condition, manifested by severe dyspnea and production of copious frothy sputum, is a medical emergency. John H. Dirckx, M.D., The Cardiovascular System: Anatomy, Physiology, Pathology The SUM Program Cardiology Transcription Unit, 2nd ed. ©2011, Health Professions Institute, www.hpisum.com Limitation of dietary sodium to 2-3 g/day and administration of diuretics, ACE inhibitors, and beta-blocking agents are useful in correcting sodium retention and circulatory overload. The symptoms of right ventricular failure result from elevation of pressure in systemic veins: swelling of the lower limbs (dependent edema) and effusion of fluid into the peritoneal cavity (ascites). Squeezing a severely swollen limb with the fingers may leave impressions that only slowly refill; this is called pitting edema. When peripheral edema involves the trunk and upper limbs as well as the lower limbs, the term anasarca is used. Brawny (“tough”) edema is chronic swelling in which deposition of connective tissue fibers in edema fluid has caused induration. Physical findings in the patient with congestive heart failure depend on the severity and duration of failure as well as its underlying cause and the presence of concomitant disorders. Examination of the heart generally reveals tachycardia, cardiac dilatation, a weak first heart sound, and a prominent fourth heart sound (protodiastolic gallop). The latter two findings reflect a faltering in the contractile force and pumping efficiency of the ventricles. On auscultation of breath sounds, the examiner hears crepitant rales (crackling sounds like those made by crumpling a piece of cellophane) caused by bubbling of air through free edema fluid in small air passages. Systemic venous engorgement may be manifested by distention of the jugular veins, enlargement of the liver (hepatomegaly), and a fluid wave on palpation of the abdomen due to ascites. Hepatojugular reflux is a visible wave of increased engorgement in the jugular veins after manual compression of the swollen liver. The chest x-ray of a patient with congestive heart failure shows cardiac dilatation and often Kerley B lines (short radiopaque streaks indicating edema in interalveolar septa). Pleural effusion (free edema fluid in the pleural space) may cause blunting of the costophrenic sulci (the sharp angles formed by the chest wall and the peripheral rim of the diaphragm). In the presence of significant systolic dysfunction, an echocardiogram shows an ejection fraction of 40% or less. A system endorsed by the American College of Cardiology and the American Heart Association divides the evolution of heart failure into four stages designated with Roman letters: A The subject is at high risk of heart failure because of an underlying condition such as hypertension or coronary atherosclerosis, but has no symptoms or signs of structural heart disease. B Structural heart disease is present, but without symptoms of heart failure. C Structural heart disease is present, along with past or present symptoms of heart failure. D Refractory heart failure requiring special interventions. The better-known New York Heart Association Classification distinguishes four levels of functional impairment in heart failure, designated with Roman numerals: I II III IV Asymptomatic. Symptomatic with moderate exertion. Symptomatic with minimal exertion. Symptomatic at rest. The treatment of chronic congestive heart failure begins with whatever measures are available to control underlying factors such as hypertension and coronary artery disease. Limitation of dietary sodium to 2-3 g/day and administration of diuretics, ACE inhibitors, and beta-blocking agents are useful in correcting sodium retention and circulatory overload. Digoxin is a derivative of digitalis (foxglove), an herbal remedy which for many decades was the mainstay of treatment in congestive failure. Digoxin exerts an inotropic effect (that is, it directly enhances the contractility of heart muscle) and also stimulates the vagus nerves, thus slowing the pulse and counteracting inappropriate sympathetic stimulation. Acute pulmonary edema is treated with morphine, an intravenous diuretic, sublingual and intravenous nitroglycerin, and nitroprusside. Acute cardiac failure that is refractory to these agents sometimes responds to inotropic drugs such as dobutamine and dopamine. Even with aggressive treatment, the five-year survival rate for persons with congestive heart failure is only 50%. Death most commonly results from progressive ventricular dysfunction, arrhythmia, or thromboembolism. John H. Dirckx, M.D., The Cardiovascular System: Anatomy, Physiology, Pathology The SUM Program Cardiology Transcription Unit, 2nd ed. ©2011, Health Professions Institute, www.hpisum.com