Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
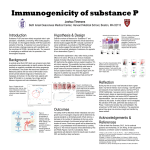
Jpn J cu« OncoI1998;28(11)673-678 Clinicopathological Factors Predicting Retroperitoneal Lymph Node Metastasis and Survival in Endometrial Cancer Xiaohai Tang 1,*, Kenjiro Tanemura', Weimin Ye2, Kazuo Ohml', Ryuichiro Tsunematsu', Takuro Yamada 1, Noriyuki Katsumatal and Takahiko Sonoda 1 of Gynecology, 2Cancer Information and Epidemiology Division and 3Division of Medical Oncology, National Cancer Center, Tokyo, Japan 1Division Background: By clarifying the significance of clinicopathological factors for retroperitoneal lymph node metastasis and survival of patients with endometrial cancer, we suggest ideas for optimal treatment of this disease. Methods: A retrospective study was conducted in 310 women with endometrial cancer who underwent surgery with retroperitoneal lymphadenectomy. To evaluate retroperitoneal lymph node metastasis, age-adjusted and multivariable analyses were carried out for six clinicopathological factors including pathological grade, myometrial invasion, cervical invasion, peritoneal cytology, lymphatic permeation and vascular invasion. To evaluate survival, besides the above factors, a positive rate of metastasis of dissected retroperitoneal lymph nodes was included. Results: In 40 patients (13%) with nodal metastasis, the average positive rate of metastasis of dissected retroperitoneal lymph nodes was 22%. For retroperitoneal lymph node metastasis, the odds ratio of deep myometrial invasion, cervical invasion and severe lymphatic permeation were 5.97, 2.72 and 12.01, respectively. For survival, the hazard ratios of the positive rates of metastasis of dissected retroperitoneal lymph nodes (both 25% and <25%), positive peritoneal cytology and poor pathological grade were 7.10, 3.24, 3.82 and 3.27, respectively, and 5-year survival rates for them were 0, 50, 72 and 77%, respectively. Conclusions: For retroperitoneal lymph node metastasis, lymphatic permeation, deep myometrial invasion and cervical invasion were the independent prognostic factors. For survival, retroperitoneal lymph metastasis, poorpathological grades and positive peritoneal cytology were the independent prognostic factors. The positive rate of metastasis of dissected retroperitoneal lymph metastasis playsan important rolein predicting survival of endometrial cancer. Lymph node biopsy is insufficient in treatment of this disease. Key words: clinicopathological factors - lymph node metastasis - survival - endometrial cancer INTRODUCTION In 1988, the International Federation of Obstetrics and Gynecology (FIGO) introduced a new system for the clinicopathological staging of endometrial cancer. The staging system includes the assessment of pathological grade, myometrial invasion, cervical Received June 10, 1998; accepted August 14, 1998 *A Sasakawa Medical Fellow from the Department of Gynecological Oncology, Sichuan Cancer Hospital, No. 55, Sect. 4, Ren Min Nan Road, Chengdu, Sichuan 610041, China For reprints and all correspondence: Kenjiro Tanemura, Division of Gynecology, National Cancer Center Hospital, 1-1, Tsukiji 5-chome, Chuo-Ku, Tokyo 104, Japan Abbreviations: FIGO, International Federation of Obstetrics and Gynecology; RLN, retroperitoneal lymph node; P, P value; PAN, paraaortic lymph node; PLN, pelvic lymph node invasion, peritoneal cytology and retroperitoneal lymph node (RLN) metastasis. Since then, numerous reports have elucidated the prognostic significance of these factors (1-13). In addition, lymphatic permeation and vascular invasion were discussed for their prognostic significance in this disease (14,15). However, the discriminatory value of these is the subject of further investigation. Patients with cervical invasion have a higher incidence of RLN metastasis. In general, cervical invasion is frequently associated with deep myometrial invasion that is in tum strongly related to RLN metastasis. However, why patients with cervical invasion have a higher incidence of nodal metastasis needs further investigation (1-3,12). The number of metastatic nodes among the total dissected RLNs has always been individualized in each patient. To understand its significance for survival, we proposed the evaluation of positive rate of metastasis of the dissected RLNs. 674 Prognostic factors of endometrial cancer Table 1. Patients' characteristics Age yr Mean 55 Range 25-82 Stage IA-IC No. 195 IIA-IIB 48 IlIA-IlIC 67 Pathology Adenocarcinoma Adenosquamous H ysterectom y No. 294 16 No. Simple 227 Modified radical 10 Radical 73 Dissected RLN in each patient No. Mean 24 Range 10-62 RLN metastasis No. 40 Positive rate of metastasis of dissected RLNs from the study, as their biological properties were different. The number of dissected RLNs was counted. There was not a significant difference in the number of dissected RLNs between the patients with and those without RLN metastasis. The percentage of metastatic nodes in the total dissected lymph nodes was defined as a positive rate of metastasis of dissected RLNs. The living status of the patients was registered up to December 1996 for survival analysis. Distribution of age, FIGO stage, pathology, type of hysterectomy, number of dissected lymph nodes in each patient, number of patients with RLN metastasis and positive rate of metastasis of dissected RLNs are given in Table 1. % Mean 22 Median 10 RLN, retroperitoneallymph node. As RLN metastasis is associated with a poor prognosis (1,2,8-17), routine RLN dissection has been suggested for patients with endometrial cancer. However, the extent of lymphadenectomy remains controversial because the significance of lymphatic metastasis is yet to be defined (l,8). In addition, the significance of retroperitoneal lymph node biopsy also needs further investigation. The aims of this retrospective study were to analyze the relationship between RLN metastasis and the clinicopathological factors, to select independent clinicopathological prognostic factors of RLN metastasis and to clarify the significance of these factors for survival. PATIENTS AND METHODS Between January 1979 and December 1996, 310 women with primary endometrial cancer were treated with hysterectomy and lymphadenectomy of RLN at the Division of Gynecology of the National Cancer Center Hospital, Japan. All patients were diagnosed to have FIGO stage IA to mc primary endometrioid adenocarcinoma and adenosquamous cancer during the mentioned period. Patients with high-risk endometrial cancers, such as papillary serous cancer and clear cell cancer, were excluded SURGICAL PROCEDURE During a period of nearly 20 years, five of the authors steadily performed all operations on the patients according to routine methods set up by them at the Division of Gynecology. Patients without cervical invasion underwent simple abdominal hysterectomy and bilateral oophorectomy. Patients who were at a relatively advanced stage of the disease and had no cervical invasion underwent modified radical hysterectomy. Patients who were identified as having cervical invasion by preoperative endocervical curettage underwent radical hysterectomy. Peritoneal cytology was obtained immediately on opening the peritoneal cavity. For the lymphadenectomy, the retroperitoneal space in the pelvis was entered after dividing the round ligaments. The vessels were outlined and the lymphatic tissue along the external and internal iliac veins and arteries was removed from inguinal ligament to the common iliac vessels. In the obturator fossae, the iliac vessels and the obturator nerves were cleaned of the lymphatic tissue down to the levator muscle. Lymphatic tissue overlying the lower segment of the aorta (from aortic bifurcation up to the level of inferior mesentery) was removed after pelvic lymphadenectomy. The visual lymph nodes were picked from the dissected lymphatic tissue and divided into anatomical groups (aortic nodes, common iliac nodes, external iliac nodes, internal iliac nodes, obturator nodes, medial inguinal nodes, lateral inguinal nodes and cardinal ligament nodes) before pathological examination. STATISTICAL ANALYSIS Age-adjusted logistic regression was used to analyze the significance of each of the clinicopathological factors on RLN metastasis and then multivariate logistic regression was carried out to determine which of these were the independent prognostic factors. The Cox regression model was employed in analyzing the significance of each of the clinicopathological factors on survival and in determining which of these were the independent prognostic factors. Spearman analysis was used in correlation studies of the clinicopathological factors. Survival rates were calculated by the Kaplan-Meier method and differences in survival rates were examined using the log-rank test. Jpn J Clin OncoI1998;28(ll) 675 Table 2. Relation between RLN metastasis and clinicopathological factors Patients (11 = 319) OR* RLN metastasis Cases 95%CI ORt 95%CI % Pathological grade Gl 143 8 6 G2+G3 167 32 19 191 4 2 >1/2-2/3 31 4 >2/3 88 Negative Positive 3.88 1.79-9.36 1.42 0.50-4.29 13 6.88 1.55-30.68 4.27 0.87-20.70 32 36 26.34 9.90-91.46 5.97 1.84 -23.66 240 17 7 70 23 33 6.43 3.20-13.18 2.72 1.06-7.05 Negative 251 25 10 Positive 59 15 25 3.10 1.49-6.32 2.43 0.88-6.73 Myometrial invasion 0-1/2 Cervical invasion Peritoneal cytology Lymphatic permeation 181 4 2 A few + several 98 17 17 9.33 3.32-33.28 3.04 0.92-11.93 Many 31 19 61 70.70 22.42-278.87 12.01 2.72-59.90 Negative Vascular invasion Negative 248 17 7 53 26 49 5.68 2.59-12.49 1.88 0.67-5.24 9 7 78 47.47 10.54-335.96 2.43 0.33-23.72 A few + several Many OR, odds ratio; CI, confidence interval. *Age-adjusted odds ratios for factors other than age, estimated by logistic regression. t Age variable and other factors. RESULTS RELATIONSHIP BETWEEN RLN METASTASIS AND CLINICOPATHOLOGICAL FACTORS Table 2 shows the results of logistic analysis in the 310 patients. Patients who had any of the clinicopathological factors in its positive status or severer grade had a higher frequency of RLN metastasis compared with patients who had any of these factors in its negative status or milder grade. As age was related to RLN metastasis, it was adjusted in the following analysis. In age-adjusted analysis, any of the clinicopathological factors in its positive status or severer grade had a higher odds ratio compared with any of these factors in its negative status or milder grade. In multivariate analysis, severe lymphatic permeation (many lymphatic capillaries filled with cancer cells on microscopy), deep myometrial invasion and cervical invasion were found to be independent clinicopathological prognostic factors for RLN metastasis. Vascular invasion was related to a high frequency of RLN metastasis. However, it was not an independent clinicopathological prognostic factor for RLN metastasis. To investigate the reason, Spearman analyses were performed for correlation. A strong correlation was found between the lymphatic permeation and vascular invasion in which the correlation coefficient was 0.53 (P = 0.0001). The rest of the factors, including pathological grade and peritoneal cytology, were not significantly related to the RLN metastasis. RELATIONSHIP BETWEEN SURVIVAL AND CLINICOPATHOLOGICAL FACTORS The results of Cox regression analysis are given in Table 3. In the age-adjusted analysis, all the clinicopathological factors except cervical invasion were found to be related to survival. To determine the independent prognostic factors for survival, multivariate analysis was performed. RLN metastasis was identified as being the most significant prognostic factor for survival. In addition, pathological grade and peritoneal cytology were also identified as being independent prognostic factors for survival. However, myometrial invasion, cervical invasion, lymphatic permeation and vessel invasion were not significantly related to survival. 676 Prognostic factors of endometrial cancer Table 3. Relation between survival and clinicopathological factors Patients = 310) HR* 95%CI HRt 95% CI 1.87-7.62 3.27 1.49-7.22 (11 Pathological grade G1 143 1 G2+G3 167 3.78 191 1 Myometrial invasion 0-1/2 >1/2-2/3 31 1.80 2.26--7.73 1.27 0.43-3.71 >2/3 88 4.18 2.26--7.73 1.56 0.67-3.73 1.75 0.96--3.19 0.62 0.29-1.34 1.68-5.44 3.82 1.92-7.62 Cervical invasion Negative 240 Positive 70 Peritoneal cytology Negative 251 Positive 59 1 3.02 Lymphatic permeation Negative 181 1 A few + several 98 2.22 1.11-4.43 1.34 0.60-3.00 Many 31 8.51 4.11-17.62 1.75 0.55-5.05 Vessel invasion Negative A few + several 248 1 53 2.78 1.45-5.33 0.91 0.40-2.08 9 17.21 6.91-42.84 2.72 0.72-10.24 Many Lymph node metastasis Negative 270 1 <25% 33 6.71 3.58-12.55 3.24 1.41-7.41 ~25% 7 17.75 5.68-55.44 7.10 2.29-27.32 HR, hazard ratio; CI, confidence interval. *Age-adjusted hazard ratios. t Age and other factors in the table were adjusted. To study the influence of the positive rate of metastasis of dissected lymph nodes on survival, 40 patients (13%) with RLN metastasis were divided into two sub-groups. The dividing point was selected at a positive rate of 25%, according to the average positive rate of 22% of metastasis of dissected lymph nodes. The first sub-group had 33 patients with <25% of the positive rate of metastasis of dissected RLNs (the mean number of dissected nodes was 23). The second sub-group had seven patients with ~25% of the positive rate (the mean number of dissected nodes was 26). When compared with the sub-group of <25% of positive rate of nodal metastasis, the sub-group of ~25% of the positive rate had a significant high hazard ratio to survival (Table 3). In Kaplan-Meier analysis, all the independent prognostic factors for survival influenced significantly the survival probability of patients with endometrial cancer (Fig. I). Marked differences in survival probability were found during the early years of follow-up compared with the later years of follow-up. At the fifth year after surgery, all patients who had a ~25% positive rate of metastasis of dissected RLNs had died, compared with 55% of patients who had a <25% positive rate and 92% of patients who had no RLN metastasis who were alive. The five-year survival rates of the patients with negative RLN metastasis and positive RLN metastasis, negative peritoneal cytology and positive peritoneal cytology and well differentiated pathology and moderate to poor differentiated pathologies were 92 and 50% (P =0.001),90 and 72% (P =0.001) and 96 and 77% (P =0.001), respectively. The Kaplan-Meier plot did not show significant influences of the distribution and number of metastatic sites of the dissected RLNs on survival. DISCUSSION The generally accepted prognostic factors for RLN metastasis and survival of endometrial cancer were evaluated in this study (1- i 5). Further, the new proposed positive rate of metastasis of dissected RLNs was evaluated for discriminating the prognosis in the patients with RLN metastasis, so that the optimal treatment protocol could be suggested. As would be expected, each of the clinicopathological factors was related to RLN metastasis and survival of this disease. Nevertheless, only a few of them had independent prognostic significance. Additionally, the independence of these factors was variable, depending on the prognostic significance judged by the RLN metastasis or the survival. Jpn J Clin OncoI1998;28(11) 1.00 N Rl.N metastasis: N: Negative (0=270) P: Positive (0=40) .. 0.60 .~ ;: P=O.OOOI ~ Positive rate of metastasis of dissected RLNs: Rl: <25% R2: >25% '0 '" .", ~ ~ 8 0.40 c, P=O.OOOI R R2 P 0.20 0.00 ~...L.w....c-,-,-,-,-.......w.'-U.J..~...L.w....c-"-'-U--'--'-'-'--,-,-,-"-'-U.J..~..LW-LJ..Lu..Ll..LL.L"-'--U...u..w...........-,-,-,-"-w....L~...w o 1 2 3 4 5 6 7 9 8 10 11 13 12 14 15 16 17 Years after Surgery b 1,00 0.80 ~ .~ 0.60 "l "0 '" ~8 0,40 ""' N: Gl (0=143) P: G2 and G3 (0=167) P=O.OOI 0,20 0.00 ~~~~~~~~~~~~~~~~~~~~~ o 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 Years after Surgery 1.00 N 0.80 0.60 18 18 677 In this study, deep myometrial invasion (>2/3), cervical invasion and severe lymphatic permeation (many) were found to be independent prognostic factors for RLN metastasis and in tum the RLN metastasis was an independent prognostic factor for survival. Hence their influence on survival was rooted in the RLN metastasis. They were harmful to survival, consistent with previously reported findings (1-3,5,12-15). As gross myometrial invasion could be assessed preoperatively (12,18), it provided a marker for preoperative prediction ofRLN metastasis. In the patients with cervical invasion, the cancerous lesion in the cervix was easy to metastasize to the paracervical area. Therefore, radical hysterectomy should be performed in these patients so that the possible paracervical involvement could be cleaned. Radiation therapy was another choice in treatment of cervical invasion (4,12,17). Once lymphatic permeation has occurred, cancer cells have the potential to metastasize to the lymph node. Vascular invasion was strongly correlated with lymphatic permeation. In Inoue et al.'s study, lymphatic permeation and vascular invasion were combined as vessel invasion and were found to be a reliable prognostic factor for survival (14). On the other hand, poor pathological grade, positive peritoneal cytology and RLN metastasis were found to be independent prognostic factors for survival. Patients with endometrial cancer of poor pathological grade advanced quickly because such cancerous lesion tended to be associated with deep myometrial invasion, lymphatic permeation and cervical invasion from which RLN metastasis occurred (12,13,19). Hence, once endometrial cancer of poor pathological grade has been diagnosed, treatment should be initiated as soon as possible. Positive peritoneal cytology significantly influences survival of this disease, consistent with results in previous reports (4,5). Other reports revealed inconsistent results that peritoneal cytology did not play an important role in the prognosis of patients who had well differentiated endometrial cancer (6,7). We noted that their patients had no RLN metastasis. The extent ofRLN assessment in the new FIGO staging system for endometrial cancer can vary from simple transperitoneal palpation with excisional biopsy of enlarged lymph nodes, via directed biopsies of one or two lymph nodes from each lymph node area, to formal pelvic and paraaortic lymphadenectomy (1). However, the average positive rate of metastasis of dissected RLNs was found to be only 22% in this study and Creasman et al. (16) reported that even in stage I disease there are still 7-13 % patients with positive pelvic lymph nodes. Additionally, at present there is no reliable method for accurate preoperative or intraoperative assessment of RLN metastasis. Hence lymph node biopsy alone is insufficient in the treatment of this disease. To 0.40 Peritoneal cytology N:Negative(n=251) P:Positive(0=59) 0.20 P=O.OOI 0.00 '-'-'-'-'.........................u..w-"-'-'-'-'-'-'-'-' ...........U-W...L~...u..w.~~..........w......w-W-W..'-'-'-U.~'-'-'-'-"~~ o 1 2 3 4 5 6 7 8 9 10 It YearsafterSurgery 12 13 14 15 16 17 18 Figure 1. Kaplan-Meier estimation of survival probability in 310 patients with endometrial cancer, according to (a) RLN metastasis, (b) pathological grade and (c) peritoneal cytology. Panel (a) shows that RLN metastases, especially with a status of 225% positive rate of metastasis of dissected RLNs, significantly influenced the survival probability in patients with this disease compared with those who had no RLN metastasis. Panels (b) and (c) shows that poorer differentiated pathologies and positive peritoneal cytology significantly influenced the survival probability in these patients compared with those who had well differentiated pathology and negative peritoneal cytology, respectively. 678 Prognostic factors of endometrial cancer obtain accurate staging, pelvic and paraaortic lymphadenectomy is necessary in the treatment of this disease. Instead of the number of metastatic nodes in total dissected RLNs, the positive rate of metastasis of dissected RLNs was used to evaluate the survival rate of patients with this disease. This is because there was a variation in the number of dissected RLNs in each patient. There are at least three causes of this variation. First, there may be variations in the actual number of RLNs in each patient. Second, sometimes there is difficulty in performing lymphadenectomy in obese patients or in patients with other severe medical problems (1). Third, there are variations in the technique to pick up the lymph nodes from the dissected lipo-Iymphatic tissue. The positive rate of metastasis in dissected RLNs was considered to be a more scientific evaluation for prediction of survival than the number of metastatic nodes in dissected RLNs, e.g. five of 15 or five of 30 are completely different. Patients with RLN metastasis were classified into FIGO stage lIlC and had a poorer survival rate than those without it. However, even in these patients, survival was distinguishable by the positive rate of metastasis of dissected RLNs. The survival curve of patients with a 2::25% positive rate of metastasis of dissected RLNs fell steeply soon after surgery. It is presumed that the high positive rate of nodal metastasis represents high malignant biological properties of the cancer and predisposes the patients to local and distant relapse. On the other hand, patients with a low positive rate of nodal metastasis had much better 5-year survival rates than patients with a high positive rate. The explanation for this phenomenon is as follows. In the patients with a low positive rate of nodal metastasis, as the number of metastatic nodes was small, it was fairly easy to dissect them thoroughly. As a result, local recurrence was relatively low in this subgroup of patients with RLN metastasis. There is evidence that distant recurrence was low when local recurrence was low (17). Second, the low positive rate of nodal metastasis may reflect a relatively early period in the natural history of the disease or a relatively low malignant biology of the cancer. The results in this study did not show an influence on survival of site and distribution ofRLN metastasis. This was in accordance with Kadar et al. 's report that the difference in survival between women with paraaortic lymph node (PAN) and pelvic lymph node (PLN) metastasis was not significant (4). However, it was contrary to Yokoyama et al. 's result that the survival of patients with PAN metastasis was poorer than that of patients with only PLN metastasis (8). Our view is that, in endometrial cancer, low segmental PAN and PLN metastasis are nodal metastasis of the same location so that they have a similar influence on survival. In any case, PAN metastasis suggests that the disease has progressed to a severer extent. The 5-year survival rate was not satisfactory with surgery alone in the treatment of patients with endometrial cancer and RLN metastasis, poorly differentiated lesion and positive peritoneal cytology. Hence postoperative radiation therapy and/or chemotherapy should be employed to improve the survival rate of these patients (9). Additionally, for patients with deep myometrial invasion, cervical invasion, lymphatic permeation and vessel invasion, postoperative treatment should be initiated if RLN metastasis has been identified. Acknowledgment This study was supported in part by the Japan-China Medical Association Sasakawa Medical Scholarship Fund. References 1. Larson DM, Connor GP, Broste SK, Krawisz BR, Johnson KK. Prognostic significance of gross myometrial invasion with endometrial cancer. Obstet Gynecol 1996;88:394-8. 2. Kaku T, Tsuruchi N, Tsukamoto N, Hirakawa T, Kamura T, Nakano H. Reassessment of myometrial invasion in endometrial cancer. Obstet Gynecol 1994;84:979-82. 3. Cohen CJ. Advanced (FIGO stages III and IV) and recurrent cancer of the endometrium. In: Coppleson M, Monaghan JM, Morrow CP, Tattersall MH, editors. Gynecologic Oncology, 2nd ed. Edinburgh: Churchill Livingstone, 1992;778-98. 4. Kadar N, Homesley HD, Malfetano JH. Prognostic factors in surgical stage III and IV cancer of the endometrium. Obstet Gynecol 1994;84:983-6. 5. Creasman WT, Rutledge FN. The prognostic value of peritoneal cytology in gynecologic malignant disease. Am J Obstet Gynecol 1976; 110:773-81. 6. Vecek N, Marinovic T, Ivic J, Jukic S, Nola M, Dzanic-Cemalovic N, et al. Prognostic impact of peritoneal cytology in patients with endometrial cancer. Eur J Gynaecol OncoI1993;14:380-5. 7. Kato T, Yamada T, Tanemura K, Tsunematsu R, Ohmi K, Sonoda T. Clinical significance of peritoneal cytology in patients with endometrial adenocarcinoma. SankaTo Fujinka 1989;56:1759-63 (in Japanese). 8. Yokoyama Y, Maruyama H, Sato S, Saito Y Indispensability of pelvic and paraaortic lymphadenectomy in endometrial cancers. Gynecol Oncol 1997;64:411-7. 9. Onda T, Yoshikawa H, Mizutani K, Mishima M, Yokota H, Nagano H, et ai. Treatment of node-positive endometrial cancer with complete node dissection, chemotherapy and radiation therapy. Br J Cancer 1997;75:1836-41. 10. Kodama S, Kase H, Tanaka K, Matsui K. Multivariate analysis of prognostic factors in patients with endometrial cancer. lnt J Gynaecol Obstet 1996;53:23-30. 11. Behbakht K, Yordan EL, Casey C, DeGeest K, Massad LS, Kirschner CV, et ai. Prognostic indicators of survival in advanced endometrial cancer. Gynecol OncoI1994;55:363-7. 12. Lampe B, Kurzl R, Hantschmann P. Prognostic factors that predict pelvic lymph node metastasis from endometrial cancer. Cancer 1994;74:2502-8. 13. Kosary CL. FlGO stage, histology, histologic grade, age and race as prognostic factors on determining survival for cancers of the female gynecological system: an analysis of 1973-87 SEER cases of cancers of the endometrium, cervix, ovary. vulva and vagina. Semin Sure Oncol 1994 10:31-46. 14. Inoue Y, Obata L, Abe K, Ohmura G, Doh K, Yoshioka T, et ai. The prognostic significance of vascular invasion by endometrial cancer. Cancer 1996;78:1447-51. 15. Tsuruchi N, Kaku T, Kamura T, Tsukamoto N, Tsuneyoshi M, Akazawa K et ai. The prognostic significance of Iymphovascular space invasion in endometrial cancer when conventional hemotoxylin and eosin staining is compared to immunohistochemical staining. GynecoIOnco/1995;57:307-12. 16. Creasman WT, Morrow CP, Bundy L. The surgical pathological spread pattern of endometrial cancer. A Gynecologic Oncology Group Study. Cancer 1987;60:2035-41. 17. Com BW, Lanciano RM, Agostino RD, Kiggundu E, Dunton CJ, Purser P,et al. The relationship of local and distant failure from endometrial cancer: defining a clinical paradigm. Gynecol Oneal 1997 66:411-6. 18. Tang X, Muramatsu Y, Yajima M, Sonoda T. Endometrium-myometrium ratio: a newly proposed diagnostic parameter on magnetic resonance imaging assessment of myometrial invasion by endometrial cancer. Jpn J Clin Oncol 1993;23:278-83. 19. Sonoda T. Clinical diagnosis of endometrial cancer: especially for discussion about primary lesion. Sanka To Fujinka 1987;56:2117-25 (in Japanese).