Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
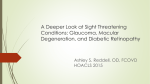
THE PROGRESSION OF DIABETIC RETINOPATHY: INITIATION AND CONTINUATION OF TREATMENT AMANDA S LEGGE, B.S. ABSTRACT CASE REPORT: A forty-four year-old white male has been experiencing progressive diabetic retinopathy changes for the past eight years. Retinopathy began as mild and nonproliferative; however because of uncontrolled blood sugars it progressed to proliferative diabetic retinopathy with clinically significant macular edema. Currently the patient’s fasting blood sugars and hemoglobin A1C levels are controlled, but the retinopathy continues to progress. Several laser treatments O.U., antivascular endothelial growth factor injections O.D., and a vitrectomy O.S. have been performed in the past. He returns for a second opinion regarding a recurring vitreous hemorrhage O.S. DISCUSSION: Diabetic retinopathy has been well studied over the past several decades. Its progression can lead to microvascular leakage, occlusion, and ischemia which correlate with a progressed deterioration of vision if left untreated. Therefore it is important to understand the pathology and treatment considerations along the continuum of diabetic retinopathy to make a prompt diagnosis and begin and continue an appropriate intervention plan. Diabetic retinopathy is the most prevalent microvascular complication in the eye and has the potential to cause irreversible vision loss1. Chronic hyperglycemia is responsible for biochemical alterations in the retinal vasculature such as inflammatory responses and upregulation of vascular endothelial growth factor (VEGF)2. These events result in microaneurysms, vascular permeability, vascular occlusion, and neovascularization. The progression to retinal ischemia can cause damaging, permanent vision loss. Therefore timely diagnosis and intervention is needed. The following case report illustrates the progression of diabetic retinopathy in a formerly noncompliant type 2 diabetic. This case also highlights the initiation of appropriate treatment and the on-going efforts to halt the progression of continuing vision loss in this young patient. CASE REPORT HISTORY The patient is a 44-year-old white male. His medical history is positive for type 2 insulin- dependent diabetes mellitus for 13 years, hypertension, hyperlipidemia, anemia, chronic kidney disease, hypothyroidism, and coronary artery disease. The patient’s diabetes is managed with 60 units of Lantus in the morning and 15 units in the evening, 1000mg of metformin twice per day, 10mg glipizide twice per day, and NovaLog before each meal per sliding scale. In addition the patient is medicated with amlopidine, carvedilol, furosemide, simvastatin, and ranitidine. The patient’s most current Hemoglobin A1C blood level was 6.8% approximately 3 weeks prior to presentation which is quite well controlled compared to past levels. At the time of initial retinopathy diagnosis his A1C levels varied between 9.5 and 13.4% and fasting blood sugars ranged between 297 and 356mg/dL. He reported that he was noncompliant with medication and diet directives in the past; however recently he has been much more compliant. According to previous records, diabetic retinopathy was first noted in 2004 as mild nonproliferative diabetic retinopathy (NPDR) without macular edema (CSME). Visual acuities were measured to be 20/20 O.D., O.S. O.S. for a total of 538 spots. The NVD regressed status post PRP treatments O.U. Clinically significant macular edema was noted in 2007 O.S. and focal laser treatment was warranted. Also at this exam a small area of disc neovascularization (NVD) was seen O.D. This was confirmed with fluorescein angiography. The patient was treated with two sessions of pan-retinal photocoagulation (PRP) O.D for a total of 1563 spots. The NVD O.D. recurred and injections of antiVEGF agents were pursued in early 2010. At that presentation the vision had deteriorated to 20/60 O.D. and 20/40 O.S. The patient received 3 injections of Lucentis and 2 injections of Avastin O.D over the course of 6 months at 4 week intervals. The fluorescein prior to these injections showed the leakage from the NVD as well as the focal and panretinal laser scars O.U. (figure 1) Following the injections there was no leakage that could be detected O.D., O.S. One year later, 2008, the patient developed CSME O.D. and NVD O.S. He was then treated with focal laser O.D. and one session of PRP Figure 1. Fluorescein Angiography demonstrating the window defects from focal laser treatment, microaneurysms, and leakage secondary to the disc neovascularization O.D. in later images. Early 2011 he developed a vitreous hemorrhage O.S. that was obscuring the macula. He underwent an additional 930 spots of PRP O.S. at that presentation; however the vitreous hemorrhage remained unresolved for 4 months. He underwent a vitrectomy O.S. approximately 6 months ago at another clinic. His vision at that time was 20/80 O.D. and 20/100 O.S. October 2011 a second vitreous hemorrhage occurred O.S. which decreased his vision to count fingers at 3 feet. He was told observation would be appropriate for a time by an outside ophthalmologist and returns at this presentation for a second opinion. The patient admits that he has been well educated about the diagnosis, management, and possible complications of diabetes. He has improved his management of glucose levels throughout the day for the past 18 months. He plans to continue to do this. His ocular history is also significant for primary open angle glaucoma O.D., O.S. that is well controlled with dorzolamide 2% twice per day O.U. The patient reports good compliance. DIAGNOSTIC DATA The patient’s most current exam revealed his unaided visual acuities were 20/80 O.D. and 20/100 O.S. at distance without improvement on pinhole. Pupils were equal, round, and reactive to light with a 1+ afferent defect O.S. Extraocular motility testing found no restrictions of muscle movement. Confrontation visual fields were full to finger counting O.D., O.S. Intraocular pressures were measured to be 20 mmHg O.D., O.S. Anterior segment evaluation was remarkable for mild anterior blepharitis O.U. and trace off-axis posterior subcapsular cataracts O.U. The iris was clear without signs of neovascularization O.U. Goniscopy revealed the most posterior structure in all quadrants to be the ciliary body face. Minimal pigment was noted without signs of neovascularization. Posterior segment evaluation O.D. revealed several microaneurysms throughout the posterior pole without macular edema. Focal laser treatment scars were seen temporal to the macula. The right optic nerve head showed mild fibrous tissue formation secondary to receded NVD. The left eye revealed a large, dense, preretinal hemorrhage with fibrovascular proliferation in the posterior pole without clinically significant macular edema. (figure 2, 3) Residual vitreous from an incomplete vitrectomy was seen inferiorly with a resolving vitreous hemorrhage. Extensive PRP scars were seen in the periphery O.U. Optical Coherence Tomography (OCT) was performed to better assess the macula O.S. Although the image was of poor quality because of the preretinal hemorrhage, macular edema was seen. This swelling may be attributable to diabetic macular edema pathology or secondary to the preretinal blood and consequential intrearetinal swelling. No cystic spaces were seen. (figure 4) Figure 2. Fundus Photography illustrating the focal laser scars temporal to the macula O.D. and extensive subretinal blood surrounding the macula O.S. Not pictured is the vitreous hemorrhage that has settled inferiorly O.S. Figure 3. Fundus Autofluorescence photography illustrating the extensive preretinal hemorrhage O.S. and focal laser scars O.U. Figure 3. Optical coherence tomography illustrating the normal macular thickness O.D. and macular edema O.S., although this is a poor scan resulting from the preretinal blood DIAGNOSIS AND FOLLOW-UP A one-month follow up revealed a resolving vitreous and pre-retinal hemorrhage O.S. The right eye remained in stable condition. He reported the vision was stable. OCT was repeated and showed no sign of macular edema O.D., O.S. Subretinal fluid, new neovascularization, or hemorrhage was not detected during dilated fundoscopy. At this time the retinopathy remains stable O.D. and improving O.S. The patient was once again advised to maintain tight blood sugar control and adhere to all primary care physician directives. No further intervention at this time was recommended; however the patient understands to return to clinic if his vision worsens. He also understands that future interventions may be necessary based on the evolution of the diabetic retinopathy. This includes a second vitrectomy O.S. to remove the residual vitreous. Patient education was critical during this case with regards to diabetic ocular and systemic complications. Over the course of 3 years the patient lost a significant amount of weight and has much better glycemic control. The patient now regularly visits his primary care provider, endocrinologist, diabetic educator, and diabetic nutritionist to keep tight control of his blood glucose and HgA1C levels. The patient was educated to maintain careful monthly follow ups until his retinal status stabilizes. DISCUSSION Diabetic retinopathy begins and progresses due to prolonged, uncontrolled, hyperglycemia. In this state, biochemical alterations result in damage to the retinal vasculature. This leads to microaneurysms, vascular permeability, vascular occlusion, and neovascularization which potentially cause permanent vision loss2. Diabetic retinopathy is a complex disease with numerous factors contributing to the overall progression. Subclinical vascular inflammation is the first indication of diabetic effects in the eye. Inflammatory agents intracellular adhesion molecule 1 (ICAM1) and its receptor, CD18, play an important role in retinopathy initiation and progression. ICAM1/CD18 is responsible for leukocyte adhesion in the pathogenesis of early diabetic retinopathy. Leukocyte stasis ultimately causes a breakdown in the bloodretinal barrier and areas of capillary nonperfusion with consequential hypoxia, the driving force behind retinopathy progression4. The initiation of the ICAM1/CD18 mechanism causes capillary wall weakness triggering microaneurysm formation, the first visible sign of diabetic retinopathy on fundus examination or fluorescein angiography5. This vessel wall weakness is thought to be caused by capillary pericyte loss secondary to a decrease in platelet derived growth factor – B (PDGF-B). This is triggered directly by a hyperglycemic state as well as indirectly with the initiation of the ICAM1/CD18 inflammation process6. Microaneurysms in isolation are benign; however they can cause capillary closure resulting in acellular capillaries which contributes to retinal non-perfusion, initiation of proliferative retinopathy, and deterioration of vision7. Another key molecule in diabetic retinopathy is VEGF, a well documented protein that contributes to retinopathy pathogenesis in diabetes. Typically in the healthy retina VEGF is found as a small percentage of the retinal proteins. With increasing hypoxic conditions, VEGF is released at higher concentrations in order to increase oxygenation. VEGF is not only a mediator of new blood vessel formation, but also of vascular permeability. Both contribute to the pathogenesis of visually-impairing forms of diabetic retinopathy: proliferative retinopathy and clinically significant macular edema, respectively8. Additionally some studies link VEGF to the inflammatory cascade by upregulating ICAM1, thus creating a cycle which accelerates the progression of retinopathy9. Certainly a multitude of other factors also contribute to the initiation and progression of diabetic retinopathy including serum cholesterol levels, uncontrolled hypertension, anemia, and other biochemical mediators such as protein kinase C-beta7,10,11,12. All contribute to decreased capillary oxygenation, retinal vessel leakage, and neovasularization, the major risk factors for severe vision loss in diabetic retinopathy12. Understanding the biochemical alterations in diabetic retinopathy allows for the development of appropriate treatment strategies to prevent progression. Classic treatment strategies include photocoagulation, anti-VEGF intravitreal injections, and steroid intravitreal injections. Possible alternative treatments include non-steroidal antiinflammatory agents, aldose reductase inhibitors, growth hormone antagonists, and protein kinase C inhibitors. Photocoagulation timing and effectiveness in diabetic retinopathy was determined by two major studies: the Diabetic Retinopathy Study (DRS) and the Early Treatment Diabetic Retinopathy Study (ETDRS). The DRS qualified high-risk characteristics of PDR and showed a 50% reduction in severe vision loss when these eyes were treated with photocoagulation13. The ETDRS defined the timing for scatter photocoagulation. It showed that eyes treated before high-risk characteristics of PDR were present had no long term benefit14. Therefore it is important to control serum glucose levels, hypertension, and cholesterol in NPDR and monitor closely until these characteristics are seen10,11. Patient education plays an ever important role when a patient presents with NDPR as with any sign of diabetic complications. The ETDRS also defined treatment guidelines for diabetic macular edema. It showed that treatment with focal or grid photocoagulation decreased the risk of moderate visual loss for all eyes with diabetic macular edema by approximately 50%15. Thus treatment is warranted for any diabetic patient presenting with clinically significant macular edema whether through photocoagulation, or more recently intravitreal injections. Both intravitreal triamcinolone and anti-VEGF agents have been proven to reduce macular edema and resolve neovascularization in PDR when photocoagulation is ineffective. Intravitreal steroids or anti-VEGF agents along with protein kinase C inhibitors downregulate VEGF within the retina and reduce vascular proliferation and leakage, thus reducing neovascularization and diabetic macular edema respectively16. Currently anti-VEGF agents are used more often because they have little potential to raise intraocular pressure or induce cataracts as triamcinolone does17. At present, photocoagulation, intravitreal steroid, and anti-VEGF injections are the mainstay of ocular intervention for PDR or macular edema, although other considerations are being investigated, such as non-steroidal anti-inflammatory agents (NSAIDs). In the past the ETDRS considered aspirin in diabetic retinopathy patients; however it was concluded that aspirin was neither beneficial nor harmful to retinopathy progression18. Recent research has well established inflammation and platelet aggregation in the process of diabetic disease, so NSAIDs are being closely looked at again. Studies have shown high-dose aspirin, twice the dose as given during ETDRS, meloxicam, a cyclo-oxygenase 2 inhibitor, and etaneracept, a soluble tumor necrosis factor receptor, suppressed diabetic retinal ICAM-1 expression, leukocyte adhesion, and blood retinal barrier breakdown in a rodent model19. This is now being studied in human trials. Whether aspirin slows the progression of diabetic retinopathy or not in humans, it is known that aspirin reduces morbidity and mortality by 17% from cardiovascular disease in the diabetic population18. This makes aspirin a viable treatment adjunct to reduce cardiovascular morbidity and mortality without negatively affecting the retina. Oral administration of protein kinase C-β (PKCβ) inhibitors and antagonists of growth hormone (GH) are also being investigated as alternative methods to treat diabetic retinopathy. PKC-β directly activates VEGF20. GH and insulin-like growth factor have also been implicated in the VEGF cascade21. Thus the inhibition of these biochemical mediators through oral administration may have the same effect as intravitreal injections with more convenience and potentially less adverse effects. When properly treated, the 5-year risk of blindness in PDR is reduced by 90% and risk of visual loss from macular edema is 50%15; however prevention is the best method to reduce the risk of visual loss from diabetic retinopathy. Several studies have shown that tight glycemic control prevents or slows the progression of diabetic retinopathy including the Diabetes Control and Complications Trial (DCCT), Epidemiology of Diabetes Interventions and Complications Trial (EDIC), and the United Kingdom Prospective Diabetes Study (UKPDS). This information should be presented to any patient known to have hyperglycemia or diabetes. Patient education is the key to preventative care with regards to diabetic retinopathy. Unfortunately the patient in this case did not tightly control his glycemic levels and diabetic retinopathy ensued. Several intervention strategies were employed to slow the progression; however none have completely halted it at this point. Proper patient education and directives were given and he has since lowered his risk of progression significantly by controlling his blood glucose levels and HgA1C. Close monitoring of the patient’s ocular and systemic status will continue. Further interventions will be considered if the patient’s vision or retinal status decrease over time. REFERENCES 1 Wilde, S., et. al., Global Prevalence of Diabetes: Estimates for the Year 2000 and Projections for 2030. Diabetes Care, 2004; 27: 1047-1053. 2 Ciulla, T., et. al., Ocular Perfusion Abnormalities in Diabetes. Acta Ophthal Scand, 2002; 80(5): 468-477. 3 Cogan, D., Toussaint, D., Kuwabara, T., Retinal Vascular Patterns: IV Diabetic Retinopathy, Arch Ophthal 1961; 66(3): 366-378. 4 Joussen, A., et. al., A Central Role for Inflammation in the Pathogenesis of Diabetic Retinopathy, The FAFSEB Journal, 2004; 18: 1450-1452. 5 Cunha, JZ, Diabetic Macular Edema, Eur J Ophthal., 1998 Jul-Sept; 8(3): 127-130. 6 Hammes, H., et. al., Pericytes and the Pathogenesis of Diabetic Retinopathy, Diabetes, 2002, Oct; 51(10): 3107-3112. 7 Kohner, EM, Sleightholm, M., Does Microaneurysm Count Reflect Severity of Early Diabetic Retinopathy?, Ophthalmology, 1986, May; 93(5): 586-589. 8 Boulton, M., Foreman, D., Williams, G., McLeod, D., VEGF Localization in Diabetic Retinopathy, Br J Ophthalmol., 1998; 82: 561-568. 9 Joussen, AM, et. al., Retinal Vascular Endothelial Growth Factor Induces Intracellular Adhesion Molecule-1 and Endothelial Nitric Oxide Synthase Expression and Initiates Early Diabetic Retinal Leukocyte Adhesion in vivo, Am J Pathol 2002; 160(2): 501-509. Fong, DS, et. al., Subretinal Fibrosis in Diabetic Macular Edema, ETDRS Report no. 23, Arca Ophthal, 1997; 15: 873-877. 11 Shrier, RW, Estacio, RP, Esler, A, Mehler, P, Appropriate Blood Pressure Control in Hypertensive and Normotensive Type 2 Diabetes Mellitus: A Summary of the ABCD Trial, Nat Clin Prac Nephrol, 2007, Aug; 3(8): 428-438. 12 Davis, MD, et. al., Risk Factors for High Risk Proliferative Diabetic Retinopathy and Severe Vision Loss, ETDRS Report No. 18, Invest Ophthalmol Vis Sci, 1998; 39: 233-252. 13 Diabetic Retinopathy Study Group, Photocoagulation Treatment of Proliferative Diabetic Retinopathy. DRS Report No. 2 Ophthalmology, 1978; 85: 82-105. 14 Early Treatment of Diabetic Retinopathy Study Group, Early Photocoagulation for Diabetic Retinopathy. ETDRS Report No. 9, Ophthalmology, 1991; 98(suppl): 767-785. 15 Early Treatment of Diabetic Retinopathy Study Group, Photocoagulation for Diabetic Macular Edema. ETDRS Report No. 4 Int Ophthalmol Clin 1987; 27: 265-272. 16 Martidis, A., et. al., Intravitreal Triamcinolone for Refractory Diabetic Macular Edema. Ophthalmology, 2002, May; 109(5): 920-927. 17 Avery, R., et. al., Intravitreal Bevacizumab (Avastin) in the Treatment of Proliferative Diabetic Retinopathy, Ophthalmology 2006, Oct: 113(10): 1695-1705. 18 Early Treatment of Diabetic Retinopathy Study Group, Effects of Aspirin Treatment on Diabetic Retinopathy, ETDRS Report No. 8, Ophthalmology, 1991; 98: 757-765. 19 Joussen, AM, et. al., Non-steroidal Anti-inflammatory Drugs Prevent Early Diabetic Retinopathy via TNF-alpha Suppression, FASEB J, 16: 438-440. 20 Frank, R., Potential New Medical Therapies for Diabetic Retinopathy: Protein Kinase C Inhibitors. Am J Ophthalmol, 2002, May; 133(5): 693-698. 21 Wilkinson-Berka, J., Wraight, C., & Werther, G., The Role of Growth Hormone, Insulin-Like Growth Factor, and Somatostatin in Diabetic Retinopathy. Curr Med Chem, 2006, Nov; 13(27): 3307-3317. 10