Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
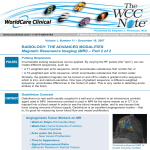
Effectiveness of dynamic contrast-enhanced MRI in evaluating clinical responses to neoadjuvant chemotherapy in breast cancer LIU Yin-Hua, YE Jing-Ming, XU Ling, HUANG Qing-Yun, ZHAO Jian-Xin, DUAN Xue-Ning, QIN Nai-Shan, WANG Xiao-Ying LIU Yin-Hua ( ), YE Jing-Ming, HUANG Qing-Yun, ZHAO Jian-Xin, DUAN Xue-Ning, Department of General Surgery, Breast Disease Center, Peking University First Hospital, Xi Shi Ku Street 8, 100034 Beijing, P. R. China e-mail: [email protected] Tel.: +86-(0)10-83575053 XU Ling Department of Medical Oncology, Breast Disease Center, Peking University First Hospital, Beijing, P. R. China QIN Nai-Shan, WANG Xiao-Ying Department of Radiology, Peking University First Hospital, Beijing, P. R. China Abstract Purpose: To investigate the effectiveness of dynamic contrast-enhanced MRI for evaluating clinical responses to neoadjuvant chemotherapy in breast cancer patients. Patients and Methods: We examined patients receiving neoadjuvant chemotherapy for primary breast cancer between October 2007 and September 2008. Dynamic contrast-enhanced MRI was used to examine breast tumors prior to and after neoadjuvant chemotherapy. This MRI examination assesses tumors using Response Evaluation Criteria in Solid Tumors (RECIST). The Miller-Payne grading system was used as a histopathological examination to assess the effect of the treatment. We examined the relationship between the results of RECIST and histopathological criteria. In addition, we used time-signal intensity curves (MRI T-SI) to further evaluate the effects of neoadjuvant chemotherapy on tumor response. Results: MRI examination of patients completing four three-week anthracycline-taxanes chemotherapy treatment revealed that there were no CR cases, 58 PR cases, 29 SD cases, and four PD cases. The effectiveness of neoadjuvant chemotherapy (CR + PR) was 63.7% (58/ 91). The postoperative histopathological evaluations revealed the following: seven G5 (pCR) cases (7.7%), 39 G4 cases (42.9%), 16 G3 cases (17.6%), 23 G2 cases (25.3%), and six G1 cases (6.6%). The effectiveness (G5 + G4 + G3) is 68.1% (62/91). MRI T-SI standards classified 53 effective cases, 29 stable cases, and nine progressing cases. These results indicate that the treatment was 58.2% effective (53/91) overall. Conclusions: Dynamic contrast-enhanced MRI and histopathological standards were highly correlated. Importantly, MRI T-SI evaluation was found to be useful in assessing the clinical significance of neoadjuvant chemotherapy. Key words Breast cancer, neoadjuvant chemotherapy, MRI, time-signal intensity curve, response evaluation Introduction Breast cancer treatment has advanced over the past two decades, achieving a better outcome for women. Neoadjuvant chemotherapy has become an established part of treatment of stage Ⅱ and Ⅲ breast cancer, and the indications for use of this modality are constantly expanding [1]. Use of neoadjuvant chemotherapy allows for assessment of response to cytotoxic drugs in vivo, which is not only clinically relevant but also critical in terms of research endeavors assessing chemoresistance and response [2]. Accurate assessment of neoadjuvant response is a critical element in monitoring and assessing treatment strategies. Recently magnetic resonance imaging (MRI) has become increasingly popular in breast imaging, and several studies have demonstrated a high correlation between tumor size as measured by MRI and histopathologic examination after neoadjuvant chemotherapy [3] [4]. But tumor imaging is unable to identify changes in the tumor density or tumor angiogenesis. The enhancement kinetics, as represented by the time-signal intensity (T-SI) curves, differ significantly for benign and malignant enhancing lesions [5] and may therefore changed after neoadjuvant chemotherapy. So in this study, we examined the changes in T-SI curves to further evaluate breast cancer treatment response besides the changes of tumor size by MRI and tried to assess the neoadjuvant chemotherapy response multifold. Patients and Methods 1.1 Patients: Women under 70 years of age admitted to our center between October 2007 and September 2008 for primary breast cancer took part in this study. Ninety-one patients met the following criteria for inclusion in the study: all exhibited measurable breast lesions, and pre-B ultrasound-guided core needle biopsy diagnosis of breast invasive ductal carcinoma (not otherwise specified ). All patients underwent ultrasound-guided fine needle aspiration cytology of the axillary lymph nodes. No patients had contraindications to neoadjuvant chemotherapy, and all completed a full course of the treatment. The neoadjuvant chemotherapy consisted of four three-week anthracycline-taxane treatments. Complete MRI results were obtained for each patient, and abdominal B-type ultrasounds, chest X-rays and bone scans (except for distant metastasis) were conducted. We found no indication of serious damage to the heart, liver or kidney function (indicated by a Karnofsky score greater than 70) in any patient. 1.2 Methods: 1.2.1 Neoadjuvant chemotherapy: A complete course of neoadjuvant chemotherapy involved four three-week cycles of anthracyclines-taxanes chemotherapy treatment. Each patient took 50 mg/m2 of pirarubicin or epirubicin 75 mg/m2 on the first day of each three-week cycle, and 75 mg/m2 of docetaxel or 175 mg/m2 of paclitaxel on the second day. Patients were then required to repeat the same medications on the first and second day 21 days after the start of the previous cycle. The same three-week cycle was repeated four times for a complete course of neoadjuvant chemotherapy, and all patients completed the treatment course. Dynamic contrast-enhanced MRI was then conducted within 10 to 14 days of the first day of the second and fourth cycles to evaluate the effectiveness of the neoadjuvant chemotherapy. 1.2.2 Imaging examination methods: The dynamic contrast-enhanced MRI was conducted using a GE Signa infinity 1.5T Twinspeed MRI scanners, with breast dedicated four-channel phased-array surface coils, in a three plane scan. Dynamic contrast-enhanced scanning utilized volume imaging for breast assessment (VIBRANT) sequence sagittal scan: repetition time: 6.9 ms; echo time: 2.7 ms;flip angle: 15°; field of vision (FOV): 20*20mm; matrix: 324 ×288; thickness 5 mm, zero difference technique Zip2; scan time: 58 s) Continuous scans were taken eight times (eight phrases) before and after injection of the contrast agent Gd-DTPA to enhance the clarity of the image. A dose of 0.2 mmol/kg Gd-DTPA was injected to the vein in front of the elbow at a speed of 2.0 ml/s. Post-image processing was performed with an AW4.2 workstation using FuncTool software (region of interest; ROI) to test for significant changes, as well as to perform 3D image reconstruction, measure the longest diameter of the breast tumor, draw dynamic enhanced curves, and identify curve type according to curve shape (Figure 1) [5]. 1.2.3 Dynamic contrast-enhanced breast MRI examination: MRI examinations were conducted before the first cycle chemotherapy and within 10 to 14 days after the first day of the second and fourth three-week treatments to evaluate the clinical significance of neoadjuvant chemotherapy. The MRI examination measure of tumor size was based on the RECIST (1.0) [6] , and the measurement of tumor progress was based on changes in T-SI curves, as shown in Table 2. MRI measurement of neoadjuvant chemotherapy efficiency = (CR + PR) / total number of cases × 100%. MRI measurement of time - signal intensity curve efficiency = effective case/ total number of cases × 100%. 1.2.4 Surgical procedure: Ten to fourteen days after four cycles of neoadjuvant chemotherapy, the treatment response was evaluated, and used to determine whether breast-conserving surgery or modified radical mastectomy were appropriate. 1.2.5 Histopathological response evaluation of neoadjuvant chemotherapy: The removed tissue was routinely converted into paraffin embedded sections, and the largest diameter of tumor was measured under a microscope. We used the Miller-Payne histopathological grading system to assess treatment response (Table 1) [7] . The total effectiveness rate of the neoadjuvant chemotherapy was calculated by (G3 + G4 + G5) cases / total number of cases × 100%. 1.2.6 Statistical methods: Pearson correlation analyses were used to test the relationship between MRI and the histopathological assessment of the longest diameter of the residual tumor after neoadjuvant chemotherapy. We considered a difference to be statistically significant if P <0.05. Analysis was performed using SPSS15.0 software. Results 2.1 Patient data: Ninety-one patients met the experimental inclusion criteria. Ages ranged between 27 and 69 years, with a median age of 49 years. Twenty-six patients were diagnosed with clinical stage IIA (28.57%), Forty-seven (51.65%) exhibited clinical stage IIB, and eighteen (19.78%) exhibited clinical stage IIIA. Modified radical mastectomies were performed in sixty-five cases, and breast-conserving surgery was performed on the remaining twenty-six patients. 2.2 Dynamic contrast-enhanced MRI evaluation of neoadjuvant chemotherapy: The outcome data of the complete neoadjuvant chemotherapy course according to RECIST criteria (1.0) was as follows: no cases of CR, fifty-eight cases of PR, twenty-nine cases of SD, and four cases of PD. The effectiveness of neoadjuvant chemotherapy according to MRI assessment was 63.7% (CR + PR cases / total cases = 58/91). 2.3 MRI T-SI evaluation of neoadjuvant chemotherapy: MRI T-SI standards classified fifty-three effective cases, twenty-nine stable cases and nine progressive cases. The overall effectiveness of neoadjuvant chemotherapy according to MRI T-SI evaluation was 58.2% (53/91). 2.4 Histopathological evaluation of neoadjuvant chemotherapy: We conducted histopathological evaluation of breast tumors using the Miller-Payne grading system to evaluate the clinical effectiveness of neoadjuvant chemotherapy. There were seven cases (7.7%) classed as G5 (pCR), thirty-nine (42.9%) as G4, sixteen (17.6%) as G3, twenty-three (25.3%) as G2, and six (6.6%) as G1. The overall effectiveness of neoadjuvant chemotherapy according to the Miller-Payne assessment was 68.1% (G5 + G4 + G3 cases/ total cases = 62/91). 2.5 Relationship between dynamic contrast-enhanced MRI and histopathological evaluation of neoadjuvant chemotherapy: The average residual tumor diameter measured by MRI was 2.12 ± 1.37 cm, while the microscopic residual tumor pathology-ray measurement of the average diameter was 1.83 ± 1.53 cm. Pearson correlation tests revealed that MRI and histopathology measurements of residual tumor tissue were highly correlated (r = 0.650, P <0.001). Fifty-eight cases exhibited PR according to MRI evaluation, whereas sixty-two cases were judged effective according to histopathological evaluation. Consistency between the two measurements was 79.3% (Table 3). There were thirty-three SD + PD cases according to MRI evaluation, and the treatment in seventeen cases was judged ineffective by histopathlogical evaluation. The consistency between the two measurements was 69.2%. 2.6 Relationship between MRI T-SI and histopathological evaluation: Fifty-three cases were judged effective by MRI T-SI assessment, compared to sixty-two effective cases classified by histopathological examination. Consistency between the two measurements was 79.2%. The other thirty-eight cases were found to be ineffective by MRI T-SI criteria, and eighteen cases were judged ineffective by histopathological examination. The consistency between these two measures was 69.2%, as shown in Table 4. 2.7 The relationship between the RECIST measure of the dynamic contrast-enhanced MRI and MRI T-SI evaluation: Thirty-six cases were found to be effective using RECIST evaluation standards, whereas twenty-nine cases were classified as effective using MRI T-SI measures. The consistency between the two measurements was 80.6%. Figure 2 was a case which was judged as PR using RECIST evaluation standards and also classified as effevtive using MRI T-SI measures. Sixteen cases were judged to be SD and PD cases by RECIST standards, whereas thirteen cases were classified ineffective by MRI T-SI. The consistency between these two measurements was 82.3%. RECISTS standards also classified twenty-nine cases as SD, whereas sixteen of which were classified as effective by MRI T-SI criteria. Twelve of these cases were judged effective by histopathological examination. The consistency between MRI T-SI and histopathological measurements was 75% (12/16) (Table 5). Four cases were PD under RECIST and effective under MRI T-SI. One of these four cases was classified as G5, and three were classified as G2 according to histopathological examination. Thirty-eight cases were classified as stable or progressive according to MRI T-SI, twenty-two of which were judged effective under MRI. The consistency between the measurements was 77.3%. Discussion Neoadjuvant chemotherapy is a potentially useful breast cancer treatment. However, the effectiveness of this therapy relies on the accuracy of tumor progression measurements. The World Health Organization (WHO) established a tumor classification system in the 1980s. The topic of solid tumor cancer therapy evaluation criteria remains contentious. In 2000, the European Association for Cancer Research and Treatment (EORTC), the National Cancer Research (NCI) and the National Cancer Institute of Canada (NCIC) amended the WHO standards developing and publishing a new evaluation standard called the RECIST 1.0. These new criteria involve precise and accurate single-track diameter measurement, instead of the conventional two-track diameter measurement. The RECIST 1.0 evaluation standard is now widely used in clinical practice. In 2009, the European Journal of Cancer published an updated and more comprehensive version of the RECIST, version 1.1 [8] . Recently, some researchers have explored different combinations of MRI evaluation criteria used to assess the effectiveness of neoadjuvant chemotherapy for breast cancer [9] [10], but the use of histopathological examination and MRI T-SI curves to evaluate of neo-adjuvant chemotherapy has been largely neglected. In the present study we examined the clinical response of breast cancer patients receiving neo-adjuvant chemotherapy. Tumor evaluation standards including RECIST criteria and histopathological examination (the Miller-Payne grading system) were used to assess tumor response. In addition, changes in MRI T-SI were also used to evaluate the clinical effectiveness of neoadjuvant chemotherapy. The results revealed that microscopic measurements of residual tumor tissue following neoadjuvant chemotherapy using dynamic contrast-enhanced MRI and histopathological evaluation were highly correlated (r = 0.650, P <0.001). Among the fifty-eight cases classified as PR under RECIST, forty-six were also classified as effective under histopathological examination. Consistency between these two measurements was found to be 51.5%. The overall measurement consistency between RECIST criteria, dynamic contrast-enhanced MRI measures and histopathological examination was 69.2%. It could be concluded that dynamic contrast-enhanced MRI examination is an effective method for assessing the clinical response of neoadjuvant chemotherapy according to RECIST, and our data indicate that it has a relatively high correlation with histopathological measures. We found that the measurement consistency between MRI T-SI curve and histopathological standards for effective cases was 79.2%, and 47.4% for ineffective cases respectively. RECISTS evaluation used in conjunction with MRI T-SI curves may enhance the accuracy of tumor assessment. Of the twenty-nine SD cases classified by RECIST in the present study, sixteen were considered to be effective using MRI T-SI, and twelve were considered effective by histopathological examination. The measurement consistency between MRI T-SI curves and histopathological examination was 75% (12/16). RECIST criteria also classified four cases as PD. MRI T-SI measures also indicated those cases as effective. One of those four cases was classified as G5, and three were considered G2 according to histopathological examination. These results suggest that more attention should be paid to the related MRI T-SI curve evaluation for cases classified as SD or PD using RECISTS standards. For cases classified as effective by MRI T-SI curve evaluation, histopathological examination could help to provide a better insight into tumor response, which may allow physicians to assess whether there is a need to alter the medication involved in neoadjuvant chemotherapy. Core needle biopsy could be used as an additional tool for identifying the tumor response. Tumor imaging anatomy and physical plane measurement are the basis of the RECIST standards. Physical measurement is unable identify changes in the tumor density or tumor angiogenesis. Change in tumor size is an important indicator of tumor response. However, other indicators can also be used. Many variables impact on MRI imaging, and may have affected image quality and measurement accuracy in our present study. Histopathological examination measures are independent of tumor size variation, so bias can occur depending on the physician’s assessment. More research is necessary to examine the effectiveness of joint standards in evaluating the clinical significance of neoadjuvant chemotherapy. MRI T-SI measures can help as an indication of tumor blood flow dynamics and perfusion parameters. The use of MRI T-SI curves in conjunction with core needle biopsy may help to better identify and avoid mismeasurement of tumor progress. We examined the effectiveness of MRI in evaluating the effects of neo-adjuvant chemotherapy. Our data indicated that the use of dynamic contrast-enhanced MRI together with MRI T-SI improved evaluations of neo-adjuvant chemotherapy. In addition, the results suggested that histopathological evaluation should be used in conjunction with dynamic contrast-enhanced MRI and MRI T-SI, and that these three measures were relatively highly correlated. Related functional MRI parameters, such as dynamic contrast-enhanced [11] , diffusion-weighted imaging (DWI) [12] and proton magnetic resonance spectroscopy (MRS) [13] are other potentially useful clinical tools that require further investigation. References: 1. Shannon C, Smith I. Is there still a role for neoadjuvant therapy in breast cancer? Crit Rev Oncol Hematol 2003;45:77-90. PMID: 12482573. 2. Fisher B, Bryant J, Wolmark N, Mamounas E, Brown A, Fisher ER, et al. Effect of preoperative chemotherapy on the outcome of women with operable breast cancer. J Clin Oncol 1998;16:2672-2685. PMID: 9704717. 3. Rosen EL, Blackwell KL, Baker JA, Soo MS, Bentley RC, Yu D,et al. Accuracy of mri in the detection of residual breast cancer after neoadjuvant chemotherapy. AJR Am J Roentgenol 2003;181:1275-1282. PMID: 14573420. 4. Londero V, Bazzocchi M, Del Frate C, Puglisi F, Di Loreto C, Francescutti G, et al. Locally advanced breast cancer: Comparison of mammography, sonography and mr imaging in evaluation of residual disease in women receiving neoadjuvant chemotherapy. Eur Radiol 2004;14:1371-1379. PMID: 14986052. 5. Kuhl CK, Mielcareck P, Klaschik S, Leutner C, Wardelmann E, Gieseke J, et al. Dynamic breast mr imaging: Are signal intensity time course data useful for differential diagnosis of enhancing lesions? Radiology 1999;211:101-110. 10189459. 6. Therasse P, Arbuck SG, Eisenhauer EA, Wanders J, Kaplan RS, Rubinstein L, et al. New guidelines to evaluate the response to treatment in solid tumors. European organization for research and treatment of cancer, national cancer institute of the united states, national cancer institute of canada. J Natl Cancer Inst 2000;92:205-216. PMID: 10655437. 7. Ogston KN, Miller ID, Payne S, Hutcheon AW, Sarkar TK, Smith I, et al. A new histological grading system to assess response of breast cancers to primary chemotherapy: Prognostic significance and survival. Breast 2003;12:320-327. PMID: 14659147. 8. Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, et al. New response evaluation criteria in solid tumours: Revised recist guideline (version 1.1). Eur J Cancer 2009;45:228-247. PMID:19097774. 9. Ye JM, Xu L, Wang DM, Zhao JX, Zhang LB, Duan XN, et al. Prospective study on the role of MRI and b ultrasonography in evaluating the tumor response to neoadjuvant chemotherapy in breast cancer]. Zhonghua Wai Ke Za Zhi 2009;47:349-352. PMID: 19595011. 10. Uematsu T, Yuen S, Kasami M, Uchida Y. Comparison of magnetic resonance imaging, multidetector row computed tomography, ultrasonography, and mammography for tumor extension of breast cancer. Breast Cancer Res Treat 2008;112:461-474. PMID: 18193352. 11. Pickles MD, Lowry M, Manton DJ, Gibbs P, Turnbull LW. Role of dynamic contrast enhanced mri in monitoring early response of locally advanced breast cancer to neoadjuvant chemotherapy. Breast Cancer Res Treat 2005;91:1-10. PMID: 15868426. 12. Meisamy S, Bolan PJ, Baker EH, Bliss RL, Gulbahce E, Everson LI, et al. Neoadjuvant chemotherapy of locally advanced breast cancer: Predicting response with in vivo (1)h mr spectroscopy--a pilot study at 4 t. Radiology 2004;233:424-431. PMID:15516615. 13. Pickles MD, Gibbs P, Lowry M, Turnbull LW. Diffusion changes precede size reduction in neoadjuvant treatment of breast cancer. Magn Reson Imaging 2006;24:843-847. PMID: 16916701. . Figure 1 Schematic drawing of the time-signal intensity curve types. Type Ⅰ corresponds to a straight (Ⅰa) or curved (Ⅰb) line; enhancement continues over the entire dynamic study. Type Ⅱ is a plateau curve with a sharp bend after the initial upstroke. Type Ⅲ is a wash out time course. A B C D E F Figure 2 A case was judged as PR using RECIST evaluation standards and also classified as effevtive using MRI T-SI measures. (Figure 2A and 2B were dynamic contrast-enhanced breast MRI and T-SI curves taken before the first cycle chemotherapy. Figure 2C and 2D were taken at 10 days after the 2nd cycle chemotherapy. Figure 2E and 2F were taken at 12 days after the 4th cycle chemotherapy. Table 1 Miller-Payne histological grading system Grade Definition No change or some alteration to individual malignant cells but no Grade 1 (G1) reduction in overall cellularity A minor loss of tumor cells but overall cellularity still high; up to Grade 2 (G2) 30% loss Grade 3 (G3) Between an estimated 30% and 90% reduction in tumor cells A marked disappearance of tumor cells such that only small Grade 4 (G4) clusters or widely dispersed individual cells remain; more than 90% loss of tumor cells No malignant cells identifiable in sections from the site of the tumor; only vascular fibroelastotic stroma remains often Grade 5 (G5) containing macrophages. However, ductal carcinoma in situ (DCIS) may be present Table 2 Time-Signal Intensity (T-SI) curve types and corresponding clinical significance. Clinical Changes in the Type of T-S1 Curves Evaluation Effective Type III T-SI curve became Type I or Type II, Type II T-SI curve became type I Stable No change Progressive Type II T-SI curve became type III Table 3: MRI and histopathological evaluations of neoadjuvant chemotherapy MRI Evaluation PD PR SD Total G1 0 2 4 6 Histopathological Evaluation G2 G3 G4 3 0 0 10 10 31 10 6 8 23 16 39 G5 1 5 1 7 Total 4 58 29 91 Table 4: MRI T-SI curve and histopathological evaluations of neoadjuvant chemotherapy MRI T-SI Evaluation Effective Stable Progressive Total G1 4 2 0 6 Histopathological Evaluation G2 G3 G4 7 10 27 11 4 11 5 2 1 23 16 39 G5 5 1 1 7 Total 53 29 9 91 Table 5: MRI T-SI curves and histopathological evaluation of neoadjuvant chemotherapy for SD patients Histopathological Evaluation MRI T-SI Evaluation Effective Total G1 G2 G3 G4 G5 2 2 5 6 1 16 Stable & Progressive Total 2 8 1 2 0 13 4 10 6 8 1 29