Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
86
"Reperfusion Injury" by Oxygen-Derived
Free Radicals?
Effect of Superoxide Dismutase Plus Catalase, Given at the
Time of Reperfusion, on Myocardial Infarct Size, Contractile
Function, Coronary Microvasculature, and
Regional Myocardial Blood Flow
Karin Przyklenk and Robert A. Kloner
Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017
Do oxygen-derived free radicals, generated at the time of reperfusion, lethally injure viable,
previously ischemic myocardium, damage vascular endothelium, and impair recovery of
postischemic contractile function? To address these issues, 23 anesthetized open-chest dogs
underwent 2 hours of left anterior descending coronary artery occlusion followed by 4 hours of
reperfusion. Immediately prior to reflow, each dog was randomized to receive either the free
radical scavenging agents superoxide dismutase (SOD)+catalase, or saline alone. SOD+catalase
had no significant beneficial effect on infarct size measured by triphenyltetrazolium staining:
area of necrosis averaged 38.5±6.1% vs. 46.3±6.2% of the area at risk in treated compared
with control animals respectively (p=NS). Furthermore, infusion of SOD+catalase did not alter
contractile function of the viable subepkardium: mean segment shortening (measured using
sonomicrometry) at 4 hours postreperfusion was - 2 3 ± 5 % of baseline, preocclusion values in
controls dogs and - 2 4 ± 9 % of preocclusion values in animals that received the scavenging
agents. However, SOD+catalase treatment preserved the endocardia! microvasculature (assessed
by semiquantitative electron microscopic analysis) and enhanced regional myocardial blood
flow after reperfusion. Specifically, mean score for microvascular injury was 0.41±0.14 vs.
0.10±0.08 (p<0.05) in control compared with SOD+catalase treated groups, and blood flow
averaged 0.56±0.11 vs. 1.27±0.33 ml/min/g tissue (p<0.05), respectively, in the previously
ischemic endocardium at 2 hours postreflow. Thus, SOD+catalase given at the time of
reperfusion had no acute beneficial effect on either the extent of myocyte necrosis or
postischemic contractile function in this canine model. SOD+catalase did, however, attenuate
both endocardial vascular injury and the "low reflow" phenomenon. These data suggest that
microvascular injury and low reflow following prolonged (2 hour) but transient coronary
occlusion may be mediated by oxygen-derived free radicals generated at the time of reperfusion.
(Circulation Research 1989;64:86-96)
T
here is no question that timely reperfusion of
an occluded coronary artery can salvage
previously ischemic myocardium. This in
turn can both reduce the extent of ischemia-induced
necrosis and enhance long-term recovery of regional
From the Department of Internal Medicine, Division of Cardiology, Harper Hospital and Wayne State University, Detroit,
Michigan.
Presented in part at the 60th Scientific Sessions of the American Heart Association, Anaheim, California, November 1987.
Supported in part by National Institutes of Health SCOR
HL-26215, Bethesda, Maryland.
Address for reprints: Karin Przyklenk, PhD, Heart Institute/
Research, Hospital of the Good Samaritan, 616 South Witmer
Street, Los Angeles, CA 90017.
Received January 25, 1988; accepted June 29, 1988.
contractile function. The benefits of early reperfusion in evolving acute myocardial infarction, first
observed in experimental models of transient coronary occlusion,'-3 have in recent years become
clinically feasible with the advent of techniques
such as angioplasty, thrombolysis, and surgical
revascularization.4-6
While reduction of infarct size and preservation
of left ventricular function are clearly desirable,
recent evidence suggests that reperfusion may be a
"double-edged sword." 7 That is, restoration of
blood flow may salvage one population of previously ischemic myocytes, yet lethally injure other
viable, previously ischemic cells. Specifically, this
phenomenon—termed "reperfusion injury"—is
Przyklenk and Kloner
Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017
thought to be a consequence of cytotoxic and highly
reactive oxygen-derived free radicals ("OH and O2~),
generated at a greatly accelerated rate upon reintroduction of O2 to previously ischemic tissue.8 Increased
concentrations of oxygen-centered radicals have been
documented in reperfused myocardium by spin resonance spectroscopy.910 Furthermore, prolonged
exposure of isolated perfused heart preparations to
free radical generating systems has been shown to
result in contractile dysfunction and severe ultrastructural damage to both the myocytes and vascular
endothelium." In spite of this in vitro evidence, the
concept of reperfusion injury in in vivo models of
prolonged coronary occlusion (i.e., >40 minutes)
followed by reperfusion remains controversial.
In the present study, we administered the potent
free radical scavenging agents superoxide dismutase (SOD)+catalase immediately prior to reflow in
an attempt to determine whether oxygen-derived
free radicals, generated at the time of reperfusion,
1) lethally injure viable, previously ischemic myocardium, 2) damage the coronary vasculature, and/
or 3) impair recovery of postischemic contractile
function in an anesthetized, open-chest canine model
of transient (2 hour) coronary artery occlusion.
Materials and Methods
Surgery
Forty-five mongrel dogs of either sex, weighing
an average of 20.4±5.0 kg, were anesthetized with
sodium pentobarbital (30 mg/kg i.v.), intubated,
and ventilated with room air. Cannulae were inserted
into the left external jugular vein for administration
of drugs and fluids and into the left common carotid
artery for measurement of heart rate and arterial
pressures. A left thoracotomy was performed
through the fifth intercostal space, the ribs were
retracted, and the heart was exposed and suspended in a pericardial cradle. The left atrial appendage was then cannulated for later infusion of either
SOD+catalase or saline and for injection of radioactive microspheres for measurement of regional
myocardial blood flow (RMBF). A Millar (Houston,
Texas) micro-tipped pressure transducer was positioned within the left ventricular (LV) cavity via the
left atrial appendage for measurement of LV pressure and its first derivative, LV dP/dt.
A small segment of the left anterior descending
coronary artery (LAD) was dissected free of surrounding tissue and isolated, usually just distal to its
first major diagonal branch. The artery was then
briefly occluded for less than 5 seconds to delineate
the extent of cyanosis.
Regional contractile function in the soon-to-be
ischemic subepicardium was assessed using sonomicrometry, the details of which have been presented
previously.1213 One pair of ultrasonic crystals, used
to measure segment shortening (SS), was inserted
via small scalpel incisions into the superficial subepicardial layer at a depth of 2-4 mm. The crystals
Reperfusion Injury by Free Radicals?
87
were positioned in the center of the LAD bed at a
separation of 5-12 mm and were oriented parallel to
the minor axis of the heart. Segment shortening,
arterial and LV pressures, and dP/dt were monitored continuously throughout the experiment on a
Gould recorder (Cleveland, Ohio).
Protocol
After initial baseline measurement of hemodynamic parameters and SS, each dog received a
bolus dose of lidocaine (1.5 mg/kg i.v.). The LAD
was then abruptly occluded with atraumatic vascular clamps. Hemodynamic parameters and SS
were assessed at 30 minutes, 1 hour, and 2 hours
postocclusion, while RMBF was measured by
injection of radioactive microspheres at 30 minutes postocclusion.
Before reperfusion at 2 hours postocclusion, each
dog was randomized to receive one of the following
treatments: 1) SOD (Sigma Chemical, St. Louis,
Missouri; 3,200 IU/mg; 5 mg/kg)+catalase (Sigma;
2,500 IU/mg; 5 mg/kg) dissolved in 5 ml of saline as
an intra-atrial bolus given 1 minute before reperfusion. This was followed by a continuous intra-atrial
infusion of SOD (5 mg/kg/hr)+catalase (5 mg/kg/
hr) dissolved in saline at a rate of 1 ml/min. This
infusion was maintained throughout the 4 hours of
reperfusion. 2) Saline (5 ml) given into the left
atrium at 1 minute before reperfusion, followed by a
continuous intra-atrial infusion at a rate of 1 ml/min
for the remainder of the protocol.
A second measurement of RMBF was made at 2
hours postreperfusion, while hemodynamic parameters and SS were assessed at 30 minutes, 1 hour, 2
hours, 3 hours, and 4 hours postreperfusion.
Immediately before the animals were killed at 4
hours postreperfusion, in vivo transmural needle
biopsies were obtained from the center of the previously ischemic LAD bed, subdivided into endocardia! and epicardial halves, and rapidly fixed by
immersion in 2.5% glutaraldehyde in 0.1 M sodium
cacodylate buffer for subsequent electron microscopic analysis. The LAD was then reoccluded and
monastral blue pigment (0.5 ml/kg) injected into the
coronary circulation via the left atrium to delineate
the in vivo occluded bed size, or area at risk (AR).
Immediately after injection of the dye, the dogs
were killed by intracardiac injection of potassium
chloride and the hearts excised.
After marking the positions of the ultrasonic
crystals, the hearts were cut into six to eight
transverse sections, parallel to the atrioventricular
groove. Epicardial and endocardial contours of
the basal surfaces of the heart slices, and the
margins of the occluded LAD bed, were traced
onto acetate sheets. Correct placement of the
crystals (i.e., within the center of the area at risk
at a depth of approximately 2-4 mm) was confirmed at this time. To distinguish necrotic from
normal tissue, the heart slices were then incubated
for 10 minutes in a 1% solution of triphenyltetra-
88
Circulation Research
Vol 64, No 1, January 1989
zolium chloride (TTC) at 37° C. 1415 The heart
slices, and boundaries of the area of necrosis (AN)
within each heart slice, were retraced onto the
acetate sheets, and the hearts were then fixed by
immersion in 10% neutral buffered formalin.
Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017
Analysis
After fixation, right ventricular tissue was trimmed
off each heart slice, and the slices were weighed.
Contours of the LV, AR, and AN were cut from the
tracing of the heart slices and weighed; AN and AR
were corrected for the weight of the tissue slice and
summed for each heart. AN was then expressed as
both a percentage of the AR (i.e., AN/AR) and
percentage of the LV (AN/LV).
For measurement of RMBF, blocks of tissue
from both the center of the previously ischemic
LAD bed and remote, normal myocardium were cut
and subdivided into endocardial, midmyocardial,
and epicardial segments. RMBF was then quantified by the method of Domenech et al.16
Tissue samples obtained for electron microscopic
analysis were cut into 1 mm3 blocks, fixed overnight
in 2.5% glutaraldehyde in 0.1 M sodium cacodylate
buffer at a pH of 7.2, and then postfixed with 1.0%
osmium tetroxide in 0.1 M sodium cacodylate (pH
7.2). The samples then underwent dehydration in
graded ethanols and propylene oxide, infiltration,
and were embedded in plastic resin (Embed 812,
Electron Microscopy Science, Fort Washington,
Pennsylvania). Semithin sections (1 fim) were cut
and stained with toluidine blue and examined under
light microscopy. Thin sections (approximately 70
nm) were then cut from selected blocks, stained with
uranyl acetate followed by lead citrate, and examined on a Zeiss EM 10 CA electron microscope.
Analysis was performed on photographs obtained
at magnifications of approximately x2,000-4,000.
Myocytes were graded in a semiquantitative fashion
from 0 to 4 using the following accepted grading
system, the details of which have been published
previously17:0=normal; 1 =minimal ischemic changes
(I bands, glycogen loss, nuclear clumping, and margination); 2=moderate ischemic changes (the findings in 1, plus early intermyofibrillar and sarcoplasmic reticular edema, mitochondrial edema); 3 =
moderately severe ischemic changes (findings in 2
plus subsarcolemmal blebs, gaps, marked edema,
presence of mitochondrial dense bodies); and 4=
severe architectural disruption, sarcolemmal breaks,
contraction bands and mitochondrial disruption.
The coronary microvasculature was similarly
graded on a scale of 0 to 1, where 0=normal;
1=severely injured (decreased pinocytotic vesicles,
presence of endothelial gaps, endothelial blebs,
fibrin deposition, and microscopic hemorrhage);
0.5=mildly injured (some but not all of the above
abnormalities). All electron microscopic analysis
was performed by a trained observer (R.A.K.) who
was blinded with respect to the treatment group of
any given specimen. Three to seven independent
fields of view were graded from both the endocardium and epicardium of each dog.
Heart rate, mean arterial pressure, and LV dP/dt
were measured and averaged over five continuous
cardiac cycles for each sample period. In addition,
dP/dt was used to define the separation between the
ultrasonic crystals at specific points in the cardiac
cycle: end diastolic lengths (EDL) were measured
at the onset of the rapid rise of dP/dt, while end
systolic lengths (ESL) were measured at peak negative dP/dt.1213 EDL and ESL were measured from
three well-separated cardiac cycles in each sample
period, averaged, and used to compute segment
shortening (SS), defined by convention as 1213
Values of SS measured during each sample period
were then normalized and expressed as a percentage of their normal, baseline value measured before
LAD occlusion (i.e., %SS).
Statistics
Dogs with high collateral blood flow during coronary occlusion and a small AR (i.e., animals that
were not sufficiently ischemic to develop myocyte
necrosis) were excluded from the final analysis.
Specifically, our exclusion criteria, established prior
to the onset of the protocol, were values of RMBF
in the "ischemic" endocardium greater than 0.10
ml/min/g tissue during LAD occlusion, and/or an
AR less than 10% of the LV. No attempt was made
to revive dogs that fibrillated during occlusion or
during reperfusion.
Mean values of AN/AR, AN/LV, AR/LV, RMBF,
and electron microscopic score were compared
between the control and SOD+catalase treated
groups by t tests for unpaired data. Hemodynamics
and absolute values of SS were compared between
groups preocclusion, at 120 minutes postocclusion
(i.e., immediately before reperfusion), and at 30,
120, and 240 minutes postreperfusion; similarly,
%SS (normalized to baseline, preocclusion values)
were compared at 120 minutes postocclusion and at
30, 120, and 240 minutes postreperfusion. Bonferroni's correction for multiple comparisons was then
applied.18 All values are expressed as mean±SEM
and are considered to differ significantly if p<0.05.
Results
Of the 45 dogs entered into the study, 15 animals
died before randomization: 14 died due to ventricular fibrillation within the first 3-30 minutes postocclusion, and one animal died because of respirator
failure. One control animal fibrillated upon reperfusion, and one control died 30 minutes postreperfusion. Five animals were excluded from the study
because they were not sufficiently ischemic during
occlusion (i.e., endocardial RMBF during occlusion
>0.10 ml/min/g tissue and AR/AR<10%). Specifi-
Przyklenk and Kloner
Reperfusion Iiyury by Free Radicals?
89
TABLE 1. Heroodynamlc Parameters
Occlusion
Pre
Heart rate (beats/min)
Control (n= 11)
149±6
SOD+CAT(n = 12)
145±7
Mean arterial pressure (mm Hg)
Control (n= 11)
126±5
SOD+CAT(/i=12)
122±5
Peak positive LV dP/dt (mm Hg/sec)
Control (n= 11)
1,716+59
SOD+CAT(n=12)
l,808±88
Reperfusion
30'
120'
30'
120'
143±5
139+7
141+7
132+7
141±7
132±7
137±8
123+7
144±11
119±7
127±5
124±7
123+5
114+8
114±5
110±8
U6±5
101+7
107+6
121+7
1,596±68
1,684±118
1,618+62
1,629+132
1,471 ±61
1,533±112
1,465±71
1,526±87
l,302±74
1,369±51
240'
SOD, superoxide dismutase; CAT, catalase.
Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017
cally, values of RMBF in these five excluded animals averaged 0.45±0.12,0.54±0.15, and 0.73+0.06
ml/min/g tissue in the endocardium, midmyocardium, and epicardium during coronary artery
occlusion, and infarcts were limited to small foci at
the tips of the papillary muscles (approximately 02% of the LV). Thus, a total of 23 animals—11
controls and 12 treated with SOD+catalase—were
included in the final analysis.
Hemodynamic Parameters
Heart rate, mean arterial pressure, and LV dP/dt
were comparable in SOD+catalase treated and control dogs both before randomization (i.e., preocclusion and throughout 2 hours of LAD occlusion) and
after reperfusion and treatment (Table 1). Thus,
infusion of SOD+catalase had no significant effect
on hemodynamics in this model.
Regional Myocardial Blood Flow
Both groups of dogs were equally ischemic at 30
minutes postocclusion (Figure 1). For example,
mean RMBF in the ischemic midmyocardium was
0.07±0.02 and 0.05±0.02 ml/min/g tissue in control
and treated animals respectively (p=NS).
SOD+catalase given at the time of reperfusion
significantly increased blood flow to the previously
ischemic endocardium and midmyocardium: in the
previously ischemic midwall, RMBF averaged
0.42±0.05 vs. 0.82±0.19 ml/min/g tissue in control
versus treated dogs respectively (p<0.05; Figure 1).
In contrast, RMBF in the normally perfused circumflex bed did not differ between the two groups
following reperfusion: 0.87±0.06 vs. 0.74±0.11 ml/
min/g in the midmyocardium (p=NS; Table 2).
These data indicate that SOD+catalase selectively
enhanced blood flow after reperfusion in the previously ischemic tissue.
Regional Contractile Function
Baseline values of segment shortening averaged
approximately 16% in both control animals and
those later assigned to receive SOD+catalase. In
addition, all dogs were equally dyskinetic during 2
hours of ischemia: mean SS was -3.4±0.9% vs.
-3.6±1.1% (or -27±9% vs. -23±8% of baseline,
preocclusion values) in control compared with
treated groups at 2 hours postocclusion (p=NS;
Table 3).
Contractile function in the salvaged subepicardium remained markedly "stunned" or dyskinetic
throughout the 4 hours of reperfusion and treatment.
SOD+catalase had no apparent beneficial effect on
postischemic contractile function: SS after 2 hours of
reperfusion averaged —2.4±0.6% vs. 0±1.7% (or
-18±5% vs. -2±11% of preocclusion values) in
control versus treated dogs respectively ( / J = N S ) .
Infarct Size and Area at Risk
In vivo area at risk (AR/LV) was essentially
equal in both control animals (19.0±0.8%) and
those that received SOD+catalase (18.7±1.8%;
p=NS; Figure 2).
No significant difference in infarct size (expressed
as a percentage of the AR) was observed between
ALL DOGS
REGIONAL MYOCARDIAL BLOOD FLOW
Ischemic LAD Bed
2.000
OCCLUSION
REPERFUSION
.J5 1.500I
1.000
^
m
0.500
\
a:
0.000
ENDO
C3
MID
CONTROLS
(n-10)
EPI
ENDO
m
MID
EPI
SOD + CATALASE
(n-12)
FIGURE 1. Regional myocardial blood flow (RMBF) in
the center of the left anterior descending coronary artery
(LAD) bed measured 30 minutes postocclusion and at 2
hours postreperfusion in control and superoxide dismutase (SOD)+catalase treated dogs. *p<0.05 vs. the corresponding control value. ENDO, endocardium; MID,
midmyocardium; EPI, epicardium.
90
Circulation Research
TABLE 2.
Vol 64, No 1, January 1989
Regional Myocardial Blood Flow in tbe Normally Perfused Circumflex Coronary Artery Bed (ml/min/g tissue)
30' Postocclusion
Control (n=10)
SOD+CAT (/i =12)
Endo
l.ll±.10
1.01±.12
2 Hours Postref>erfusion
Mid
0.94±.08
0.92±.12
Epi
O.77±.O8
O.82±.1O
Endo
Mid
0.96±.07
0.73±.ll
O.87±.O6
0.74+.11
Epi
O.72±.O5
0.78±.13
Endo, endocardium; Mid, midmyocardium; Epi, epicardium; SOD, superoxide dismutase; CAT, catalase.
Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017
control and SOD+catalase treated groups: AN/AR
averaged 46.3±6.2% in control animals compared
with 38.5±6.1% in animals that received SOD+
catalase (p=NS; Figure 2). Similar results were
obtained when AN was expressed as a percentage
of the total LV mass: AN/LV was 9.1 ±1.5% vs.
8.2±1.7% for control compared with treated dogs,
respectively (p=NS; Figure 2). These data indicate
that SOD+catalase, initiated at the time of reperfusion, had no significant beneficial effect on the
extent of necrosis produced by 2 hours of LAD
occlusion and 4 hours of reperfusion.
The relation between AN/AR and collateral flow
to the ischemic midmyocardium during LAD occlusion for both control and treated groups is illustrated in Figure 3. The regression line for dogs that
received SOD+catalase fell below that obtained for
the saline controls (suggesting a possible reduction
in infarct size); however, the y intercepts of the two
lines did not differ when analyzed statistically
(p>0.20). Similar plots were obtained when either
endocardial, epicardial, or weighted mean transmural flow was used as the dependent variable.
While these data imply that SOD+catalase given
at the time of reperfusion may have limited infarct
size in some animals, this did not approach statistical significance because of the considerable variability in both collateral flow and AN/AR in the
canine model. 23
Electron Microscopic Analysis
Biopsies for electron microscopic analysis were
obtained from the center of the previously ischemic
LAD bed in 20 of the 23 dogs that successfully
completed the protocol.
Injury to the vascular endothelium was attenuated by infusion of SOD+catalase: mean score for
microvascular injury in the previously ischemic
endocardium was significantly less in treated aniTABLE 3.
mals (0.10±0.08) than in the saline controls
(0.41 ±0.14; p<0.05; Table 4 and Figure 4). This
marked preservation of the endocardial vascular
endothelium by SOD+catalase is illustrated in the
electron micrographs shown in Figure 5. In contrast, no differences in the degree of epicardial
vascular injury or myocyte damage were noted
between control and treated groups (Table 4).
Discussion
Do oxygen-derived free radicals, generated at the
time of reperfusion, lethally injure viable, previously ischemic myocardium? To address this issue,
several investigators have administered free radical
scavenging agents or antioxidants in an attempt to
reduce infarct size in the canine model of transient
coronary occlusion. Allopurinol,1920 oxypurinol,21
SOD+catalase22 and SOD alone, 1923 given before
or during coronary occlusion, have all been shown
to reduce the extent of necrosis produced by 60-90
minutes of ischemia and 4-24 hours of reflow.
These data appear to support the concept of' 'reperfusion injury"; however, recent evidence indicates
that oxygen-centered radicals are also formed during occlusion in species (such as dog and man) in
which native collateral vessels provide residual
blood flow (and therefore low levels of molecular
oxygen) to the ischemic tissue.24-25 As free radicals
formed during prolonged periods of coronary occlusion appear to contribute to myocyte necrosis,2627
studies which address reperfusion injury by initiating treatment before or during occlusion must be
interpreted with caution.
In contrast, other studies have failed to document
a reduction in infarct size in response to early
treatment (before or during occlusion) with free
radical scavengers or antioxidants. Allopurinol,21-28
oxypurinol,2930 and SOD31-33 in these studies did
not reduce the extent of myocyte necrosis produced
Regional Contractile Function: Segment Shortening in the Subepicardium of the LAD Bed
Pre
I. % of preocclusion values
Control (n= 11)
100%
SOD+CAT(n=12)
100%
11. Absolute values
Control (n= 11)
SOD+Cat(n=12)
15.6±1.2%
16.3±1.0%
Occlusion
30 min
Reperfusion
120 min
30 min
120 min
240 min
-27±8%
-20±8%
-27±9%
-23±8%
-8±8%
+7±12%
-18±5%
-2±11%
-23±5%
-24±9%
-3.6±0.8%
-3.1±1.2%
-3.4±0.9%
-3.6±l.l%
-1.2±1.4%
+ 1.3±1.7%
-2.4±0.6%
0±1.7%
-3.2±0.7%
-3.6+1.3%
SOD, superoxide dismutase; CAT, catalase.
Przyklenk and Kloner
Reperfusion hjjury by Free Radicals?
91
0.050
0.100
0.150
0.200
MIDMYOCARDIAL RMBF (ML/MIN/G TISSUE)
0.250
ALL DOGS
0.000
AN/AR (X)
—-""CONTROLS
AN/LV (X)
C D CONTROLS
AR/LV (X)
SOD + CATALASE
(n-12)
Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017
FIGURE 2. Infarct size data (i.e., area of necrosis [AN]
expressed as a percentage of the area at risk [AR], AN
expressed as a percentage of the total left ventricular
weight [LVj, and AR expressed as a percentage of the
LV) for control and treated dogs.
by 40 minutes to 3 hours of occlusion and 6 hours to
4 days of reperfusion.
Only two other studies3435 have addressed the
topic of reperfusion injury by administering a free
radical scavenger at the time of reperfusion. Ambrosio et al34 found that recombinant human SOD given
"only at the moment" of refiow significantly reduced
infarct size produced by 90 minutes of ischemia and
48 hours of reperfusion. These data provide evidence in support of reperfusion injury mediated by
oxygen-derived free radicals. In contrast, Nejima et
al,35 who also studied the extent of necrosis produced by 90 minutes of coronary occlusion, found
no difference in infarct size, measured 1 week
postreperfusion, in dogs treated with SOD+catalase
compared with controls.
In the present study, we found that SOD+catalase
administered 1 minute before reperfusion did not
reduce infarct size associated with 2 hours of coronary artery occlusion and 4 hours of reflow when all
dogs were considered. However, further retrospective analysis of the data suggested that the efficacy
of SOD+catalase treatment in any given animal in
our study may have been influenced by the degree
of collateral blood flow during LAD occlusion.
Mean RMBF to the midmyocardium for the 22 dogs
in which flow measurements were obtained was
0.06 ml/min/g tissue. In the subgroup of animals
TABLE 4.
— - S O D + CATALASE
FIGURE 3. Relation between regional myocardial blood
flow to the midmyocardium during LAD occlusion and
area of necrosis expressed as a percentage of the area at
risk for I) control animals (dashed line): ANIAR=(-241.8)
(mid-RMBF)+60.1; r= -0.56 andp=NS2) SOD+catalase
treated animals (solid line): ANIAR=(-219.0)(midRMBF)+48.9; r= -0.78 and p<0.01. Note that the regression line obtained for the SOD+catalase treated animals
falls below that obtained for the controls, but intercepts
do not differ significantly.
with higher than average collateral flow (RMBF in
the ischemic midmyocardium >0.06 ml/min/g), AN/
AR was lower in SOD+catalase treated dogs
(18.3±6.2%) than in the comparable subgroup of
saline controls (40.0±6.7%; p<0.05; Figure 6, left
panel). This apparent reduction in infarct size could
not be attributed to significant differences in either
area at risk (AR/LV, 17.7±2.7% vs. 13.5±2.2% in
control compared with treated high-flow subgroups;
/?=NS) or RMBF during occlusion (i.e., in the
midmyocardium, mean RMBF was 0.11 ±0.01 vs.
0.16±0.03 ml/min/g tissue in control compared with
treated subgroups; p=NS). In contrast, in the subgroup of dogs with lower than average collateral
flow during occlusion (RMBF in the ischemic midmyocardium <0.06 ml/min/g), infarct size was similar in control (57.4±9.8%) compared with treated
animals (48.6±5.9% of the area at risk; p=NS;
Figure 6, right panel).
Although these data were obtained from retrospective analysis, are based on an arbitrary subdivision of "higher than average" and "lower than
average" flows, and involved small sample sizes,
the results imply that the distribution of individual
flow values may be of importance in determination
of the efficacy free radical scavengers given at the
Electron Microscopic Analysis: Mean Semlquantitative Scores
Myocytes
Control (n=10)
SOD+CAT(/i = 10)
Endo
3.19±0.36
2.47±0.46
Microvasculature
Epi
0.84±0.38
1.71 ±0.50
Endo
0.41 ±0.14
0.10±0.08*
V < 0.05 vs. corresponding controls.
Endo, endocardium; Epi, epicardium; SOD, superoxide dismutase; CAT, catalase.
Epi
0.20±0.11
0.23±0.11
92
Circulation Research
Vol 64, No 1, January 1989
MICROVASCULAR DAMAGE
ALL DOGS
0.750
ENDO
0.500
0.250
0.000
1
EP1
*
I
m
CD CONTROLS
(n-10)
9
^
SOD + CATALASE
(n = 10)
Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017
FIGURE 4. Mean semiquantitative index ofiryury to the
endocardial and epicardial microvasculature for control
animals and those that received superoxide dismutase
(SOD)+catalase. *p<0.05 vs. the corresponding controls.
time of reperfusion. That is, possible differences in
distribution of flow values among the various studies may account for some of the apparent discrepancies: free radical scavenging agents may have
been more effective in studies in which a large
proportion of the dogs had moderately high collateral blood flow, while negative results may have
been obtained in studies in which a large proportion
of the animals were severely ischemic during coronary occlusion.
Ambrosio et al34 also concluded that collateral
blood flow during occlusion was a crucial determinant of the efficacy of SOD treatment. However, in
contrast to our retrospective observations, Ambrosio and coworkers found the hearts that showed the
greatest benefit from SOD treatment were those
with the lowest (as opposed to the highest) collateral flows during occlusion. This is sirniiar to the
apparent, flow-dependent effect of the calciumchannel blocking agent verapamil observed in a
limited subset of dogs that were severely ischemic
during coronary occlusion.36 In addition, Gallagher
et al31 found no reduction in infarct size with SOD or
catalase in a population of dogs with moderately high
values of RMBF during occlusion. The possible role
of collateral flow in influencing the efficacy of treatment with free radical scavenging agents is inconclusive: the effect and importance of "high" versus
"low" RMBF during occlusion must be clarified
from carefully designed prospective studies.
While several studies have examined the effects
of free radical scavenging agents on infarct size, few
have assessed the concomitant effect of the scavengers on contractile function of the viable subepicardial tissue salvaged by reperfusion. Considerable
evidence indicates that recovery of regional contractile function of myocardium stunned by a brief
(15-minute) period of transient occlusion is enhanced
significantly by pretreatment with SOD+catalase13-37-38 and other scavengers and antioxidants.39-41 The effect of these agents on function of
viable myocardium stunned by prolonged (s40
minute) periods of ischemia, however, has received
little attention to date.
As anticipated, all dogs in the present study were
severely dyskinetic during the 2 hours of coronary
occlusion. A slight, transient improvement in contractile function, similar to that described by Buda
et al42 was observed at 30 minutes postreperfusion
in both treated and control dogs. However, all dogs
again became dyskinetic in the final 2 hours of the
protocol. These data are in agreement with several
previous studies43-45 that demonstrate that myocardium salvaged by reperfusion after 2 hours of ischemia remains severely depressed for days following
reflow.
SOD+catalase, given at the time of reflow, had
no apparent beneficial effect on contractile function
of the viable subepicardium during the initial 4
hours of reperfusion. These data are similar to those
obtained by Puett et al,29 who subjected dogs to 90
minutes of regional ischemia and administered either
oxypurinol (an inhibitor of xanthine oxidase) or
saline at 60 minutes postocclusion: at 3 hours postreperfusion, percent radial shortening (assessed by
echocardiography) was comparable in both
oxypurinol-treated and saline control groups. At 24
hours postreperfusion, however, animals that had
received oxypurinol exhibited improved contractile
function when compared with saline controls.29
Although SOD+catalase and oxypurinol did not
have an acute beneficial effect on contractile function, results obtained by Puett et al suggest that
antioxidants and scavengers may accelerate recovery of regional contractile function when assessed
at or beyond 24 hours postreperfusion. In contrast,
Nejima et al35 found that SOD+catalase, given 5
minutes before reperfusion, did not improve regional
contractile function assessed 1 week postreperfusion in conscious dogs that underwent 90 minutes of
transient coronary occlusion. Thus, the long-term
effect of free radical scavenging agents and antioxidants on recovery of regional contractile function
following prolonged periods of transient ischemia
remains uncertain.
When reperfusion is carried out following prolonged (>90 minute) periods of coronary occlusion,
areas of no reflow,4647 low reflow,47 and microvascular injury17 are often observed within the area of
myocardial necrosis. Are these perfusion defects
mediated by oxygen-derived free radicals generated
at the time of reperfusion? The effect of free radical
scavenging agents on regional myocardial blood
flow and microvascular damage have received little
attention in in vivo models of transient, regional
myocardial ischemia.
As anticipated, control animals in the present
study exhibited 'low reflow' following reperfusion:
regional myocardial blood flow was restored to only
0.42-0.67 ml/min/g tissue in the previously ischemic LAD bed, or approximately 40-70% of values
measured in the normally perfused circumflex bed.
Przyklenk and Kloner
Reperfusion Ltfury by Free Radicals?
93
Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017
'-^to•u
1
m
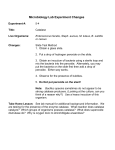
FIGURE 5. Top: Electron micrograph obtained from the previously ischemic endocardium of a saline control animal.
Both the myocytes (m) and the vascular endothelial cells (e) are severely damaged (approximate magnification, x.5,100).
Bottom: Electron micrograph obtained from the previously ischemic endocardium of an animal that received
SOD+catalase at the time ofreperfusion. The myocytes (m) are irreversibly injured, but the vascular endothelium (e) has
been preserved (approximate magnification, x3,100).
SOD+catalase administered at the time of reflow
enhanced postreperfiision blood flow to the endocardium and midmyocardium of the previously ischemic LAD bed. These data are comparable to the
increased values of coronary flow associated with
addition of free radical scavenging agents and antioxidants to cardioplegic solutions in models of
transient global ischemia.48 In addition, a trend
94
Circulation Research Vol 64, No 1, January 1989
HIGH COLLATERAL FLOW
LOW COLLATERAL FLOW
(Mldmyocordial RMBF > 0.06 m l / m i n / g tissue)
(Midmyocardlal RMBF < 0.06 m l / m i n / g tissue)
70
60-
I
504030
20
10
0
AN/AR (X)
CD CONTROLS
(n-5)
AN/LV (X)
AR/LV (X)
SOD + CATALASE
(n-4)
AN/AR (X)
CD CONTROLS
(n-5)
AN/LV (X)
AR/LV (X)
SOD + CATALASE
(n-8)
Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017
FIGURE 6. Left: Infarct size data for the subgroup of control and treated animals with higher than average collateral
blood flow during left anterior descending coronary artery (LAD) occlusion. *p<0.05 and **p<0.01 vs. the corresponding
control values. Right: Infarct size data for the subgroup of control and treated animals with lower than average collateral
blood flow during LAD occlusion. AN/AR, area of necrosis as a percentage of area at risk; AN/LV, area of necrosis as
a percentage of left ventricle; AR/LV, area at risk as a percentage of left ventricle.
toward a similar hyperemic effect was noted by
Ambrosio et al34 at 10 minutes postreperfusion in
animals treated with human recombinant SOD. In
both our study and that of Ambrosio et al,34 the
increase in flow postreperfusion occurred only in
regions of the myocardium that had been ischemic;
no hyperemic effect was observed in the normally
perfused tissue.
How can this improved blood flow in the previously ischemic myocardium of SOD+catalasetreated animals be explained? The improved values
of regional myocardial blood flow probably cannot
be attributed to vasodilation, as no effect was
observed within the normally perfused circumflex
bed. In addition, this increased flow does not appear
to be related to improved contractile function, as
segment shortening in the previously ischemic LAD
bed measured 2 hours postreperfusion did not differ
between control and treated groups.
Considerable evidence indicates that oxygenderived free radicals are responsible for vascular
injury in the cerebral circulation following brain
injury.49 Specifically, free radicals have been shown
to increase vascular permeability in the brain, leading to edema and tissue damage.50-51 Similar observations have, more recently, been made in isolated
heart preparations. For example, Jackson et al52
found an increase in vascular permeability and
vascular dysfunction in isolated rabbit hearts perfused with buffered solutions containing oxygenderived free radicals. Morphologic evidence of
vascular injury (by electron microscopy) was
observed both in isolated rabbit septae exposed to
free radical-generating solutions" and in isolated
septal preparations subjected to 1 hour of ischemia
followed by reperfusion.53 In each case, the addition of free radical scavenging agents (dimethyl
sulfoxide, SOD, and catalase) to the perfusate
provided significant protection against this free
radical-mediated vascular injury. 115253
Electron microscopic analysis of biopsy samples
obtained in the present study clearly indicate that
the morphology of the endocardial vascular endothelium was preserved in animals that received
SOD+catalase at the time of reflow. This would
suggest that oxygen-derived free radicals generated
upon reperfusion may play a role in mediating
microvascular injury in this model. Because both
low reflow and vascular injury were completely
ablated in the endocardium of dogs treated with
SOD+catalase, it appears likely that the enhanced
flow postreperfusion in these animals could be
attributed, at least in part, to the preservation of the
vascular endothelium by the free radical scavenging
agents.
These data may further suggest that the vascular
endothelium, thought to be rich in xanthine
oxidase,54 may represent a major source of oxygenderived free radicals in this canine model of prolonged coronary occlusion followed by reperfusion.
However, free radicals may also be generated within
the previously ischemic myocytes by either the
xanthine oxidase reaction8 or by other enzymatic
pathways known to produce reactive oxygen
species.55 In addition, recent evidence indicates
that polymorphonuclear neutrophils, known to rapidly infiltrate previously ischemic myocardium following reperfusion, also represent a significant
source of oxygen-derived free radicals in the canine
model of prolonged but transient ischemia.56 The
precise source(s) or mechanism(s) of free radical
production in the present study is uncertain.
In summary, we observed that SOD+catalase,
initiated at the time of reperfusion, did not reduce
infarct size produced by 2 hours of coronary artery
occlusion and 4 hours of reflow in the anesthetized,
open-chest dog. Furthermore, treatment with these
Przyklenk and Kloner
potent scavenging agents did not attenuate postischemic contractile dysfunction of the viable, previously ischemic subepicardium. However,
SOD+catalase given 1 minute before reperfusion
effectively ablated both microvascular damage and
the low reflow phenomenon in the endocardium and
midmyocardium of the previously ischemic LAD
bed. Thus, microvascular injury and low reflow
after prolonged but transient coronary occlusion in
the canine model may be mediated by oxygen free
radicals generated at the time of reperfusion.
Acknowledgment
The authors gratefully acknowledge the expert
technical assistance of Sara Noorily, E.M. Technologist (E.M.S.A. Certified), Department of Pathology, Harper-Grace Hospital, Detroit, Michigan.
Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017
References
1. Reimer KA, Lowe JE, Rasmussen MM, Jennings RB: The
"wavefront phenomenon" of ischemic cell death. I. Myocardial infarct size vs. duration of occlusion in dogs. Circulation 1977^6:786-794
2. Reimer KA, Jennings RB: The "wavefront phenomenon" of
myocardial ischemic cell death. II. Transmural progression
of necrosis within the framework of ischemic bed size
(myocardium at risk) and collateral flow. Lab Invest 1979;
40:633-644
3. Przyklenk K, Vivaldi MT, Schoen FJ, Arnold JMO, Kloner
RA: Salvage of ischemic myocardium by reperfusion: Importance of collateral bloodflowand myocardial oxygen demand
during occlusion. Cardiovasc Res 1986^0:403-414
4. Patel B, KJoner RA: Analysis of reported randomized trials
for streptokinase therapy for acute myocardial infarction in
the 1980's. Am J Cardiol 1987^9:501-504
5. DeWood MA, Spores J, Berg R Jr, Kendall RW, Grunwald
RP, Selinger SL, Hensely GR, Sutherland KI, Shields JP:
Acute myocardial infarction: A decade of experience with
surgical reperfusion in 701 patients. Circulation 1983;
68(suppl II):II-8-II-16
6. Braunwald E: The aggressive treatment of acute myocardial
infarction. Circulation 1985;71:1087-1092
7. Braunwald E, Kloner RA: Myocardial reperfusion: A doubleedged sword? J Clin Invest I985;76:1713-1719
8. McCord JM: Oxygen-derived free radicals in postischemic
tissue iryury. N EnglJ Med 1985;312:159-163
9. Kramer JH, Arroyo CM, Dickens BF, Weglicki WB: Spintrapping evidence that graded myocardial ischemia alters
postischemic superoxide production. Free Radical Biol Med
I987;3:153-159
10. Garlick PB, Davies MJ, Hearse DJ, Slater TF: Direct
detection of free radicals in reperfused rat heart using
electron spin resonance spectroscopy. Circ Res 1987;
61:757-760
11. Burton KP, McCord JM, Ghai G: Myocardial alterations due
to free radical generation. Am J Physiol 1984;246:H776-H783
12. Lange R, Ware J, Kloner RA: Absence of a cumulative
deterioration of regional function during three repeated 5 or
15 minute coronary occlusions. Circulation 1984;69:400-408
13. Przyklenk K, Kloner RA: Superoxide dismutase plus catalase improve contractile function in the canine model of the
'stunned myocardium'. Circ Res 1986^8:148-156
14. Fishbein MC, Meerbaum S, Rit J, Lando U, Kanmatsuse K,
Mercier JC, Corday E, Ganz W: Early phase acute myocardial infarct size quantification: Validation of the triphenyltetrazolium chloride tissue enzyme staining technique. Am
Heart J 1981 ;101:593-600
15. Vivaldi MT, Kloner RA, Schoen FJ: Triphenyltetrazolium
staining of irreversible ischemic injury following coronary
artery occlusion in rats. Am J Pathol 1985;121:522-530
Reperfusion Iqjury by Free Radicals?
95
16. Domenech RJ, Hoffman JE, Noble MM, Saunders KB,
Henson RJ, Subyanto S: Total and regional coronary blood
flow measured by radioactive microspheres in conscious and
anesthetized dogs. Circ Res 1969;25:581-596
17. Kloner RA, Rude RE, Carlson NC, Maroko PR, DeBoer
LWV, Braunwald E: Ultrastructural evidence of microvascular damage and myocardial cell injury after coronary
artery occlusion: Which comes first? Circulation 1980;
62:945-952
18. Wallenstein S, ZuckerCL, Fleiss JL: Some statistical methods useful in circulation research. Circ Res 1980;47:l-9
19. Chambers DE, Parks DA, Patterson G, Roy R, McCord JM,
Yoshida S, Parmley LF, Downey JM: Xanthine oxidase as a
source of free radical damage in myocardial ischemia. J Mol
Cell Cardiol 1985;17:145-152
20. Werns SW, Shea MJ, Mitsos SE, Dysko RC, Fantone JC,
Shork MA, Abrams GD, Pitt B, Lucchesi BR: Reduction of
the size of infarction by allopurinol in the ischemicreperfused canine heart. Circulation 1986;73:518-524
21. Wems SW, Grum CM, Ventura A, Lucchesi BR: Effects of
allopurinol or oxypurinol on myocardial reperfusion injury
(abstract). Circulation 1987;76(suppl IV):IV-197
22. Jolly SR, Kane WJ, Bailie MB, Abrams GD, Lucchesi BR:
Canine myocardial reperfusion injury: Its reduction by the
combined administration of superoxide dismutase and catalase. Circ Res 1984^4:277-285
23. Werns SW, Shea MJ, Driscoll EM, Cohen C, Abrams GD,
Pitt B, Lucchesi BR: The independent effects of oxygen
radical scavengers on canine infarct size: Reduction by
superoxide dismutase but not by catalase. Circ Res 1986;
56:895-898
24. Arroyo CM, Kramer J, Lieboff R, Mergner G, Dickens B,
Weglicki W: Detection by electron spin resonance (ESR)
spectroscopy with spin trapping of oxygen- and carboncentered free radicals in ischemic canine myocardium
(abstract). Fed Proc 1987;46:4IO
25. Kramer JA, Arroyo CM, Weglicki WB: Direct observation
of free radical generation in ischemic hearts (abstract).
Circulation 1987;76(suppl IV):IV-199
26. Akizuki S, Yoshida S, Chambers DE, Eddy LJ, Parmley LF,
Yellon DL, Downey JM: Infarct size limitation by the
xanthine oxidase inhibitor allopurinol in closed-chest dogs
with small infarcts. Cardiovasc Res 1985;19:686-692
27. Przyklenk K, Kloner RA: Effect of oxygen-derived free
radical scavengers on infarct size following six hours of
permanent coronary artery occlusion: Salvage or delay of
myocyte necrosis? Basic Res Cardiol 1987;82:146-158
28. Reimer KA, Jennings RB: Failure of xanthine oxidase inhibitor allopurinol to limit infarct size after ischemia and reperfusion in dogs. Circulation 1985;71:1069-1075
29. Puett DW, Forman MB, Cates CU, Wilson BH, Hande KR,
Friesinger GC, Virmain R: Oxypurinol limits myocardial
stunning but does not reduce infarct size after reperfusion.
Circulation 1987;76:678-686
30. Kinsman JM, Murry CE, Richard VJ, Jennings RB, Reimer
KA: Oxypurinol does not limit infarct size in a canine model
of 40 minutes of ischemia with reperfusion (abstract). Circulation 1987;76(suppl IV):IV-197
31. Gallagher KP, Buda AJ, Pace D, Gerren RA, Schlafer M:
Failure of superoxide dismutase and catalase to alter infarct
size in conscious dogs after 3 hours of occlusion followed by
reperfusion. Circulation 1986;73:1065-1076
32. Uraizee A, Reimer KA, Murry CE, Jennings RB: Failure of
superoxide dismutase to limit size of myocardial infarction
after 40 minutes of ischemia and 4 days of reperfusion in
dogs. Circulation 1987;75:1237-1248
33. Richard VJ, Murry CE, Jennings RB, Reimer KA: Superoxide dismutase and catalase do not limit infarct size after 90
minutes of ischemia and 4 days of reperfusion in dogs
(abstract). Circulation 1987;76(suppl IV):IV-199
34. Ambrosio G, Becker LC, Hutchins GM, Weisman HF,
Weisfeldt ML: Reduction in experimental infarct size by
recombinant human superoxide dismutase: Insights into the
96
35.
36.
37.
38.
39.
Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017
40.
41.
42.
43.
44.
45.
Circulation Research
Vol 64, No 1, January 1989
pathophysiology of repcrfusion injury. Circulation 1986;
74:1424-1433
Nejima J, Canficld DR, Manders WT, Knigbt DR, Cohen
MV, Fallon JT, Vatner SF: Failure of supcroxide dismutase
and catalase to alter size of infarct and functional recovery in
conscious dogs with reperfusion (abstract). Circulation 1987;
76(suppl IV):IV-198
Reimer KA, Jennings RB, Cobb FR, Murdock RH, Greenfield JC Jr, Becker LC, Bulkley BH, Hutchins GM, Schwartz
RP, Bailey KR, Passamani ER: Animal models for protecting ischemic myocardium: Results of the NHLBI cooperative study. Comparison of unconscious and conscious dog
models. Circ Res 1985^6:651-665
Myers ML, BoUi R, Lekich RF, Hartley CJ, Roberts R:
Enhancement of recovery of myocardial function by oxygen
free radical scavengers after reversible regional ischemia.
Circulation 1985,72:915-921
Gross GJ, Farber NE, Hardman HF, Warltier DC: Beneficial actions of superoxide dismutase and catalase in stunned
myocardium of dogs. Am J Physiol 1986;250:H372-H377
Myers ML, Bolli R, Lekich RF, Hartley a , Roberts R:
N-2-mercaptopropionylglycine improves recovery of myocardial function following reversible regional ischemia. J Am
Coll Cardiol 1986;8:1161-1168
Charlat ML, O'Neill PG, Egan JM, Abemathy DR, Michael
LH, Myers ML, Roberts R, Bolli R: Evidence for a pathogenic role of xanthine oxidase in the "stunned" myocardium. Am J Physiol 1987;252:H566-H577
Bolli R, Zhu WX, Hartley CJ, Michael LH, Repine JE, Hess
ML, Kukreja RC, Roberts R: Attenuation of dysfunction in
the postischemic 'stunned' myocardium by dimethylthiourea. Circulation 1987;76:458-468
Buda AJ, Zotz RJ, Pace DP, Krause LC, Turla M: Immediate rebound followed by deterioration of regional left ventricular function with coronary reperfusion. J Am Coll
Cardiol 1986;8:333-341
Ellis SG, Henschke CI, Sandor T, Wynne J, Braunwald E,
KJoner RA: Time course of functional and biochemical
recovery of myocardium salvaged by reperfusion. J Am Coll
Cardiol 1983;3:1047-1055
Lavallee M, Cox D, Patrick TA, Vatner SF: Salvage of
myocardial function by coronary artery reperfusion 1,2 and
3 hours after occlusion in conscious dogs. Circ Res 1983;
53:235-247
Arnold JMO, Antman EM, Przyklenk K, Braunwald E,
Sandor T, Vivaldi MT, Schoen FJ, Kloner RA: Differential
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
effects of reperfusion on incidence of ventricular arrhythmias and recovery of ventricular function at 4 days following
coronary occlusion. Am Heart J 1987;! 13:1055-1065
Kloner RA, Ganote CE, Jennings RB: The "no reflow"
phenomenon following temporary coronary occlusion in the
dog. J Clin Invest 1974^4:1496-1508
Kloner RA, Alker KJ: Effect of streptokinase on intramyocardial hemorrhage, infarct size, and the no-reflow phenomenon during coronary reperfusion. Circulation 1984;
70:513-521
Schlafer M, Kane PF, Kirsh MM: Superoxide dismutase
plus catalase enhances the efficacy of hypothennic cardioplegia to protect the globally ischemic, reperfused heart. J
Thorac Cardiovasc Surg 1982,83:830-839
Hammond B, Kontos HA, Hess ML: Oxygen radicals in the
adult respiratory distress syndrome, in myocardial ischemia
and reperfusion injury, and in cerebral vascular damage.
Can J Physiol Pharmacol 1985;63:173-187
Del Maestro RF, Bjork J, Arfors KE: Increase in microvascular permeability induced by enzymatically generated free
radicals. I. In vivo study. Microvasc Res 1981^2:239-254
Del Maestro RF, Bjork J, Arfors KE: Increase in microvascular permeability induced by enzymatically generated free
radicals. II. Role of superoxide anion radical, hydrogen
peroxide, and hydroxyl radical. Microvasc Res 1981;
22:255-270
Jackson CV, Mickelson JK, Pope TK, Rao PS, Lucchesi
BR: Oj free radical-mediated myocardial and vascular dysfunction. Am J Physiol 1986;251:H1225-H1231
Burton KP: Superoxide dismutase enhances recovery following myocardial ischemia. Am J Physiol 1985 ;248:
H637-H643
Jaresch ED, Bruder G, Held HW: Significance of xanthine
oxidase in capillary endothelial cell. Ada Physiol Scand
1986;548(suppl):39-46
Freeman BA, Crapo JD: Biology of disease: Free radicals
and tissue injury. Lab Invest 1982;47:412-426
Romson JL, Hook BG, Kunkel SL, Abrams GD, Shork A,
Lucchesi BR: Reduction of the extent of ischemic myocardial injury by neutrophil depletion in the dog. Circulation
1983;67:1016-1023
KEY WORDS • free radicals • superoxide dismutase •
catalase • reperfusion • myocardial blood flow • regional
function • coronary microvasculature
"Reperfusion injury" by oxygen-derived free radicals? Effect of superoxide dismutase plus
catalase, given at the time of reperfusion, on myocardial infarct size, contractile function,
coronary microvasculature, and regional myocardial blood flow.
K Przyklenk and R A Kloner
Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017
Circ Res. 1989;64:86-96
doi: 10.1161/01.RES.64.1.86
Circulation Research is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1989 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7330. Online ISSN: 1524-4571
The online version of this article, along with updated information and services, is located on the
World Wide Web at:
http://circres.ahajournals.org/content/64/1/86
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in
Circulation Research can be obtained via RightsLink, a service of the Copyright Clearance Center, not the
Editorial Office. Once the online version of the published article for which permission is being requested is
located, click Request Permissions in the middle column of the Web page under Services. Further information
about this process is available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation Research is online at:
http://circres.ahajournals.org//subscriptions/