Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
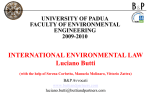
OUTCOMES IN PRACTICE How to Implement the “Let Me Decide” Advance Health and Personal Care Directive Program D.W. Molloy, MRCP, FRCP(C), Rosalie Russo, Angela Stiller, and M.J. O’Donnell A dvance directives extend patient autonomy and allow individuals to maintain control of their own health care after they can no longer speak for themselves. Despite these benefits, advance directives are being underutilized in most health care sectors [1–3]. Results from studies evaluating advance directive interventions have been variable [4–10]. The highest levels of advance directive completion have been associated with systematic implementation [11–13]. In 1988, we developed the Let Me Decide (LMD) advance directive program [14]. The LMD directive has instructional and proxy components [15] and includes a chart on which patients indicate their health care choices (Figure). We have evaluated the systematic implementation of the program in nursing homes [12,16] and in the community [13,17]. The first study [12] was a randomized controlled trial that examined the effect of program implementation in nursing homes on patient and family satisfaction. Six nursing homes were pair-matched on key characteristics, and 1 home per pair was randomized to the intervention. Among the intervention homes, 49% of competent residents and 78% of families of incompetent residents completed directives. There was no difference in satisfaction between intervention and control homes. The intervention homes reported fewer hospitalizations per resident and less resource use while the proportion of deaths in the intervention and control homes were similar. The second study [13] evaluated the feasibility and effectiveness of implementing the program among communitydwelling veterans. Eighty-two (71%) of 116 veterans expressed interest in receiving information about the program and 67 (82%) of these were educated. Forty-two (63%) of the 67 educated veterans completed directives. Veterans who were educated about directives reported that the education process was beneficial and should be offered to other veterans. We have found consistent support from residents, families, and health care workers for the LMD program [12,14,16,17]. In this article, we describe our systematic approach to the implemention of the LMD program in long-term care facilities. Vol. 7, No. 9 Laying the Groundwork Identify Barriers A number of barriers to directive implementation have been identified. Patients can have misconceptions and fears about directives [3,18,19] and report that physicians fail to initiate discussions or promote them [20]. Health care workers cite lack of knowledge, education, and experience with using advance directives [11,14,21,22] and lack of time for discussion of directives with patients and their families [23]. Others feel that directives are vague or too complicated [24]. We have developed a tool that measures barriers to implementing advance directives in different care sectors. Our questionnaire lists 30 potential barriers (eg, time contraints, patients unable to understand directive concepts, conflicting attitudes or opinions among patients, families, and other health care workers) and asks respondents to indicate which barriers they encounter and to rate those they encounter on a scale from least important to most important. By identifying barriers, institutions can adapt their educational programs and customize them to meet the specific needs of patients and staff. Identify Staff Educational Needs When advance directives are introduced in long-term care settings, the majority of residents choose palliative care for irreversible conditions. Most die in the long-term care institution rather than in a hospital, increasing the palliative care burden on these institutions. We employ a questionnaire that assesses for health care workers’ educational needs in areas such as stress management, management of pain, and management of the psychological impact of death on patients and families. Like the barriers questionnaire, this instrument D.W. Molloy, MRCP, FRCP(C), Professor of Medicine, Division of Geriatric Medicine, McMaster University, Director, Geriatric Research Group, Henderson Hospital, Hamilton, Ontario, Canada; Rosalie Russo, Senior Research Coordinator, Geriatric Research Group, McMaster University; Angela Stiller, Research Coordinator, Geriatric Research Group, McMaster University; and M.J. O’Donnell, Clinical Fellow, Geriatric Research Group, McMaster University. JCOM September 2000 41 LET ME DECIDE If my condition is Reversible/Acceptable Life-threatening illness Cardiac arrest Palliative Limited Surgical Intensive No CPR CPR Date Signature If my condition is Irreversible/Intolerable Feeding Life-threatening illness Cardiac arrest Basic supplemental Intravenous Tube Palliative Limited Surgical Intensive No CPR CPR Power of Attorney Signature(s) Feeding Basic supplemental Intravenous Tube Physician Signature Date of next review should be once a year, after an illness, or if any change in health Date Signature Power of Attorney Signature(s) Physician Signature Date Signature Power of Attorney Signature(s) Physician Signature Figure. Personal health care chart from Let Me Decide directive. (Reprinted with permission from Molloy DW. Let me decide. Troy, ON: Newgrange Press; 1999.) is helpful for developing and adapting educational programs for health care workers. Establish Policies Institutions should have policies in place that state when and how to introduce directives to residents, ensuring that a standardized approach is maintained. Guidelines and procedures for charting, contacting individuals about directives, contacting substitute decision makers, and choosing different treatment protocols depending on the choices expressed in the directive should be outlined. Procedures should clearly state how to follow directives, what each level of care means, and how to interpret personal statements. A study in a community setting [25] found that nursing staff had positive attitudes toward patient autonomy and advance directives, but had difficulty finding time to discuss directives with patients and their families, let alone educate them and assist in their completion. Since time constraints is one of the most common reported barriers to directive implementation, administrators need to examine issues of workload when developing new policies for advance directives. Appoint and Train Facilitator Implementing the advance directive program requires a well-trained and skilled health care facilitator. In the past, 42 JCOM September 2000 nurses have been trained for this role in a variety of settings; however, staff in other health care–related fields could also be trained (eg, social worker, program coordinator). Ideally, the facilitator should be on staff at the institution and be familiar with other staff, residents and families, residents’ council, and the administrative structure of the institution. As the facilitator’s skill and knowledge are paramount to the successful completion of the directive program, facilitators attend specialized training workshops. A 2-day “train the trainer” workshop for facilitators provides an explicit standardized approach to educating hospital, nursing home, community health service staff, residents, and families. Facilitators learn how to measure competency, complete directives, and negotiate and deal with family conflict. How to effectively disseminate information about the program in their institution (eg, mailings, open information sessions) is also discussed. Training workshops provide background material on advance directives research, ethical issues, current legislation, and policy development. Educate Health Care Workers Facilitators provide standardized education for health care staff in the long-term care facility, the receiving hospitals, and community health care services (eg, nursing staff, medical staff, emergency staff, social workers, palliative care teams, Vol. 7, No. 9 OUTCOMES IN PRACTICE in-service educators, dietitians, occupational/physiotherapists, health records, admitting, community health care representatives, staff on clinical teaching units). During 1-hour presentations, the facilitator describes the 5 sections of the directive, explains how to interpret treatment choices, and discusses the impact of the directive on staff. Additional education is provided to hospital emergency department staff and in-house physicians at the long-term care facilities. Regular refresher sessions maintain awareness among previously trained staff and are mandatory for the orientation of new staff. Background material, including videos and books about the directive program, are made available to staff through library resources. In long-term care facilities, educational sessions are provided for the residents’ council, which helps cultivate a supportive environment for directive implementation. Implementing the Directive Once the facility establishes policies and educates the staff, directive implementation can begin. Several steps are involved. Step 1: Screen for Cognitive Impairment and Other Deficits As the first step in implementing the directive, facilitators screen individuals for cognitive impairment or other deficits using the Standardized Mini-Mental State Exam [26,27], a short screening measure of cognitive function. Patients who score 20 or greater are 95% likely to be able to fully understand or appreciate the consequences of the choices offered as part of the advance directive [28]. Five percent of people who score less than 20 may be competent to complete a directive. A cut-off of 15 is used to ensure 100% of people competent to complete a directive are given the opportunity to be educated and complete a directive [12]. Residents who score 15 or above receive education about directives (Step 2, below). In the cases where people score less than 15, the family is approached to determine their interest in completing an “expression of wishes for future care for their incapable family member.” This document is the same one completed by competent residents but serves only to provide a standardized format for documenting the treatment they believe patients would want in particular situations. Mini-mental state exam scores can be affected by depression, which can alter the ability to comprehend, make appropriate decisions, and appreciate consequences. Residents with depression are more likely to refuse life-sustaining medical treatment [29,30]. If depression is suspected, patients are screened with the Geriatric Depression Scale [31]. If the scale score suggests depression, the facilitator notifies the responsible physician and terminates the educational process until further notice. Vol. 7, No. 9 Table 1. Excerpt from Introduction to Let Me Decide Directive In this directive I am stating my wishes for my health and personal care should the time ever come when I am not able to communicate because of illness or injury. This directive should never be used if I am able to decide for myself. It must never be substituted for my judgment if I can make these decisions. If the time comes when I am unable to make these decisions, I would like this directive to be followed and respected. Please do everything necessary to keep me comfortable and free of pain. Even though I may have indicated that I do not want certain treatment, I recognize that these may be necessary to keep me comfortable. I understand that my choices may be overridden if the treatment is necessary to maintain comfort. I have thought about and discussed my decision with my family doctor. In an emergency, please contact my power(s) of attorney/substitute decision maker(s) or my family doctor listed below. If these people are not available, then please do as I have requested in this directive. Reprinted with permission from Molloy DW. Let me decide. Troy, ON: Newgrange Press; 1999. Step 2: Educate Facilitators inform residents individually that a new advance directive program is being implemented in the facility and that the residents have an opportunity to be educated about directives and to complete one. Residents are invited to review an informational booklet and to view three 20-minute educational videos prior to educational sessions. In educating residents, facilitators use individualized communication strategies to ensure that each patient’s needs are met, taking the necessary time to provide explanation and hold discussion. Language is kept simple, and no more than 1 idea is communicated at a time. Facilitators consider factors such as educational level, emotional state (grief, depression, or anxiety), and physical condition (blindness, deafness) of the patient so that they employ the most appropriate style and format of education for the sessions. Sessions are held in the early morning or afternoon in quiet, private areas in the facility or the patient’s own room. Educational material is available in several languages. Overview of directive. As part of educating residents and their designated substitutes, facilitators provide an overview of the 5 sections of the LMD directive. The Introduction section (Table 1) states the reason why the directive is being completed. Signing the directive revokes any previous documents, establishes this document as the latest expression of wishes, and names the substitutes (power of attorney, proxy, mandatory). The facilitator makes sure that the person understands what is stated in this section, and the importance of the substitute decision makers’ role is discussed. Substitutes need to understand the person’s goals, values, and JCOM September 2000 43 LET ME DECIDE Table 2. Definitions of Terms Used in Let Me Decide Directive The directive will only be published in this article and never excerpted, copied, sold, reproduced or used again outside of the article in this edition of the journal. The article may not be sold with the directive in it either. Reprinted with permission from Molloy DW. Let me decide. Troy, ON: Newgrange Press; 1999. choices, and need to be able to make these known to others, if and when the need arises. Next, facilitators explain the terms used in the personal health care chart, on which the residents indicate the type of care they would want if their condition was “reversible/ acceptable” and the type of care they would want if their condition was “irreversible/intolerable.” For both conditions, residents are asked to choose the type of care they would want in case of life-threatening illness (palliative, limited, surgical, or intensive) or in case of cardiac arrest (CPR or no CPR) and type of feeding they would want (basic, supplemental, intravenous, or tube). The definitions of these terms are listed in the Definition section of the directive (Table 2). Facilitators explain these terms using many practical examples. For example, facilitators explain that surgery might still be given if palliative care is requested: “If your hip was broken and you had severe pain, surgery might be the only way to relieve your pain.” 44 JCOM September 2000 Residents are reminded that they will be able to change their choices and update their directives as often as they like; this usually occurs about once a year or if there is a change in their health. Facilitators show the place provided on the directive for the updated information and explain the process. The facilitator also explains the Signatures section, which in addition to the signatures contains the names, addresses, and telephone numbers of the family doctor, substitutes, and witnesses. Development of personal statement. The LMD directive contains an area for the resident to describe in his/her own words what for them constitutes an unacceptable level of function. The facilitator starts by reading the introductory phrase, “I consider an irreversible/intolerable condition to be any condition…” and explains that the resident can describe, in their own words, the level of disability they would consider unacceptable or intolerable. The personal Vol. 7, No. 9 OUTCOMES IN PRACTICE statement usually describes an irreversible condition in terms of function (eg, “loss of ability to communicate or perform activities of daily living such as dressing, washing, recognizing family and friends”). To help residents formulate their personal statement, the facilitators asks, “Consider what treatment you would want if you were in good health with an acceptable quality of life and suddenly you became ill with a life-threatening illness, such as pneumonia or a bleeding ulcer, that could be completely cured without any lasting disability. What treatment would you want in this situation?” They then ask, “Consider what treatment choices you would make if you suffered a severe brain injury and were in an irreversible coma, in a persistent vegetative state, unconscious, unable to communicate or swallow, with no hope of recovery. Would you want different treatment options than if you were healthy and had a good quality of life?” People are asked to complete phrases such as “As long as I can… , I would accept this level of function and quality of life. But when I can’t do… , then I would consider this an unacceptable quality of life.” Facilitators ask, “From what point on would you want to be kept comfortable and not want technology to prolong your life?” Facilitators emphasize that different people have different values and goals in life and are prepared to accept different disabilities. They use the following example: Consider Beethoven and Picasso. Beethoven went deaf, a tragic loss for a great composer. Hearing may have been the most important sense for him. If he had gone blind, it would have been less disabling. On the other hand, if Picasso had gone blind, it would have been devastating. The facilitator repeats back what the resident has said, offering examples of the consequences of their choices to make sure their choices are consistent with their wishes and to ensure that they understand and appreciate these consequences. Facilitators document the content and outcomes of educational sessions in the medical charts. Concerns about peoples’ capacity to complete directives, specific strategies used to explore and validate these concerns, names of the substitute decision makers, responses to educational sessions, conflicts, and follow-up plans such as referral to social workers, clergy, or doctors are documented. Step 3: Assess Capacity to Complete Directive After residents are educated, facilitators use the Screening Instrument to Assess Capacity to Complete an Advance Directive (SIACAD) to assess capacity to complete the LMD directive [28]. The SIACAD is a 24-item questionnaire that assesses understanding of the purpose of the directive, meaning of terms used in the directive, and consequences of choices Vol. 7, No. 9 Table 3. Questions Used to Assess Competency to Complete an Advance Directive Does this advance directive deal with people’s property? Does this advance directive deal with people’s health? Do proxies make decisions for people who are clear headed and able to communicate? Do proxies make decisions for people when they are in a coma? Is it important that proxies understand the person’s health care wishes? Do people usually recover completely from an irreversible illness? Is Alzheimer’s disease usually considered a reversible illness? Do people usually recover completely from a reversible illness? Is pneumonia usually considered a reversible illness? Can people make different treatment choices for reversible and irreversible conditions? Do all four levels of care (for life-threatening illness) provide the same kind of treatment? Does palliative care usually include having surgery and being hooked up to a breathing machine? Do people who choose palliative care usually get transferred to the intensive care unit? Does limited care include palliative care? Does intensive care mean that everything possible will be done to treat a person? Does intensive care mean comfort measures only? Does basic feeding mean that people will be fed by tubes? Does supplemental feeding include high energy supplements or extra vitamins? Does supplemental feeding usually include nasogastric tube? Is cardiopulmonary resuscitation (CPR) used to restore someone’s breathing or heartbeat? Does “No CPR” mean that a person will be resuscitated if their heart stops? If people choose “No CPR,” will their heart and breathing eventually stop? Can people make a personal statement (in their directive) describing what they consider an irreversible condition to be? Do people who say “No blood transfusion” in their directive receive a blood transfusion? Reprinted with permission from Molloy DW, Silberfeld M, Darzins P, Guyatt GH, Singer PA, Rush B, et al. Measuring capacity to complete an advance directive. J Am Geriatr Soc 1996;44:660–4. that can be made in the directive (Table 3). If the score indicates the patient is incapable, next of kin are approached to help develop a care plan. If the score indicates borderline capacity, conditions that could influence cognition (eg, hearing loss, delirium) are examined and treated. The facilitator reeducates, particularly focusing on the areas where the patient answered incorrectly, and then reassesses capacity. If patients are still deemed incapable after reeducation and readministration of the SIACAD, facilitators approach the next of kin to help develop a care plan consistent with the incapable person’s prior JCOM September 2000 45 LET ME DECIDE expressed wishes and values. If their wishes and values are unknown, decisions are made that are consistent with their best interests. Step 4: Complete the Directive Once the patient is deemed competent, choices are reviewed and documented on the directive and the directive is signed by the patient, substitute decision makers, and physician. Managing the Directive A systematic approach to managing directives ensures consistency and quick retrieval of medical information from residents’ charts. Original directives are kept in the medical charts and marked “Original copy—do not remove from chart.” Charts containing a directive are flagged with a brightly colored sticker on the outside of the chart. Treatment wishes for reversible and irreversible conditions for lifethreatening illness, feeding options, and cardiopulmonary resuscitation are recorded in the doctor’s progress notes. All directives are marked with the message “To attending physician: please transcribe this directive on the doctor’s orders.” Notes on the doctor’s orders can also refer to the the directive (eg, “See advance directive—please follow patient’s choices expressed there”). Additional copies of directives are kept at the front of the chart and sent with transfer forms when residents are moved to hospitals, clinics, or other institutions. When a patient is transferred to hospital, the transfer records should indicate that the patient has been transferred and that a copy of the directive has been forwarded with them. If an individual chooses not to complete a directive, a description of the discussions, reasons for refusal, and follow-up is also documented. Directive Review Facilitators review directives with residents annually or after serious medical events, changes in health status, or any time changes in directives are requested by the resident. Changes (or “no changes”) are recorded on the original directive. If major changes are requested, such as significant additions or deletions to personal statements or changes to the personal health care chart, it might be simpler to fill out new directives and obtain all required signatures using the original protocol. Whenever changes are made to directives, physicians review them, substitute decision makers re-sign them, and copies of the signed documents are provided to all parties. Old copies are discarded from medical charts. When competent people with a completed directive become incompetent or experience a deterioration in their level of function that meets their own definition of an “irreversible” condition with an intolerable quality of life, this is noted on the directive and medical chart. The updated directive states that 46 JCOM September 2000 this person is now incompetent, in an irreversible condition with an unacceptable quality of life, based on their own personal statements. This change is reviewed by substitutes. The wishes of the person while competent are honored and cannot be overridden by substitute decision makers. Some facilities have computerized systems for storing patient information and would likely be adaptable to include directive review dates. Routine lists can provide upto-date information for scheduling these appointments. For those facilities where manual tracking is more appropriate, the day book or calendar system works best. Program Evaluation The advance directive program is evaluated using tools that measure residents’ and families’ satisfaction with health care received and their involvement in the decision making process [32]. Reassessment of barriers to advance directive use and learning needs for palliative care [33] over time help to refine educational programs, modify specific strategies for improving the implementation of the program, and introduce new options for customizing advance directives and policies. Cost of Program For our program, the facilitator requires a commitment of 100% of a standard work shift for 6 to 8 months for nursing homes with 160 to 250 residents. After initial implementation, facilitators usually work one-quarter time to maintain the program—half a day in smaller homes (less than 200 residents) and a full day in larger homes (200 or more residents). The amount of time required to maintain the program will vary slightly depending on the admission rate. The approximate estimated cost to provide education and complete the directive is $113 CAD per resident. More residents are deciding to stay in the nursing home at the end of life instead of transferring to a hospital. Extra funding will be necessary to support their wishes and provide quality care to residents who request palliation in nursing homes. Conclusion Successful implementation of directive programs requires the integration of policies, education, directive completion and capacity assessment strategies. A systematic approach by trained and skilled facilitators is essential to successfully implement programs. Comprehensive directives and reliable programs ensure that competent people in long-term, acute care facilities and in the community have their freedom protected and maintain the ability to exercise their rights. Authors’ address: Geriatric Research Group, Henderson Hospital, 711 Concession St., Hamilton, ON L8V1CM, Canada, [email protected]. Vol. 7, No. 9 OUTCOMES IN PRACTICE References 1. Murphy CP, Sweeney MA, Chiriboga D. An educational intervention for advance directives. J Prof Nurs 2000;16:21–30. 2. Crego PJ. When, how, and why of advance directives: tools for the cardiovascular nurse. Prog Cardiovasc Nurs 1999;14:92–6. 3. Tonelli MR. Pulling the plug on living wills : A critical analysis of advance directives. Chest 1996;110:816–22. 4. Miles SH, Koepp R, Weber EP. Advance end-of-life treatment planning. A research review. Arch Intern Med 1996;156:1062–8. 5. Cugliari AM, Miller T, Sobal J. Factors promoting completion of advance directives in the hospital. Arch Intern Med 1995;155:1893–8. 6. Rubin SM, Strull WM, Fialkow MF, Weiss SJ, Lo B. Increasing the completion of the durable power of attorney for health care. A randomized, controlled trial. JAMA 1994;271:209–12. 7. High DM. Advance directives and the elderly: a study of intervention strategies to increase use. Gerontologist 1993;33342–9. 8. Siegert EA, Clipp EC, Mulhausen P, Kochersberger G. Impact of advance directive videotape on patient comprehension and treatment preferences. Arch Fam Med 1996;5:207–12. 9. Orlander JD. Use of advance directives by health care workers and their families. South Med J 1999;92:481–4. 10. Landry FJ, Kroenke K, Lucas C, Reeder J. Increasing the use of advance directives in medical outpatients. J Gen Intern Med 1997;12:412–5. 11. Hammes BJ, Rooney BL. Death and end-of-life planning in one midwestern community. Arch Intern Med 1998;158:383–90. 12. Molloy DW, Guyatt GH, Russo R, Goeree R, O’Brien BJ, Bédard M, et al. Systematic implementation of an advance directive program in nursing homes: a randomized controlled trial. JAMA 2000;283:1437–44. 13. Molloy DW, Russo R, Pedlar D, Bédard M. Implementation of advance directives among community-dwelling veterans. Gerontologist 2000;40:213–7. 14. Molloy DW, Guyatt GH, Goeree R, Jubelius R, Urbanyi M, Flett N, et al. A comprehensive health care directive for competent and incompetent residents of a home for the aged. Annals RCPSC 1997;30:339–45. 15. Molloy W. Let me decide. Troy, ON: Newgrange Press; 1999. 16. Molloy DW, Urbanyi M, Horsman JR, Guyatt GH, Bédard M. Two years experience with a comprehensive health care directive in a home for the aged. Annals RCPSC 1992;7:433–6. 17. Patterson C, Molloy DW, Guyatt GH, Bédard M, North J, Hassard J, et al. Systematic implementation of an advance health care directive in the community. Can J Nurs Adm 1997;10:96–108. 18. Neuman K, Wade L. Advance directives: the experience of health care professionals across the continuum of care. Soc Work Health Care 1999;28:39–48. 19. Perkins HS. Are advance directives becoming an endangered species [editorial]? Chest 1996;109:299. 20. Markson L, Clark J, Glantz L, Lamberton V, Kern D, Stollerman G. The doctor’s role in discussing advance preferences for endof-life care: perceptions of physicians practicing in the VA. J Am Geriatr Soc 1997;45:399–406. 21. Bailly DJ, DePoy E. Older people’s responses to education about advance directives. Health Soc Work 1995;20:223–8. 22. Sam M, Singer PA. Canadian outpatients and advance directives: poor knowledge and little experience but positive attitudes. CMAJ 1993;148:1497–502. 23. Sulmasy DP, Song KY, Marx ES, Mitchell JM. Strategies to promote the use of advance directives in a residency outpatient practice. J Gen Intern Med 1996;11:657–63. 24. Clarnette RM, Molloy DW. Health care directives. The Annual of Medical Direction. Columbia (MD): American Medical Directors Association; 1991:48–51. 25. Molloy DW, Bédard M, Guyatt GH, Patterson C, North J, Jubelius R, et al. Attitudes training issues and barriers for community nurses implementing an advance directive program. Perspectives 1997;21:2–8. 26. Molloy DW. Standardized Mini-Mental State Examination booklet. Troy, ON: Newgrange Press; 1999. 27. Molloy DW, Alemayehu E, Roberts R. Reliability of a Standardized Mini-Mental State Examination compared with the traditional Mini-Mental State Examination. Am J Psychiatry 1991; 148:102–5. 28. Molloy DW, Silberfeld M, Darzins P, Guyatt GH, Singer PA, Rush B, et al. Measuring capacity to complete an advance directive. J Am Geriatr Soc 1996;44:660–4. 29. Ryan CJ. Depression, decisions and the desire to die [editorial]. Med J Aust 1996;165:411. 30. Hooper SC, Vaughan KJ, Tennant CC, Perz JM. Major depression and refusal of life-sustaining medical treatment in the elderly. Med J Aust 1996;165:416–9. 31. Yesavage JA, Brink TL, Rose TL, et al. Development and validation of a geriatric screening scale: a preliminary report. J Psychiatry Res 1983;17:37–49. 32. Guyatt GH, Mitchell AL, Molloy DW, Capretta R, Horsman JR, Griffith L. Measuring patient and relative satisfaction with level or aggressiveness of care and involvement in care decisions in the context of life threatening illness. J Clin Epidemiol 1995;48:1215–24. 33. Patterson C, Molloy W, Jubelius R, Guyatt GH, Bédard M. Provisional educational needs of health care providers in palliative care in three nursing homes in Ontario. J Palliat Care 1997;13:13–7. Copyright 2000 by Turner White Communications Inc., Wayne, PA. All rights reserved. Vol. 7, No. 9 JCOM September 2000 47