Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
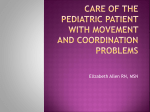
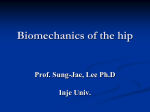
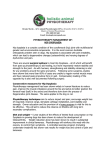
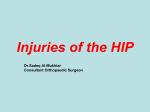
Ultrasound Evaluation of Pavlik Harness in Treatment of Infants with Developmental Dysplasia of the Hip: Prone Axial Approach to Harness in Situ C Fernández, MD; M Guasp, MD; J Gómez Fernández-Montes, MD Department of Radiology , Pediatric Imaging Section Hospital Universitario y Politécnico la Fe, Valencia, Spain Purpose • To describe a practical guideline for the performance of the ultrasound (US) in prone position for the control of Pavlik Harness (PH) in monitoring the treatment of developmental dysplasia of the hip (DDH) . Introduction • In DDH, the epiphysis is displaced posteriorly in relation to the acetabulum. • The PH is the first-choice non-invasive treatment of infants with DDH, keeping the epiphysis within the acetabulum, allowing some movement and a good perfusion, to avoid the avascular necrosis of femoral head. • Over the past five years, we have used US in prone position to monitor the treatment when PH is in place to define intraarticular position of the femoral head. Pavlik Harness The PH is a reduction harness which keeps the hips in a fetal position (flexion, abduction and external rotation) in order to get the relaxation of psoas and to reduce progressively the posterior dislocated femoral head. It is a chest halter with two straps around the shoulders and four straps for the legs. Once put the harness, should not be remove, even during US.. Technique • • • • • • Equipment specification Cautions Position of the patient Imaging of the Hip Clinical cases Follow-up Equipment specification • For newborns and infants up to 6 months old, it is recommended a real-time linear array transducer from 4 to 9 MHz. Cautions • During the scanning, the infant should be relaxed. • A quiet environment and a parent in contact with the infant are helpful. • The upper body can remain clothed. • A well-fed infant, having been fed just prior to the examination, might also be more relaxed and cooperative. Position of the Patient The examination must be performed with the infant in the harness and prone position. This position favors the intraarticular situation of the femoral head, so that if we see the epiphysis backwards displaced in this position, it will be the same in any other position. This photo illustrates the position of the transducer in order to obtain the axial view. Imaging of the hip Only the axial plane with respect to the pelvis is obtained .For teaching purposes, transverse images are similar to axial cross-sectional imaging. I T E P I T P E SS P T : Greater Trochanter, E : Epiphysis, I : Ischium, P : Pubis, SS: Sonic shadow Prone Picture View: normal and pathologic findings In the normal hip, we can see all the acetabulum from ischium to pubis, with the epiphysis centered on it . In the posterior dislocation, the epiphysis will be uncovered and closer to transducer than the ischium. Transverse View: anatomy and ultrasound correlation SS P The posterior margin of the acetabulum (ischium) should be closer to the transducer than the not-ossified femoral epiphisis and should cover it. Transverse View: normal and pathologic ultrasound findings We must compare the healthy side (left) with pathological one (right), moving the transducer from one buttock to the other, what allows us to see clearly the differences. P LEFT In the normal hip, we can see all the acetabulum, from the ischium (red arrow) to the pubis, with the epiphysis (white arrow) centered on it . RIGHT In posterior dislocation, the epiphysis will be closer to the transducer that the ischium and uncovered. The trochanter compresses the soft tissues of the buttock. Transverse View: Bilateral pathologic ultrasound findings RIGHT LEFT In cases of bilateral DDH, the comparison is even more necessary, because sometimes one hip is reduced and the other is not. US in prone position shows a patient with PH placed and both dislocated hips (the femoral epiphysis are displaced posteriorly respect to the ischiums). Case 1: Example of response to the treatment RIGHT 17/11/08 LEFT The ultrasound by posterior approach with Pavlik harness placed shows both hips centered and covered. These findings were confirmed in the following ultrasound control. Case 1 10/02/09 X-ray three months later, shows a good development of the left acetabulum, with the epiphysis covered but smaller than the right one. 12/02/10 X-ray obtained 1 year later, shows the effectiveness of the treatment with both normal hips. Case 2: Example of failure to the treatment T T I E E I RIGHT LEFT The US control of a patient with harness at second and third week of treatment shows that the left hip remains dislocated, requiring the removal of the harness and a surgical procedure. Case 2 Postoperative X-Ray which assesses the orientation of the operated hip with a plaster placed (if there is any doubt, we must do a low dose CT). Currently, we are testing the ultrasound in prone position through the hip spica cast to evaluate the situation of the intraarticular operated hip using a technique similar to the described for the harness, in order to avoid radiation by X-ray or CT. Follow-up PAVLIK HARNES First control US at 1-2 weeks Response to treatment Failure to treatment 2nd US at 1 month PH adjustment Remain with PH for 1 month 3nd US after removing PH First X-ray at 4 months old 2nd X-ray at walking age 2nd US 1 week later Persistent dislocation Early surgery to prevent the erosion of the labrum and an avascular necrosis (“Pavlik disease”) Conclusion In DDH, the ultrasound evaluation of Pavlik harness in situ by prone axial approach is a simple, safe and reproducible technique to monitor the intra-articular situation and the acetabular coverage of the femoral epiphysis. References • • • • • • • • Ladino Torres M, DiPietro M. Developmental Dysplasia of the Hip. Ultrasound Clin 2009; 4:445–455. ACR–AIUM Practice guideline for the performance of the ultrasound examination for detection and assessment of developmental dysplasia of the hip. Revised 2008 Atalar H, Sayli U, Yavuz Y, Uraş I, Dogruel H. Indicators of successful use of the Pavlik harness in infants with developmental dysplasia of the hip. International Orthopaedics (SICOT) 2007; 31: 145–150. Taylor G, Clarke N. Monitoring the treatment of developmental dysplasia of the hip with the pavlik harness. The journal of bone and joint surgery 1997; vol. 79-b, No. 5. Kelly D. Carmichael, MD; Anthony Longo, MD; David Yngve, MD; Jose Alberto Hernandez, MD; Leonard Swischuk, MD. The Use of Ultrasound to Determine Timing of Pavlik Harness Discontinuation in Treatment of Developmental Dysplasia of the Hip Orthopedics October 2008; Volume 31: Issue 10 Lerman JA, Emans JB, Millis MB, Share J, Zurakowski D, Kasser JR.Earlyfailure of Pavlik harness treatment for developmental hip dysplasia: clinical and ultrasound predictors. J Pediatr Orthop 2001 ; 21(3):348-353. Carmichael K, Longo A, Yngve D, Hernandez J, Swischuk L. The Use of Ultrasound to Determine Timing of Pavlik Harness Discontinuation in Treatment of Developmental Dysplasia of the Hip. Orthopedics. October 2008 ;Vol31: Issue 10.