Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
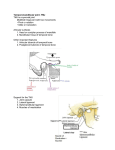
51 Temporomandibular Joint Pain DANIEL M. LASKIN KEY POINTS Temporomandibular joint (TMJ) pain must be distinguished from the pain that more commonly arises from the muscles of mastication (myofascial pain), which can produce similar signs and symptoms. are known, only three types are considered to generally produce pain: the various arthritides, derangements of the intra-articular disk, and certain neoplasms. TMJ pain also must be distinguished from pain coming from the ear or parotid gland. ARTHRITIS OF THE TEMPOROMANDIBULAR JOINT TMJ pain and masticatory muscle pain generally are accompanied by limitation of mouth opening, but not pain arising from the ear or parotid gland. Arthritis is the most common painful condition affecting the TMJ. Although osteoarthritis and rheumatoid arthritis are encountered most frequently, cases of infectious arthritis, metabolic arthritis, and presentation as part of the spondyloarthropathies are also seen in practice. Traumatic arthritis is another relatively common occurrence. Most major systemic arthropathies may also involve the TMJ and thereby give rise to pain and limited jaw movement. Displacement of the intra-articular disk in the TMJ produces pain that is accompanied by a clicking or popping sound or sudden onset of jaw locking. Pain in the temporomandibular joint (TMJ) region, a commonly encountered symptom, affects more than 10 million Americans. Because of its diverse causes, however, considerable difficulty is often involved in proper diagnosis and treatment. Owing to the proximity of the ear and parotid gland and the similar nature of pain in these areas, pathologic conditions involving these structures are often confused with conditions arising in the TMJ. Pain occurring in the adjacent muscles of mastication, also a frequently encountered situation, not only is similar to TMJ pain in character and location, but also is associated with jaw dysfunction, a common finding with painful conditions directly involving the TMJ. For these reasons, knowledge of the various painful conditions occurring in the TMJ region is essential in establishing a correct diagnosis. Because patients with primary TMJ disease often have secondary myofascial pain in the muscles of mastication, and because patients with primary myofascial pain problems in the masticatory muscles can develop secondary TMJ disease, the generally accepted term used to describe this overlapping group of conditions is temporomandibular disorders. These conditions are subdivided for purposes of diagnosis and treatment into conditions that primarily involve the TMJ (TMJ problems) and conditions that primarily involve the muscles of mastication (myofascial pain and dysfunction [MPD], masticatory myalgia). From a diagnostic standpoint, it is important to consider the numerous conditions that mimic the temporomandibular disorders or MPD by producing similar signs and symptoms (Tables 51-1 and 51-2). Table 51-3 lists the various pathologic entities that commonly involve the TMJ. Although a variety of conditions Osteoarthritis Osteoarthritis is the most common type of arthritis involving the TMJ and the most frequent cause of pain in that region. Clinical symptoms of the disease have been reported in 16% of the general population,1 but radiographic features have been found in 44% of asymptomatic individuals.2 Although the TMJ is not a weight-bearing joint in the same sense as the joints of the long bones, the stresses associated with such parafunctional habits as clenching and grinding of the teeth are sufficient to contribute to similar degenerative changes in some patients.3 Acute and chronic trauma and derangements of the intra-articular disk also are common causes of secondary degenerative arthritis. Clinical Findings Primary osteoarthritis, which usually is seen in older individuals, is insidious in its onset; it generally produces only mild discomfort, and individuals rarely complain about the condition. Secondary osetoarthritis usually occurs in younger patients (20 to 40 years old) and tends to be painful. In contrast to primary degenerative joint disease and rheumatoid arthritis, it often is limited to only one TMJ, although it may become bilateral in the late stages, and involvement of other joints is uncommon. The condition is characterized by TMJ pain that is increased by function, joint tenderness, limitation of mouth opening, and occasional clicking and popping sounds. In the late stages, crepitation may be noted in the joint. Imaging Findings The earliest radiologic feature of osetoarthritis of the TMJ, whether primary or secondary, is subchondral sclerosis in the mandibular condyle. If the condition progresses, 721 722 PART 6 | DIFFERENTIAL DIAGNOSIS OF REGIONAL AND DIFFUSE MUSCULOSKELETAL PAIN Table 51-1 Differential Diagnosis of Nonarticular Conditions Mimicking Temporomandibular Joint Pain or Myofascial Pain in the Masticatory Muscles Jaw Limitation Muscle Tenderness Pulpitis No No Pericoronitis Yes Possible Otitis media No No Parotitis Yes No Sinusitis No No Trigeminal neuralgia No No Atypical (vascular) neuralgia Temporal arteritis No No No No Trotter’s syndrome Yes No Eagle’s syndrome No No Disorder Diagnostic Features Mild to severe ache or throbbing; intermittent or constant; aggravated by thermal change; eliminated by dental anesthesia; positive radiographic findings Persistent mild to severe ache; difficulty swallowing; possible fever; local inflammation; relieved with dental anesthesia Moderate to severe earache; constant pain; fever; usually history of upper respiratory infection; no temporomandibular joint tenderness Constant aching pain, worse when eating; pressure feeling; absent salivary flow; ear lobe elevated; suppuration from duct Constant aching or throbbing; worse with change of head position; nasal discharge; often maxillary molar pain not relieved by dental anesthesia Sharp stabbing pain of short duration; trigger zone; pain follows nerve pathway; older age group; often relieved by dental anesthesia Diffuse throbbing or burning pain of long duration; often associated autonomic symptoms; no relief with dental anesthesia Constant throbbing preauricular pain; artery prominent and tender; low-grade fever; may have visual problems; elevated erythrocyte sedimentation rate Aching pain in ear, side of face, and lower jaw; deafness; nasal obstruction; cervical lymphadenopathy Mild to sharp stabbing pain in ear, throat, and retromandible; provoked by swallowing, turning head, carotid compression; usually post tonsillectomy; styloid process >2.5 cm Modified from Laskin DM, Block S: Diagnosis and treatment of myofascial pain dysfunction (MPD) syndrome, J Prosthet Dent 56:75–84, 1986. condylar flattening and marginal lipping may be noted. In the later stages, erosion of the cortical plate, osteophyte formation, or both may occur. Breakdown of the subcortical bone occasionally may result in the formation of bone cysts. Although changes in the articular fossa generally are not as severe as changes in the condyle, cortical erosion sometimes can be seen. Narrowing of the joint space also occurs in the late stages; this is indicative of concomitant degenerative changes in the intra-articular disk. Although changes in the TMJ usually can be seen on plain radiographs, sagittal and coronal computed tomography (CT) scans are the preferred modality for imaging the bony structures. Table 51-2 Differential Diagnosis of Nonarticular Conditions Producing Limitation of Mandibular Movement Jaw Limitation Muscle Tenderness Odontogenic infection Yes Yes Nonodontogenic infection Yes Yes Myositis Yes Yes Myositis ossificans No No Possible Possible Scleroderma No No Hysteria No No Tetanus Yes No Extrapyramidal reaction No No Depressed zygomatic arch Possible No Osteochondroma coronoid No No Disorder Neoplasia Diagnostic Features Fever; swelling; positive radiographic findings; tooth tender to percussion; pain relieved and movement improved with dental anesthesia Fever; swelling; negative dental findings on radiograph; dental anesthesia may not relieve pain or improve jaw movement Sudden onset; jaw movement associated with pain; areas of muscle tenderness; usually no fever Palpable nodules seen as radiopaque areas on radiograph; involvement of nonmasticatory muscles Palpable mass; regional nodes may be enlarged; may have paresthesia; radiograph may show bone involvement Skin hard and atrophic; mask-like facies; paresthesias; arthritic joint pain; widening of periodontal ligament Sudden onset after psychological trauma; no physical findings; jaw opens easily under general anesthesia Recent wound; stiffness of neck; difficulty swallowing; spasm of facial muscles; headache Patient on antipsychotic drug or phenothiazine tranquilizer; hypertonic movement; lip smacking; spontaneous chewing motions History of trauma; facial depression; positive radiographic findings Gradual limitation; jaw may deviate to unaffected side; possible clicking sound on jaw movement; positive radiograph findings Modified from Laskin DM, Block S: Diagnosis and treatment of myofascial pain dysfunction (MPD) syndrome, J Prosthet Dent 56:75–84, 1986. CHAPTER 51 Diagnosis The diagnosis of osteoarthritis is based on the patient’s history and clinical and radiographic findings. A history of trauma or parafunctional oral habits is often reported. Involvement is generally unilateral, and no significant changes are observed in any of the other joints. The pain tends to be well localized, and the TMJ is often tender to palpation. Treatment Treatment of degenerative arthritis of the TMJ is usually medical, as in other joints of the body. It involves the use of nonsteroidal anti-inflammatory drugs, application of heat, eating a soft diet, limitation of jaw function, and use of a bite appliance to control parafunction if the patient has a chronic habit of clenching or grinding the teeth. Arthrocentesis has also been shown to be helpful.4,5 Physical therapy with thermal agents, ultrasound, and iontophoresis also can be beneficial, and isotonic and isometric exercises are used to improve joint stability after acute symptoms have subsided. The use of intra-articular steroid injections is controversial; they should be used only in patients with acute symptoms that do not respond to other forms of medical management. Because of the potentially damaging effects of long-acting steroids,4,6 they should be limited to no more than three or four single injections given at 3-month intervals. Intra-articular injection of highmolecular-weight sodium hyaluronate given twice, 2 weeks apart, has been shown to have essentially the same therapeutic effect as a steroid injection, without the potential adverse effects.5,7 When the acute symptoms have been controlled, therapy is directed toward control of factors possibly contributing to the degenerative process. Unfavorable loading of the joint is eliminated by replacement of missing teeth to establish a good, functional occlusion; by correction of any severe dental malrelationships through orthodontics or orthognathic surgery; and by continued use of a bite appliance at night to control teeth-clenching or teeth-grinding habits.6,8 In patients in whom medical management for 3 to 6 months fails to relieve the symptoms, surgical management may be indicated. Surgery involves removal of only the minimal amount of bone necessary to produce a smooth articular surface. Unnecessary removal of the entire cortical plate, as occurs with the so-called condylar shave procedure or high condylotomy, can lead to continuation of the resorptive process in some instances, and should be avoided if possible. Rheumatoid Arthritis More than 50% of patients with rheumatoid arthritis have involvement of the TMJ.9 Although the TMJ may be affected early in the course of the disease, other joints in the body usually are involved first. The general female-tomale ratio is 3 : 1. TMJ involvement may also characterize juvenile inflammatory arthritis. In children, destruction of the mandibular condyle by the disease process results in growth retardation and facial deformity characterized by a | Temporomandibular Joint Pain 723 severely retruded chin. Fibrous or bony ankylosis is a possible sequel at all ages. Clinical Findings Patients with rheumatoid arthritis of the TMJ have bilateral pain, tenderness, swelling in the preauricular region, and limitation of mandibular movement. These symptoms are characterized by periods of exacerbation and remission. Joint stiffness and pain are usually worse in the morning and decrease during the day. The limitation in mandibular movement worsens as the disease progresses; the patient also may develop an anterior open bite. Imaging Findings Although radiographic changes may not be noted in the early stages of the disease, about 50% to 80% of patients show bilateral evidence of demineralization, condylar flattening, and bone erosion as the disease progresses, so the articular surface appears irregular and ragged. Erosion of the glenoid fossa also is seen sometimes. Narrowing of the joint space is caused by destruction of the intra-articular disk. With continued destruction of the condyle, loss of ramus height can lead to contact of only the posterior teeth and an anterior open bite. Diagnosis Rheumatoid arthritis is diagnosed on the basis of the history, clinical and radiographic findings, and confirmatory laboratory tests. Distinguishing features for rheumatoid arthritis and degenerative arthritis of the TMJ are shown in Table 51-3. Treatment Treatment of rheumatoid arthritis of the TMJ is similar to that provided for other joints.7,10 Anti-inflammatory drugs are used during the acute phases, and mild jaw exercises are used to prevent excessive loss of motion when acute symptoms subside. In severe cases, disease-modifying drugs, such as methotrexate, and biologic agents, including etanercept, infliximab, adalimumab, certolizumab, golimumab, abatacept, tocilizumab, and rituximab, may be used pending systemic presentation. Orthognathic surgery may be necessary in patients with an anterior open bite after the disease goes into remission, or in patients in whom ankylosis develops after that condition is corrected. Spondyloarthropathies In addition to the adult and juvenile forms of rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, and reactive arthritis also can involve the TMJ.8-13 Psoriatic Arthritis Psoriatic arthritis occurs in approximately one-third of patients who have cutaneous psoriasis. It can have a sudden onset, can be episodic in nature, and may show spontaneous 724 PART 6 | DIFFERENTIAL DIAGNOSIS OF REGIONAL AND DIFFUSE MUSCULOSKELETAL PAIN Table 51-3 Differential Diagnosis of Temporomandibular Joint (TMJ) Diseases Disorder Jaw Limitation Muscle Tenderness Agenesis No Yes Condylar hypoplasia No No Condylar hyperplasia No No Possible Yes Infectious arthritis Yes No Rheumatoid arthritis Yes Yes Spondyloarthropathies Psoriatic arthritis Yes Yes Ankylosing spondylitis Yes Yes Metabolic arthritis Gout Yes Yes Pseudogout Yes Yes Traumatic arthritis Yes Yes Degenerative arthritis Yes Yes Ankylosis No Yes Internal disk degeneration Yes Yes Neoplasia Diagnostic Features Congenital; usually unilateral; mandible deviates to affected side; unaffected side long and flat; severe malocclusion; often ear abnormalities; radiograph shows condylar deficiency Congenital or acquired; affected side has short mandibular body and ramus, fullness of face, deviation of chin; body of mandible elongated and face flat on unaffected side; malocclusion; radiograph shows condylar deformity, antegonial notching Facial asymmetry with deviation of chin to unaffected side; cross-bite malocclusion; prognathic appearance; lower border of mandible often convex on affected side; radiograph shows symmetric enlargement of condyle Mandible may deviate to affected side; radiographs show enlarged, irregularly shaped condyle or bone destruction, depending on type of tumor; unilateral condition Signs of infection; may be part of systemic disease; radiograph may be normal early, later can show bone destruction; fluctuance may be present; pus may be obtained on aspiration; usually unilateral Signs of inflammation; findings in other joints (hands, wrists, feet, elbows, ankles); positive laboratory test results; retarded mandibular growth in children; anterior open bite; radiograph shows bone destruction; usually bilateral Presence of cutaneous psoriasis; nail dystrophy; involvement of distal interphalangeal joints; radiograph shows condylar erosion; negative for rheumatoid factor Frequent involvement of the spine and sacroiliac joint; extra-articular manifestations of spondylitis include iritis, anterior uveitis, aortic insufficiency, and conduction defects; erosive condylar changes; TMJ ankylosis may occur Usually sudden onset; often monoarticular; commonly involves great toe, ankle, and wrist; joint swollen, red, and tender; increased serum uric acid; late radiographic changes Generally unilateral; TMJ may be only joint involved; joint frequently swollen; presence of intra-articular calcification; may be a history of trauma History of trauma; radiograph normal except for possible widening of joint space; local tenderness; usually unilateral Unilateral joint tenderness; often crepitus; TMJ may be only joint involved; radiograph may be normal or show condylar flattening, lipping, spurring, or erosion Usually unilateral, but can be bilateral; may be history of trauma; young patient may show retarded mandibular growth; radiographs show loss of normal joint architecture Pain exacerbated by function; clicking on opening or opening limited to <25 mm with no click; positive magnetic resonance imaging findings; may be history of trauma; usually unilateral Modified from Laskin DM, Block S: Diagnosis and treatment of myofascial pain dysfunction (MPD) syndrome, J Prosthet Dent 56:75–84, 1986. remission.9,12 Often only one TMJ is involved. Symptoms include TMJ pain and tenderness, restricted jaw movement, and crepitation, mimicking the symptoms of rheumatoid arthritis.9,12 Radiographic changes are nonspecific and cannot be distinguished easily from those of other types of arthritis, particularly rheumatoid arthritis and ankylosing spondylitis.13,14 They usually involve erosive changes in the condyle and glenoid fossa associated with extreme narrowing of the joint space.11,15,16 In severe cases, ankylosis may develop, reflected occasionally in new bone formation at earlier stages.12,17 The diagnosis usually is based on the triad of psoriasis, radiographic evidence of erosive arthritis, and a negative serologic test for rheumatoid factor. Even in the presence of a rash, however, the diagnosis cannot be absolutely confirmed. The differential diagnosis always should include rheumatoid arthritis, reactive arthritis, ankylosing spondylitis, and gout. Treatment of psoriatic arthritis of the TMJ is similar to that of rheumatoid arthritis, and is driven essentially by the imperative to treat the systemic inflammatory disease process.13,18-21 Surgery is necessary if ankylosis occurs. Ankylosing Spondylitis About one-third of patients with ankylosing spondylitis develop TMJ involvement several years after onset of the disease. Pain and limitation of jaw movement are the most common symptoms, and ankylosis can develop in advanced cases.8,11,14,22 On radiographic examination, about 30% of patients show erosive changes in the condyle and fossa and narrowing of the joint space.15,23 In long-standing cases, a CHAPTER 51 more florid osteophytic response is sometimes seen during quiescent periods. The severity of the changes seems to be related to the severity of the disease. Treatment of ankylosing spondylitis of the TMJ is generally medical and is part of the total management of the patient. Physical therapy is used to improve jaw mobility, and bite appliances are used, when indicated, to reduce parafunctional stress on the joint. If ankylosis develops, surgery is the treatment of choice.24 | Temporomandibular Joint Pain 725 Chills, fever, sweating, and systemic findings characteristic of the specific type of infection also are present. Often the teeth cannot be occluded because of swelling within the joint. In pyogenic forms of infectious arthritis, fluctuation may be noted in the joint region. Patients with Lyme disease show characteristic skin lesions and often positive serology.18,29 Imaging Findings Reactive Arthritis Reactive arthritis of the temporomandibular joint is more common in males than in females. It is characterized by recurrent pain, swelling, and limitation of mouth opening.25 Radiographically, condylar erosion may be evident.26 Treatment is similar to that of the other seronegative spondyloarthropathies, consisting of nonsteroidal anti-inflammatory drugs, intra-articular steroids, and disease-modifying drugs. If a specific triggering bacterial infection can be identified, an appropriate antibiotic should be prescribed. Traumatic Arthritis Acute trauma to the mandible that does not result in a fracture can still produce injury to the TMJ. When this occurs in a child, it is essential to warn the parents about the possibility of future retardation of mandibular growth and associated facial deformity resulting from damage to the articular cartilage, which is an important growth site.16,27 Traumatic arthritis is characterized by TMJ pain and tenderness and limitation of jaw movement. The resultant inflammation and occasional hemarthrosis can lead to loss of tooth contact on the affected side. Frequently, bruises or lacerations are apparent at the site of the initial injury. No radiographic changes may be seen, or widening of the joint space may be produced by intra-articular edema or hemorrhage. In some instances, radiographs may show an intracapsular fracture that was not recognized on clinical examination. Treatment of traumatic arthritis consists of the use of nonsteroidal anti-inflammatory drugs, application of heat, a soft diet, and initial restriction of jaw movement. When acute symptoms subside, range-of-motion exercises should be used to avoid fibrous ankylosis. Infectious Arthritis Infectious arthritis rarely involves the TMJ. Although it can affect the joint as part of such systemic diseases as gonorrhea, syphilis, tuberculosis, and Lyme disease,17,18,28,29 the most common way is by direct extension of an adjacent infection of dental, parotid gland, or otic origin.19,30 Occasionally, it also may occur from localization of blood-borne organisms in the joint after a traumatic injury or by direct involvement through a penetrating wound.20,30 The most common pathogens are Staphylococcus aureus, Haemophilus influenzae, and Streptococcus species.31 Clinical Findings Infectious arthritis generally results in unilateral pain, tenderness, swelling, and redness in the region of the TMJ. Radiographic findings are usually normal in early stages of the disease because of lack of bony involvement, but the intra-articular accumulation of pus or inflammatory exudate may cause separation of articulating surfaces, which can be detected on magnetic resonance imaging (MRI). Later, depending on the severity and chronicity of the infection, varying degrees of bony destruction, ranging from damage to the articular surface of the mandibular condyle to extensive osteomyelitis, may be seen. In the late stages, fibrous or bony ankylosis may occur. In children, infectious arthritis can affect growth of the condyle, resulting in facial asymmetry. Treatment Treatment of infectious arthritis includes the use of appropriate antibiotics, proper hydration, control of pain, and limitation of jaw movement. Arthrocentesis with Ringer’s solution one to three times weekly until acute symptoms subside has also been recommended.32 Suppurative infections may require aspiration, incision, and drainage, or sequestrectomy. When bone loss has been extensive, reconstructive procedures may be necessary. In children in whom mandibular growth has been affected, a costochondral graft can be used to correct facial asymmetry and re-establish growth of the mandible. Metabolic Arthritis Metabolic arthritis, which can accompany gout or pseudogout (calcium pyrophosphate dehydrate arthropathy), is rare in the TMJ.21,33 Gout Gouty arthritis of the TMJ occurs most frequently in men older than 40 years and usually is preceded by involvement of one or more joints of the feet or hands. The attack usually occurs suddenly, and the joint becomes swollen, painful, red, and tender. Recovery may occur in a few days, and remission can last for months to years. When attacks are infrequent, radiographic changes may not be noted for a long time. Because so few cases have been reported, the precise radiographic changes that occur have not been well documented. Calcified areas in the disk, destruction of the hard tissues of the joint, condylar exostoses and spurring, and the presence of tophi have been described.21,33-35 The initial approach to treatment of gout involving the TMJ is medical. If symptoms are not controlled, however, surgical débridement of the joint and arthroplasty may be indicated. 726 PART 6 | DIFFERENTIAL DIAGNOSIS OF REGIONAL AND DIFFUSE MUSCULOSKELETAL PAIN A Pseudogout Calcium pyrophosphate dehydrate arthropathy (pseudo gout) in the TMJ clinically mimics gout, and the mandibular condyle may show degenerative and erosive changes radiographically. In the primary form, which usually is seen in older patients, intra-articular calcification is noted (chondrocalcinosis), and diffuse calcification occurs in the intra-articular disk.21-25,36-39 Similar changes are seen in the secondary form, but it occurs in younger patients and frequently is preceded by a history of trauma. Just as in gout of the TMJ, the initial treatment of pseudogout is medical, and surgery is reserved for patients in whom such treatment is ineffective. E B INTERNAL DERANGEMENTS Internal derangements are a common cause of pain in the TMJ. They represent a disturbance in the normal anatomic relationship between the intra-articular disk and the condyle, resulting in interference with the smooth movement of the joint. Clinical Findings Three stages of internal derangement have been identified: (1) a painless incoordination phase, in which a momentary catching sensation is felt during mouth opening; (2) anterior disk displacement with reduction into the normal position during mouth opening, which is characterized by a clicking or popping sound (Figure 51-1); and (3) anterior disk displacement without reduction on attempted mouth A D C Figure 51-2 A-E, Anterior displacement of the intra-articular disk without reduction on attempted mouth opening. The displaced disk acts as a barrier and prevents full translation of the condyle. (Modified from McCarty W: Diagnosis and treatment of internal derangements of the articular disc and mandibular condyle. In Solberg WK, Clark GT, editors: Temporomandibular joint problems: biologic diagnosis and treatment, Chicago, 1980, Quintessence, p 151.) opening, which is characterized by restriction of jaw movement, or locking (Figure 51-2). Joint pain in patients with anterior disk displacement, with or without reduction, is caused by condylar compression of the highly innervated retrodiskal tissue that occupies the glenoid fossa as the intra-articular disk assumes a more forward position, and by the accompanying inflammation. Etiology Closing click F B Opening click E C D Figure 51-1 Anterior displacement of the intra-articular disk with reduction on opening of the mouth. A clicking or popping sound occurs as the disk returns to its normal position in relation to the condyle. During closure, the disk again becomes anteriorly displaced, sometimes accompanied by a second sound (reciprocal click). (Modified from McCarty W: Diagnosis and treatment of internal derangements of the articular disc and mandibular condyle. In Solberg WK, Clark GT, editors: Temporomandibular joint problems: biologic diagnosis and treatment, Chicago, 1980, Quintessence, p 155.) The three main causes of internal derangement of the intraarticular disk are trauma, abnormal functional loading of the joint, and degenerative joint disease.26,40 It has been suggested that spasm in the lateral pterygoid muscle, a portion of which attaches to the anterior aspect of the disk, can lead to a disk derangement, but evidence for this theory is circumstantial. Although some clinicians believe that occlusal factors also play a role in causing internal derangements, no conclusive studies have shown such a relationship. Acute macrotrauma is probably the most common cause of internal derangement. Among the incidents that have been implicated are a blow to the jaw, endotracheal intubation, cervical traction, and iatrogenic stretching of the joint during dental or oral surgical procedures. Although whiplash injuries frequently have been implicated in the development of internal derangement, a study of 155 patients with this type of injury showed that only 1 developed clicking in the TMJ immediately after the automobile accident.27,41 At 1 month of follow-up, two additional patients of the 129 contacted experienced clicking, but at 1 year, no additional patients of the 104 contacted had developed clicking. Although internal derangements of the TMJ can be caused by a whiplash injury, the incidence seems to be low. CHAPTER 51 Whether a patient merely develops alterations in the articular surface leading to a catching or binding sensation, anterior disk displacement with reduction on mouth opening (clicking or popping), or anterior disk displacement without reduction during mouth opening (locking) after trauma to the TMJ depends on the severity of the injury. Although associated traumatic arthritis causes pain during function in each of these instances, the pain is more severe in the last two conditions because of compression of retrodiskal tissue, which is now located in the articular zone. Functional overloading of the TMJ associated with the habit of chronic teeth clenching is another frequent cause of internal derangements. Although the TMJ is constructed for eccentric movements, it is not constructed for the constant isometric loading and unloading that occurs during this activity. Such parafunction affects the lubrication of the joint and alters the articular surfaces, introducing friction between the disk and the condyle that leads to degenerative changes in the articular surfaces and results in gradual anterior displacement of the disk.26,28,40,42 Degenerative joint disease may precede the development of an internal derangement, or it may occur after the development of an internal derangement. In the first instance, changes in the character of the articulating surfaces result in an inability of the parts to glide smoothly over each other, gradually leading to forward displacement of the disk, which normally rotates posteriorly during mouth opening. In the second instance, the displaced disk results in an altered relationship between articulating components of the joint, which leads to degenerative changes in these structures. In patients in whom the condition causing the degenerative joint disease is still active, whether primarily or secondarily, the condition and the disk derangement must be treated for the problem to be resolved completely. Imaging Findings Depending on the cause of the internal derangement and its duration, radiographs may or may not show any evidence of degenerative joint disease. Magnetic resonance imaging shows anterior disk displacement in the closed mouth position, however, as well as a return to a normal disk relationship during mouth opening in patients with clicking and popping; in patients with locking, the disk remains in the anterior position on attempted mouth opening, and movement of the condyle is limited. A small group of patients with locking show the intra-articular disk in normal position when the teeth are in occlusion, rather than anteriorly displaced, and no change in disk position occurs when the patient attempts to open the mouth.29,43 In such cases, adhesion of the disk to the articular eminence prevents translation of the condyle. These patients differ from those with anteriorly displaced, nonreducing disks in that they do not have a history of TMJ clicking preceding the sudden onset of locking. Treatment Initial treatment of patients with painful clicking or popping in the TMJ consists of a nonsteroidal anti-inflammatory drug; a soft, nonchewy diet; and use of a bite-opening appliance to reduce compression of retrodiskal tissue | Temporomandibular Joint Pain 727 Management of internal derangements of the TMJ Clicking Analgesics Soft diet Limited jaw function Bite appliance Pain continues Pain relieved Diskoplasty Continue bite appliance in patients with parafunction Locking Arthrocentesis or arthroscopic lysis and lavage Bite appliance in patients with parafunction Pain continues Diskoplasty or diskectomy Pain relieved Continue bite appliance Periodic follow-up Periodic follow-up Figure 51-3 Management of internal derangements of the temporomandibular joint (TMJ). Patients with painful clicking or locking are treated medically initially, whereas patients with locking require surgical intervention. (Figure 51-3). A muscle relaxant drug can be added to the regimen if the patient has associated myofascial pain. When the pain has stopped, no further treatment is necessary, although joint noise still may be present. A long-term follow-up study (1 to 15 years) of 190 patients with a history of clicking treated by such conservative nonsurgical modalities, which are not directed specifically to the problems of joint noise or disk displacement, showed that the condition worsened in only 1%, indicating that it is permissible to observe individuals with painless clicking as long as they remain otherwise asymptomatic.30,44 However, in those patients who have teeth-clenching and -grinding habits, use of a bite appliance is indicated to control these habits. In patients with pain and clicking in the TMJ that is unresponsive to nonsurgical management, the disk should be repositioned arthroscopically or by open surgery (diskoplasty). Patients with parafunctional habits should continue the use of a bite appliance when sleeping. In patients with locking (anterior disk displacement without reduction), whether painful or not, treatment is urgent because if the condition is left untreated for a long time, subsequent management can be complicated by further degenerative changes in the disk and condyle that make disk salvage (diskoplasty) impossible. Initial treatment involves joint lavage and lysis of adhesions arthroscopically or by arthrocentesis. The latter involves establishment of inlet and outlet portals in the upper joint space with hypodermic needles, irrigation with lactated Ringer’s solution to remove inflammatory tissue breakdown products and cytokines, and lysis of adhesions by hydraulic distention and manual manipulation of the joint (Figure 51-4).31,45 The results of arthrocentesis parallel those achieved with arthroscopic lysis and lavage, and the procedure is less invasive. Although neither of these procedures restores the disk to its normal position, they do restore disk and joint mobility, and they reduce pain and improve function in most 728 PART 6 | DIFFERENTIAL DIAGNOSIS OF REGIONAL AND DIFFUSE MUSCULOSKELETAL PAIN A tumor, and synovial hemangioma have been reported. Malignant tumors of the TMJ are even rarer, with infrequent reports of fibrosarcoma, chondrosarcoma, synovial fibrosarcoma, osteosarcoma, malignant fibrous histiocytoma, malignant schwannoma, leiomyosarcoma, and multiple myeloma. The TMJ also can be invaded by neoplasms from the cheek, the parotid gland, the external auditory canal, and the adjacent ramus of the mandible. Metastasis to the condyle from distant neoplasms in the breast, lung, prostate, colon, thyroid gland, liver, stomach, and kidney has been described. Tumors of the TMJ can cause pain, limitation of jaw movement, deviation of the mandible to the affected side on attempted mouth opening, and difficulty in occluding the teeth. Depending on the nature of the condition, radiographs may show bony deformation, apposition, or resorption. A biopsy is necessary to establish the definitive diagnosis. MYOFASCIAL PAIN AND DYSFUNCTION B Figure 51-4 Temporomandibular joint arthrocentesis. A, Hypodermic needles inserted into the upper joint space to allow lavage of the joint. B, Joint being irrigated with lactated Ringer’s solution. patients.32,33,46,47 In these patients, retrodiskal tissue within the joint undergoes fibrosis and acts as a pseudodisk. It is important that patients who have teeth-grinding or teethclenching habits are prescribed a bite appliance postoperatively to wear while sleeping. In patients who do not respond favorably to arthroscopy or arthrocentesis, the displaced disk should be repositioned by an open operation. If the disk is extremely deformed and cannot be repositioned, or if a large, nonreparable perforation in the disk or a tear in the retrodiskal tissue is present, the disk should be removed. Although autogenous auricular cartilage or dermal grafts, or temporalis muscle flaps, have been used as a disk replacement, results have been unpredictable.31,45,48 More recent long-term studies have shown that most patients can tolerate a diskless joint.34,49 Currently, no acceptable alloplastic substitutes for the disk are available. NEOPLASMS Although primary neoplasms involving the TMJ are uncommon, they must be considered in the differential diagnosis of painful conditions affecting this region.35,36,50,51 Chondroma, osteochondroma, and osteoma are the most frequently encountered benign tumors, but isolated cases of fibro-osteoma, myxoma, fibrous dysplasia, giant cell reparative granuloma, aneurysmal bone cyst, synovioma, synovial chondromatosis, chondroblastoma, osteoblastoma, glomus Myofascial pain and dysfunction (MPD), or masticatory myalgia, is considered to be a psychophysiologic disease that primarily involves the muscles of mastication, and not the TMJ. Women are affected more frequently than men; the ratio in various reports ranges from 3 : 1 to 5 : 1. Although the condition can occur in children, the incidence seems to be greatest in adults 20 to 40 years old. MPD frequently is confused with painful conditions affecting the TMJ, such as degenerative arthritis or internal derangements, because patients with primary MPD can develop these diseases secondarily, and patients with primary joint disease can develop secondary MPD. Enhanced understanding of the causes and pathogenesis of this condition makes its diagnosis easier and its treatment more effective.37,38,52,53 Etiology Psychological stress has been suggested as an important contributing factor in the development of MPD (psychophysiologic theory).39,54,55 It is hypothesized that in most patients, stress-related, centrally induced increases in muscle activity, frequently combined with the presence of parafunctional habits such as clenching or grinding of the teeth, may result in associated muscle fatigue, pain, and limited mouth opening.40,54 However, similar symptoms occasionally have been seen to result from muscle overextension, muscle overcontraction, or trauma (Figure 51-5). A counter-theory (the pain adaptation theory of Lund)56 has been proposed to suggest that pain in the masticatory muscles leads to a reduction rather than an increase in muscle activity as a protective mechanism, and this causes the limitation in mouth opening.; however, this theory does not explain the origin of the pain. Despite extensive research, the cause of myofascial pain and dysfunction remains unknown. Clinical Findings Pain of unilateral origin is the most common symptom of MPD. In contrast to the pain associated with joint disease, which is well localized, the pain of muscle origin is more CHAPTER 51 Stress Muscular overextension Muscular hyperactivity “Dental irritation” Muscular fatigue Muscular overcontraction Myofascial pain-dysfunction Contracture Occlusal disharmony Internal derangement Degenerative arthritis Altered chewing pattern Figure 51-5 Causes of myofascial pain and dysfunction. Although the diagram shows three pathways, the one involving psychological stress is most common. The mechanism by which stress leads to myofascial pain and dysfunction is termed the psychophysiologic theory. (Modified from Laskin DM: Etiology of the pain-dysfunction syndrome, J Am Dent Assoc 79:147–153, 1969. Copyright © 1969 American Dental Association. Reprinted by permission of ADA Publishing Co., Inc.) diffuse. The patient generally is unable to identify accurately the specific site involved; this can serve as an important diagnostic criterion in distinguishing between muscle and joint disorders. Depending on the muscle involved, the pain associated with MPD may be described by the patient in various ways. The masseter is the muscle most frequently involved, and the patient usually refers to the pain as a jaw ache. The temporalis is the next most commonly involved muscle; it produces pain on the side of the head, which is interpreted by the patient as a headache. Involvement of the lateral pterygoid muscle produces earache or a deep pain behind the eye, whereas medial pterygoid involvement causes discomfort on swallowing and the feeling of a painful, swollen gland beneath the angle of the mandible. Medial pterygoid invol vement also can cause stuffiness or a full feeling in the ear. The pain associated with MPD is usually constant, but it is often more severe on arising in the morning or may worsen gradually as the day progresses. Pain generally is exacerbated by jaw function, especially during such activities as eating and excessive talking. Myofascial pain tends to be regional rather than local, and patients with a longstanding problem may complain that pain in the facial region has spread to the cervical area and later to the shoulders and back. Tenderness in the muscles of mastication, another common finding, can be used to confirm the source of the pain in muscles that are accessible to palpation (masseter, temporalis, and medial pterygoid). Although muscle tenderness usually is not reported by the patient, this symptom can be elicited easily by the examiner. The most frequent sites of tenderness are near the angle of the mandible, in the belly and the posterosuperior aspect of the masseter, in the anterior temporal region, and over the temporal crest on the anterior aspect of the coronoid process. The location of some of the tender areas suggests that tendons may be a source of pain and tenderness. Limitation of mandibular movement is the third cardinal symptom of MPD. It manifests as an inability to open the mouth as wide as usual and as a deviation of the mandible | Temporomandibular Joint Pain 729 to the affected side when mouth opening is attempted. Lateral excursion to the unaffected side is reduced. The limitation of mandibular movement usually is correlated with the amount of pain present. A clicking or popping sound in the TMJ is another finding in some patients with MPD. This is not a cardinal sign, however, because it occurs only in patients with a chronic teeth-clenching habit, which gradually produces frictional changes in the joint and subsequent disk displacement.26,40 The presence of joint sounds alone is insufficient to allow a diagnosis of MPD. Joint sounds must be accompanied by myofascial pain and tenderness in the masticatory muscles that began before the onset of the joint noise. Such patients must be distinguished from patients with a primary internal derangement, in whom muscle splinting produces myofascial pain and tenderness after the onset of the joint noise. The history and differences in physical findings are helpful in making this distinction. In addition to having the three cardinal symptoms of pain, muscle tenderness, and limitation of mouth opening, patients with MPD usually have no clinical or radiographic evidence of pathologic changes in the TMJ. These negative characteristics are important in establishing the diagnosis because they confirm that the primary site of the problem is not the articular structures. Diagnosis Because the cardinal signs and symptoms of MPD are similar to those produced by such organic problems involving the TMJ as degenerative joint disease and internal disk derangement and by a variety of nonarticular conditions (see Tables 51-1 and 51-2), diagnosis of this condition can be difficult, requiring a careful history and a thorough clinical evaluation. Periapical radiographs of the teeth and screening radiographs (transcranial, transpharyngeal, or panoramic) of the TMJs can be helpful in eliminating dental problems or gross joint disease. If screening views of the TMJs show some abnormality, CT scans are usually advisable for confirmation. MRI also can be useful in determining the position of the disk when an internal derangement of the TMJ is being considered. Depending on the suspected condition, other radiographic views of the head and neck and scintigraphy may be needed to establish a final diagnosis. Certain laboratory tests may be helpful in some instances. These include a complete blood cell count if an infection is suspected; serum calcium, phosphorus, and alkaline phosphatase measurements for possible bone disease; serum uric acid determination for gout; serum creatinine and creatine kinase levels as indicators of muscle disease; and erythrocyte sedimentation rate, rheumatoid factor, latex fixation, and antinuclear antibody tests for suspected rheumatoid arthritis. Electromyography can be used to evaluate muscle function. Psychological evaluation and psychometric testing are good research tools, but they have little diagnostic value other than in identifying the presence of associated abnormal behavioral characteristics. A condition that sometimes is confused with myofascial pain is fibromyalgia, particularly when MPD involves several regions in addition to the face. Although a small subset of patients with MPD eventually may develop fibromyalgia, these are probably distinct conditions.41,57 Table 51-4 lists 730 PART 6 | DIFFERENTIAL DIAGNOSIS OF REGIONAL AND DIFFUSE MUSCULOSKELETAL PAIN Table 51-4 Distinguishing Features of Myofascial Pain and Fibromyalgia Myofascial Pain Fibromyalgia Age distribution Gender distribution Distribution of pain 20-40 years Mainly women Localized; usually unilateral Tender points Trigger points Fatigue Few Uncommon Localized muscle fatigue Common 20-50 years Mainly women Generalized; bilaterally symmetric Multiple Common Generalized fatigue Common Sleep disturbance becomes symptom free, the medications are stopped first, and wearing the bite appliance is discontinued next. If the patient has a return of symptoms, and the appliance is worn only at night, its use can be continued indefinitely. Patients who do not respond to the use of a bite appliance are entered into phase III treatment for 4 to 6 weeks. In this phase, physical therapy (heat, massage, ultrasound, electrogalvanic stimulation)60 or relaxation therapy (electromyographic biofeedback, conditioned relaxation)61 is added to the regimen. No evidence shows that one form of treatment is better than another, and either can be used Phase I Therapy (2-4 weeks) the distinguishing characteristics of myofascial pain versus fibromyalgia. Treatment Treatment of MPD is divided into four phases.42,58 When a definitive diagnosis is made, phase I therapy should be started (Figure 51-6). Phase I therapy initially involves providing the patient with some understanding of the problem. Because patients often have difficulty accepting a psychophysiologic explanation for their condition, the discussion should deal with the issue of muscle fatigue as the cause of the pain and dysfunction, delaying consideration of the role of stress and psychological factors until the symptoms have improved, and the patient’s confidence has been gained. Relating the symptoms to the specific masticatory muscles from which they arise helps the patient understand the reason for the type and location of the pain—headache from the temporalis muscle, jaw ache from the masseter muscle, discomfort on swallowing and stuffiness in the ear from the medial pterygoid muscle, and earache and pain behind the eye from the lateral pterygoid muscle. In addition to the initial explanation, the patient should be counseled regarding home therapy; this includes recommendations about avoidance of clenching and grinding of the teeth, eating a soft diet, use of moist heat and massage on the masticatory muscles, and limitation of jaw movement. A nonsteroidal anti-inflammatory drug should be prescribed for the pain. In patients who have problems sleeping, a small dose of amitriptyline at bedtime is helpful in improving sleep and reducing parafunction. About 50% of these patients experience resolution of their symptoms within 2 to 4 weeks with phase I therapy. For patients whose symptoms persist, phase II therapy is initiated. Home therapy and medications are continued, and a bite appliance is made for the patient. Although numerous types have been used, the Hawley-type maxillary appliance is probably most effective because it prevents contact of the posterior teeth and prevents most forms of parafunctional activity (Figure 51-7).43,59 The appliance generally is worn at night, but it can be worn for 5 to 6 hours during the day, if necessary. The appliance should not be worn continuously, however, because the posterior teeth may supraerupt in some patients. With phase II therapy, another 20% to 25% of patients become symptom free in 2 to 4 weeks. When the patient Initial explanation of the problem Home therapy Medication for pain and sleep Symptoms eliminated Symptoms persist Phase II Therapy (2-4 weeks) Reevaluate diagnosis Check for compliance Phase out therapy Symptoms eliminated Continue home therapy and medications Prescribe a bite appliance Final explanation of problem Instructions for self-management Follow-up appointments Symptoms persist Phase III Therapy (4-6 weeks) Symptoms eliminated Continue home therapy and medications Reevaluate the bite appliance Initiate physical therapy or relaxation therapy Symptoms persist Phase IV Therapy Consultation Pain center Psychological counseling Figure 51-6 Management of myofascial pain and dysfunction. Treatments are divided into four phases. If the symptoms are eliminated in any of the first three phases, the ongoing therapy is gradually phased out, and the patient is instructed in continued self-management of the condition. (Modified from Laskin DM, Block S: Diagnosis and treatment of myofascial pain dysfunction [MPD] syndrome, J Prosthet Dent 56:75–84, 1986.) CHAPTER 51 Figure 51-7 Hawley-type maxillary bite appliance. Only the anterior teeth contact the appliance, and space between the posterior teeth is evident (arrow). first. If one is unsuccessful, the other can be tried. Phase III therapy usually helps another 10% to 15% of patients. If all of these approaches fail, and no question arises about the correctness of the diagnosis, psychological counseling is recommended. This counseling involves helping patients identify possible stresses in their lives and learning to cope with such situations. If the diagnosis is in doubt, the patient should be referred first for appropriate dental and neurologic consultation and re-evaluation. Another alternative is to refer patients with recalcitrant MPD to a TMJ center or pain clinic because such patients generally require a multidisciplinary approach for successful treatment. SUMMARY Successful management of patients with temporomandibular disorders depends on establishing an accurate diagnosis and using proper therapy based on an understanding of the cause of the condition being treated. Of particular importance is separating patients with MPD, who constitute the major group encountered and who are not surgical candidates, from patients with TMJ disease, who frequently require surgical treatment. Even in the latter group, many commonly encountered conditions, such as arthritis and internal disk derangements, often respond to nonsurgical therapy, and this type of treatment should be given a fair trial before more aggressive management is considered. References 1. Merjersjo C: Therapeutic and prognostic considerations in TMJ osteoarthrosis: a literature review and a long-term study in 11 subjects, J Craniomandib Pract 5:70, 1987. 2. Madsen B: Normal variations in anatomy, condylar movements and arthrosis frequency of the TMJs, Acta Radiol 4:273, 1966. 3. Milam SB, Zardeneta G, Schmitz JP: Oxidative stress and degenerative temporomandibular joint disease, J Oral Maxillofac Surg 56:214, 1998. 4. Manfredini D, Bonnini S, Arboretti R, et al: Temporomandibular joint osteoarthritis: an open label trial of 76 patients treated with arthrocentesis and hyaluronic acid injections, Int J Oral Maxillofac Surg 38:827, 2009. | Temporomandibular Joint Pain 731 5. Onder ME, Tuz HH, Kocyigit D, et al: Long-term results of arthrocentesis in degenerative temporomandibular disorders, Oral Surg Oral Med Oral Pathol Radiol Endod 107:1, 2008. 6. Haddad IK: Temporomandibular joint osteoarthritis: histopathological study of the effects of intra-articular injection of triamcinolone acetonide, Saudi Med J 21:675, 2000. 7. Bjornland T, Gjaerum AA, Moystad A: Osteoarthritis of the temporomandibular joint: an evaluation of the effects and complications of corticosteroid injection compared with injection with sodium hyaluronate, J Oral Rehabil 34:583, 2007. 8. Abubaker AO, Laskin DM: Nonsurgical management of arthritis of the temporomandibular joint, Oral Maxillofac Surg Clin N Am 7:1, 1995. 9. Bessa-Nogueira RV, Vasconcelos BC, Duarte AP, et al: Targeted assessment of the temporomandibular joint in patients with rheumatoid arthritis, J Oral Maxillofac Surg 66:1804, 2008. 10. Zide MF, Carlton D, Kent JH: Rheumatoid arthritis and related arthropathies: systemic findings, medical therapy, and peripheral joint surgery, Oral Surg Oral Med Oral Pathol 61:119, 1986. 11. Davidson C, Wojtulewsky JA, Bacon PA, et al: Temporomandibular joint disease in ankylosing spondylitis, Ann Rheum Dis 34:87, 1975. 12. Wilson A, Braunwald E, Issilbacker KJ: Psoriatic arthropathy of the temporomandibular joint, Oral Surg Oral Med Oral Pathol 70:555, 1990. 13. Kononen M: Radiographic changes in the condyle of the temporomandibular joint in psoriatic arthritis, Acta Radiol 28:185, 1987. 14. Wenneburg B, Kononen M, Kallenberg A: Radiographic changes in the temporomandibular joint of patients with rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, J Craniomandib Disord 4:35, 1990. 15. Miles DA, Kaugers GA: Psoriatic involvement of the temporomandibular joint: literature review and report of two cases, Oral Surg Oral Med Oral Pathol 71:770, 1991. 16 Lundberg M, Ericsson S: Changes in the temporomandibular joint in psoriasis arthropathica, Acta Derm Venereol 47:354, 1967. 17. Koorbusch GF, Zeitler DL, Fotos PG, et al: Psoriatic arthritis of the temporomandibular joint with ankylosis, Oral Surg Oral Med Oral Pathol 71:267, 1991. 18. de Viam K, Laries RJ: Update in treatment options for psoriatic arthritis, Expert Rev Clin Immunol 5:779, 2009. 19. Alstergren P, Larsson PT, Kopp S: Successful treatment with multiple intra-articular injections of infliximab in a patient with psoriatic arthritis, Scand J Rheumatol 37:155, 2008. 20. Lamazza L, Guerra F, Messina AM, et al: The use of etanercept as a non-surgical treatment for temporomandibular joint psoriatic arthritis: a case report, Aust Dent J 54:161, 2009. 21. Salvarini C, Cantini F, Olivieri I: Disease-modifying antirheumatic drug therapy for psoriatic arthritis, Clin Exp Rheumatol 20(Suppl 28):S71, 2002. 22. Wenneberg B: Inflammatory involvement of the temporomandibular joint: diagnostic and therapeutic aspects and a study of individuals with ankylosing spondylitis, Swed Dent J Suppl 20:1, 1983. 23. Wenneberg B, Hollender L, Kopp S: Radiographic changes in the temporomandibular joint in ankylosing spondylitis, Dentomaxillofac Radiol 12:25, 1983. 24. Manemi RV, Fasanmade A, Revington PJ: Bilateral ankylosis of the jaw treated with total alloplastic replacement using the TMJ concepts system in a patient with ankylosing spondylitis, Br J Oral Maxillofac Surg 47:159, 2009. 25. Kononen M: Signs and symptoms of craniomandibular disorders in men with Reiter’s disease, J Craniomandib Disord 6:247, 1992. 26. Kononen M, Kovero O, Wenneberg B, et al: Radiographic signs in the temporomandibular joint in Reiter’s disease, J Orofac Pain 16:143, 2002. 27. Harris S, Rood JP, Testa HJ: Post-traumatic changes of the temporomandibular joint by bone scintigraphy, Int J Oral Maxillofac Surg 17:173, 1988. 28. Hanson TL: Pathological aspects of arthritides and derangements. In Sarnat BG, Laskin DM, editors: The temporomandibular joint: a biological basis for clinical practice, ed 4, Philadelphia, 1992, WB Saunders, pp 165–182. 29. Lesnicar DG, Zerdoner D: Temporomandibular joint involvement caused by Borrelia burgdorferi, J Craniomaxillofac Surg 35:397, 2007. 30. Leighly SM, Spach DH, Myall RW, et al: Septic arthritis of the temporomandibular joint: review of the literature and report of two cases in children, Int J Oral Maxillofac Surg 22:292, 1993. 732 PART 6 | DIFFERENTIAL DIAGNOSIS OF REGIONAL AND DIFFUSE MUSCULOSKELETAL PAIN 31. Cai XY, Yang C, Zhang ZY, et al: Septic arthritis of the temporomandibular joint: a retrospective review of 40 cases, J Oral Maxillofac Surg 68:731, 2010. 32. Cai XY, Yang C, Chen MJ, et al: Arthroscopic management of septic arthritis of the temporomandibular joint, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 109:24, 2010. 33. Gross BD, Williams RB, DiCosimo CT, et al: Gout and pseudogout of the temporomandibular joint, Oral Surg Oral Med Oral Pathol 63:551, 1987. 34. Barthelemy I, Karanas Y, Sannajust JP, et al: Gout of the temporomandibular joint: pitfalls in diagnosis, J Craniomaxillofac Surg 29:307, 2001. 35. Suba Z, Takacs D, Gyulai-Gaal S, et al: Tophaceous gout of the temporomandibular joint: a report of 2 cases, J Oral Maxillofac Surg 67:1526, 2009. 36. Nakagawa Y, Ishibashi K, Kobayoshi K, et al: Calcium phosphate deposition disease in the temporomandibular joint: report of two cases, J Oral Maxillofac Surg 57:1357, 1999. 37. Chuong R, Piper MA: Bilateral pseudogout of the temporomandibular joint: report of a case and review of the literature, J Oral Maxillofac Surg 53:691, 1995. 38. Aoyama S, Kino K, Amagosa T, et al: Differential diagnosis of calcium pyrophosphate dihydrate deposition of the temporomandibular joint, Br J Oral Maxillofac Surg 38:550, 2000. 39. Ascani G, Pieramici MD, Fiosa A, et al: Pseudogout of the temporomandibular joint: a case report, J Oral Maxillofac Surg 66:386, 2008. 40. Laskin DM: Etiology and pathogenesis of internal derangements of the temporomandibular joint, Oral Maxillofac Surg Clin N Am 6:217, 1994. 41. Heise AP, Laskin DM, Gervin AS: Incidence of temporomandibular joint symptoms following whiplash injury, J Oral Maxillofac Surg 50:825, 1992. 42. Nitzan DW: The process of lubrication impairment and its involvement in temporomandibular disk displacement: a theoretical concept, J Oral Maxillofac Surg 59:36, 2001. 43. Nitzan DW, Samson B, Better H: Long-term outcome of arthrocentesis for sudden-onset persistent, severe closed lock of the temporomandibular joint, J Oral Maxillofac Surg 55:151, 1997. 44. Greene CS, Laskin DM: Long-term status of TMJ clicking in patients with myofascial pain and dysfunction, J Am Dent Assoc 117:461, 1988. 45. Laskin DM: Surgical management of internal derangements. In Laskin DM, Greene CS, Hylander WL, editors: Temporomandibular disorders: an evidence-based approach to diagnosis and treatment, Chicago, 2006, Quintessence, pp 469–481. 46. Dimitroulis G: A review of 55 cases of chronic closed lock treated with temporomandibular joint arthroscopy, J Oral Maxillofac Surg 60:519, 2002. 47. Carvajal W, Laskin DM: Long-term evaluation of arthrocentesis for treatment of internal derangement of the temporomandibular joint, J Oral Maxillofac Surg 58:852, 2000. 48. Kramer A, Lee JJ, Bierne OR: Meta-analysis of TMJ discectomy with and without autogenous/alloplastic interpositional materials: comparison analysis of functional outcomes, J Oral Maxillofac Surg 62(Suppl 1):49, 2004. 49. Eriksson L, Westesson PL: Discectomy as an effective treatment for painful temporomandibular joint internal derangement: a 5 year clini- cal and radiographic follow-up, J Oral Maxillofac Surg 59:750, 2001. 50. Stern D: Benign and malignant tumors. In Laskin DM, Greene CS, Hylander WL, editors: Temporomandibular disorders: an evidence-based approach to diagnosis and treatment, Chicago, 2006, Quintessence, pp 319–333. 51. Clayman L: Surgical management of benign and malignant neoplasms. In Laskin DM, Greene CS, Hylander WL, editors: Temporomandibular disorders: an evidence-based approach to diagnosis and treatment, Chicago, 2006, Quintessence, pp 509–532. 52. Laskin DM: Diagnosis and etiology of myofascial pain and dysfunction, Oral Maxillofac Surg Clin N Am 7:73, 1995. 53. Clark GT: Treatment of myelogenous pain and dysfunction. In Laskin DM, Greene CS, Hylander WL, editors: Temporomandibular disorders: an evidence-based approach to diagnosis and treatment, Chicago, 2006, Quintessence, pp 483–500. 54. Laskin DM: Etiology of the pain-dysfunction syndrome, J Am Dent Assoc 59:147, 1969. 55. Dworkin SF: Psychological and psychosocial assessment. In Laskin DM, Greene CS, Hylander WL, editors: Temporomandibular disorders: an evidence-based approach to diagnosis and treatment, Chicago, 2006, Quintessence, pp 203–217. 56. Lund JP, Donga R, Widmer CG, et al: The pain-adaptation model: a discussion of the relationship between chronic musculoskeletal pain and motor activity, Can J Physiol Pharmacol 69:683, 1991. 57. Cimino R, Michelotti A, Stradi R, et al: Comparison of the clinical and psychologic features of fibromyalgia and masticatory myofascial pain, J Orofac Pain 12:35, 1998. 58. Laskin DM, Block S: Diagnosis and treatment of myofascial paindysfunction (MPD) syndrome, J Prosthet Dent 56:75, 1986. 59. Clark GT, Minakuchi H: Oral appliances. In Laskin DM, Greene CS, Hylander WL, editors: Temporomandibular disorders: an evidence-based approach to diagnosis and treatment, Chicago, 2006, Quintessence, pp 377–390. 60. Feine JS, Thomason M: Physical medicine. In Laskin DM, Greene CS, Hylander WL, editors: Temporomandibular disorders: an evidence-based approach to diagnosis and treatment, Chicago, 2006, Quintessence, pp 359–379. 61. Ohrbach R: Biobehavioral therapy. In Laskin DM, Greene CS, Hylander WL, editors: Temporomandibular disorders: an evidence-based approach to diagnosis and treatment, Chicago, 2006, Quintessence, pp 391–402. Websites www.nicdr.nih.gov—General information, clinical trials, and sponsored research in TMJ and related areas. www.aaoms.org—General information about TMJ surgery. www.tmj.org—Advocate group that provides general information for patients. The references for this chapter can also be found on www.expertconsult.com.