Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
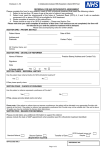
Please see reverse of form for guidance notes and where to send your referral. ORTHODONTIC REFERRAL FORM for patients with IOTN 3.6 or above who have never started a course of treatment, except when < 10 years old NHS number Patients Details Date of birth Name Address 1 Address 2 Town Sex M Age 0 Tel Mobile postcode Email Referring Practitioner Details Tel Name Practice Name Address Mobile Email NHS Town postcode Exam date Clinicians who are trained in IOTN may complete parts A,B or D then E . Those not IOTN trained should complete parts C or D then E Part A IOTN referral Enter IOTN dental health component (DHC) of patient 1 to 5 plus the qualifier a to x or in part E the clinical reason for the referral. If DHC is 3 or less go to part B or D. (see overleaf or the referral pack) Part B IOTN 3.6 referral. To qualify for treatment at the minimum IOTN level the patient must have a DHC of 3 plus an aesthetic component (AC) of at least 6 with the correct qualifier. The AC is highly subjective, so only IOTN certified clinicians should use this. Otherwise please use Parts C or D. DHC ? qualifier ? Ac ? qualifier ? (see overleaf or the referral pack) Part C Clinical referral. You must check one of the features below and give a reason for your referral in part E. A patient displaying one of the clinical occlusal traits in the list below should have a minimum IOTN (DHC) of at least 4 (see over leaf or in the referral pack). 1a Overjet >6mm 4 .Open bites>4mm but 1b if >10mm 2a Reverse overjet > 1mm with speech defects 5. Ant /post x bites with > 2mm displacement 7 Missing teeth 8 Supernumeries 10 impacted teeth inc. canines 11 infra occluding deciduous teeth or 2b > 3.5mm 3. Traumatic overbite . 6 Crowded /malaligned teeth contact point displacement >4mm 9 Non palpable permanent canines aged >9 In one or more quadrants 12. Possible surgical case Features explained over page Part D referral for advice. Please tick this box Then indicate in part E the nature of the advice required. Referral for advice is acceptable, however in such cases there must be a clinical reason which is clearly demonstrated below and not patient /parent request. To support your case you should include where possible any models radiographs and photographs taken. Please attach as much information as possible so that the orthodontist can assess the advice needed for treatment under the NHS regulations. Part E please complete this part for all referrals. Last caries incidence >12 months ago. Current active caries No If yes, explain below management plan indicating prognosis of teeth. Confirm by checking the box that the patient does not have Confirm by checking the box that copy of the consent form has a digit sucking habit and their oral hygiene is satisfactory. All been shared with the patient & parent /guardian and they are able to the necessary prevention and advice indicated in Delivering comply with the conditions.They should understand what is generally Better Oral Health has been provided and that continuing care involved in orthodontic treatment and treatment is not guaranteed by will be offered. this referral. Relevant medical history Clinical reasons from parts A B C or D, comments on caries, oral hygiene and any additional information . Orthodontic Specialist Referral Centre Address 1 Address 2 Town I have read and understood the guidance notes for referral of this type Practitioner’s signature or Performer number postcode Date Please ensure all required sections are completed, attach a medical history form (child version) if necessary, relevant radiographs and any additional letter or information you may wish to include Electronic referral form O.R.F. e V 3.9 Designed by B. Hayes Aug 2015 Please note this orthodontic referral form is limited to patients who have never had a previous course of NHS treatment, except when under the age of 10. You must obtain prior approval from NHS England before referring patients currently in treatment or those who have already received orthodontic treatment under the NHS regulations Where to refer: A referral must be made in accordance with the Strategic Framework for Orthodontics (2015). An assessment of the complexity of the case made and referred to a provider of the appropriate skill level and facilities for the procedure. Please use the chart below to determine the most suitable orthodontic provider. You will need to give the patient a choice of all orthodontic providers including their waiting times in order that the patient /parent can chose a provider within the appropriate level Complexity Level 2 Primary care specialist practice or general practice Level 3a Primary care specialist practice Procedure Straight forward interceptive measures; removable appliances, non-complex fixed appliance alignment for patients without skeletal discrepancies or significant anchorage demands. Provider Orthodontist on specialist list or GDP with additional orthodontic skills Routine orthodontic treatment of skeletal discrepancies with removable functional and fixed appliances. Restorative and surgical problems including impacted teeth where an interdisciplinary liaison approach can be managed in specialist practice Orthodontist on specialist list Level 3b Hospital consultant service Patients in the developing Patients severe skeletal disproportion or Patients inwith the developing craniofacial syndromes, complex restorative or surgical procedures requiring a multi-disciplinary approach. Patient with medical developmental, social or psychological concerns not suitable for specialist practice. Consultant orthodontist or orthodontist on specialist list Where possible level 2 and 3a complexity should be delivered in primary care and training setting, 3b delivered primarily in a hospital. A more detailed description of the complexity levels and provider descriptors can be found in the Strategic Framework for Orthodontics. Part A IOTN referral dental health component (DHC). This is the preferred section for referral for those clinicians familiar with this index, as it indicates clearly the patient’s need for treatment. The DHC must be at least 3 with an aesthetic component of 6 or above to qualify for treatment under the NHS. You must also add the qualifier a to x (used to identify When to refer :Theocclusal majority of orthodontic treatment commence in nature the lateofmixed and early permanent dentition. the child needs deviant traits) or the clinical reasoncan in part E, so the the problem is identified. You can useIf part C. if you areearly interceptive treatment useinPart D stating the reasons. Patients are referred too earlyonforthe treatment not trained IOTN. The referral pack has more detailed information IOTN. they will be referred back to the referring practitioner. Patients should not be referred early in an attempt to circumvent long waiting lists, as this is unfair on other patients, already on a waiting list, who were referred at the appropriate time. The referral pack contains further detailed guidance on patient referral. Part B IOTN 3.6 referral. This section applies to patients with a DHC of 3. You must include qualifier a to x or the clinical reason in and the aesthetic component (AC) derived from comparing the patient with 12 standardised pictures. This Orthodontic treatment is part timeEconsuming, sometimes uncomfortable and requires commitment from the patient. Patients with poor oral hygiene should must be at least 6 to create the lowest referral category of 3.6 If no Performer within a practice has undertaken IOTN training not be referred until they can demonstrate appropriate levels of plaque control. It is important that you discuss the nature of orthodontic treatment with (nb for newly qualified UK graduates this is part their training) and they are not confident to provide an IOTN score, using your patient before referring them. They should be aware and of give commitment that: the colour photographs provided, Part C or D can be completed instead. It is important that all appointments are kept Part Cmust clinical referral. If you are uncertain of the IOTN, by identifying one of the clinical features listed 1 to 12 you Appliances be worn as indicated shouldmay havetake awarded the 18 patient withmonths a DHCand of atthat least 4. By adding your will reasons for the (which referralisinlikely part to D the orthodontist Treatment between and 30 a period of retention be required be for the rest of their life) canadvice confirmand a valid IOTN score to see the patient. You willtoneed advice if you feel 3.6 is applicable as the AC is not scored. Dietary oral hygiene instructions must be adhered They require a genuine interest in undertaking orthodontic treatment with fixed appliances 1a 1b The Overjet: measured from thetreatment most prominent of the four When refer: majority orthodontic can commence in incisors. the late and early to They must achieve and of maintain an excellent standard of oral hygiene andmixed be dentally fit permanent dentition. If the child needs early 2a 2b Reverse overjet: In severe cases consider referral to hospital. interceptive treatment Part Dtostating reasons. referred too practice; early for treatment will be sent back to the by referring practitioner. They they They are onlyuse entitled receivethe 1 course ofPatients treatment from one if their treatment is discontinued either patient or practice, 3) Traumatic overbite: Increased complete overbite with signs of trauma to the labial or palatal tissues. should notwould be referred early in lists, as this is unfair on other patients, already onby a waiting list, who referred only receive a an 2ndattempt course to of circumvent treatment inlong verywaiting exceptional circumstances which would be considered the Regional IFRwere Panel. The 4) Open bites Ant/Post: these must be greater than 4 mm. at the appropriate The referral pack contains further detailed guidance on was patient exceptiontime. to this would be moving a considerable distance where this notreferral. planned at the point of referral 5) Ant/ Post X bite with displacement: mandibular displacement from RCP to ICP greater than 2mm. Orthodontic patients will be required to sign a contract with the providing orthodontist. This is in the referral pack 6) Crowded / Misaligned Teeth: one or more teeth must have a contact point displacement >4mm premolar rotations do not Orthodontic treatment is time consuming, sometimes uncomfortable and requires commitment from the patient. Patients with a poor oral hygiene count. not be that referred until continue they can to demonstrate appropriate levels continuing of plaque control. It is important that you discuss the nature ofatorthodontic Itshould is important patients visit to: their for routine care. Orthodontic should besecond considered risk(third for caries and 7) Missing teeth: this relates a) dentist Hypodontia, congenitally absent teeth, commonlypatients upper laterals or premolars treatment with your consider patient before referring them and reinforce the commitment they have agreed to intherapies. the patient The contract. practitioners should Delivering Better Oral Health when considering preventative advice and use of a high fluoride molars do not count) b) Avulsed teeth or inappropriate extractions (eg space remaining due to early loss of one or more first toothpaste may be indicated (2800ppm or for older children 5000ppm) molars) It is important8)that patientsof continue to visit their dentist forteeth routine continuing care. Orthodontic patients should be considered at risk for caries and Presence supernumerary teeth: Extra causing a problem. practitioners should Better Oral Health when considering preventative adviceinand Thebyuse a high fluoride toothpaste 9) Nonconsider palpableDelivering permanent canines. If the maxillary canines cannot be palpated the therapies. buccal sulcus ageof9-10 years, may be indicated or for older children 5000ppm) should be carried out. they(2800ppm may be ectopic and further investigations 10) Impacted teeth: a) simple tipped teeth causing food packing b) moderate /severe impactions, including impeded eruption, not enough room for a tooth to erupt. Including impacted and palatal canines. Parts to D more detaileddeciduous explanations. 11) InfraAoccluding (Submerged) teeth: these may prevent the eruption of the permanent teeth. 12) Possible surgical case: for severe skeletal discrepancy, defects of cleft lip palate, craniofacial anomaly. Part D referral for advice. There are many times when orthodontic advice can aid your treatment plans for a patient, Fold -- these may include: early intervention, caries management and extractions, disorders of eruption retained or missing teeth. You will need to supply a description of the orthodontic problem and include if possible radiographs, photos and study models. The orthodontist can then decide if an assessment is necessary. If the patient qualifies for reasons in A, B or C then you could use that route, with a note about the advice required. There will be instances where the patient /parent push for a referral but the need does not meet the NHS criteria. Referral for advice under the NHS should not be made in those circumstances.