Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
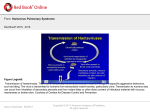
BRIEF REPORT Severe Pulmonary Involvement in a Case Attributed to Domestically Acquired Seoul Hantavirus in the United States Ingrid L. Roig,1 Daniel M. Musher,1,2 and David J. Tweardy1 1Section of Infectious Diseases, Department of Medicine, Baylor College of Medicine, and 2Michael E. DeBakey Veterans Affairs Medical Center, Houston, Texas Hantavirus is known to cause 2 distinct clinical syndromes: hemorrhagic fever with renal syndrome (HFRS) and hantavirus pulmonary syndrome. Seoul virus is an Old World hantavirus known to cause HFRS. We report a case attributed to domestically acquired Seoul hantavirus with prominent pulmonary involvement and a fatal outcome. The majority of known hantaviruses are naturally hosted by rodents (order Rodentia, superfamily Cricetidae and Muridae) as well as moles (order Talpidae) and shrews (order Soricidae) [1]. Hantavirus causes 2 known diseases in humans: hemorrhagic fever with renal syndrome (HFRS) and hantavirus pulmonary syndrome (HPS). Both syndromes share many clinical features, leading many investigators to consider them to be different manifestations of a similar pathogenic process. Seoul hantavirus is an Old World hantavirus that has been linked to a milder form of HFRS in Asia and Europe. Only 1 human case of domestically acquired infection has been described in the United States [2], although seroprevalence studies in the last decade have detected antibodies to Hantaan and Seoul viruses in domestic rats [3, 4]. Here we report a case of severe pulmonary involvement with positive serology suggestive of domestically acquired Seoul virus infection. Received 7 May 2011; accepted 13 September 2011; electronically published 31 October 2011. Correspondence: Ingrid L. Roig, MD, Section of Infectious Diseases, Department of Medicine, Baylor College of Medicine, One Baylor Plaza, BCM 286, N1319, Houston, Texas 77030 ([email protected]). Clinical Infectious Diseases 2012;54(1):91–4 Ó The Author 2011. Published by Oxford University Press on behalf of the Infectious Diseases Society of America. All rights reserved. For Permissions, please e-mail: [email protected]. DOI: 10.1093/cid/cir748 Case Report In April 2010, a 33-year-old obese hispanic male resident of Brazoria County, Texas, was hospitalized with a 7-day history of upper respiratory symptoms, nonproductive cough, pleuritic chest pain, and shortness of breath. He was in severe respiratory distress (oxygen saturation 50%) and required immediate intubation. His past medical history was unremarkable. He worked as a sandblaster and had not traveled outside Brazoria County. He denied direct exposure to rodents. His temperature was 102°F; he was hypotensive on vasopressors with a pulse rate of 120 and a respiratory rate of 36. On an oscillator machine with a fraction of inspired oxygen of 100%, his oxygen saturation was 80%. He had prominent flushing of the face, neck, and chest and coarse breath sounds, but no rashes, petechiae, peripheral edema, or ascites. Laboratory evaluation on the day of admission showed hemoconcentration, mild thrombocytopenia, hyponatremia, hypoalbuminemia, mild proteinuria, and elevations in liver enzymes, creatinine, lactic dehydrogenase, and lactic acid (Table 1). A chest radiograph showed diffused bilateral patchy opacities. His initial electrocardiogram (EKG) showed right-axis deviation with normal sinus rhythm and an isolated T-wave inversion in an inferior lead. Echocardiography showed mildly depressed left ventricular function with a normal left ventricular size and a dilated right ventricle with severe pulmonary hypertension. The patient was treated empirically with vancomycin, cefepime, azithromycin, and oseltamivir. Bacterial cultures of urine and blood were negative. Routine cultures of bronchoscopic washings were negative for bacterial pathogens. Tests for human immunodeficiency virus, Legionella, Histoplasma, and Streptococcus pneumoniae were negative. Both nasal swab for influenza A and B and H1N1 PCR were negative. Bronchoalveolar lavage fluid showed plasmacytoid and plasmablastic cells consistent with immunoblasts (Figure 1). Despite maximal oxygenation, the patient’s respiratory status worsened, his renal function deteriorated, he developed cardiac arrest, and he died 6 days after admission. Comment The sudden onset of a febrile illness with severe respiratory compromise and capillary leak syndrome in the absence of any other positive findings raised consideration of hantaviral infection. A serum sample was sent to the Special Pathogens Branch, Centers for Disease Control and Prevention, for hantavirus serologic testing. The test revealed immunoglobulin (Ig) M to Seoul hantavirus at 1:1600 dilution; IgG was undetectable, as were IgM and IgG for Sin Nombre virus. Enzyme-linked immunosorbent BRIEF REPORT d CID 2012:54 (1 January) d 91 Table 1. Laboratory Findings of a 33-Year-Old Hispanic Man a Week After Onset of Symptoms of Seoul Virus Infection Specimen On admission 3 Day 3 of hospitalization Day 6 of hospitalization Reference range 9100 14 900 21 700 90 90 89 50–70 Lymphocytes, % 5 6 1 20–40 Hemoglobin, g/dL 18.8 17.9 17 14–18 Hematocrit, % 62.1 62.7 60.3 White blood cell count, cells/mm Neutrophils, % No. of platelets/mm3 Sodium, mg/dL 114 130 156 139 202 142 Urea nitrogen, mg/dL 42 70 56 Creatinine, mg/dL 1.7 Albumin, g/dL 1.4 4.1 40–54 150–400 136–145 7–18 0.6–1.3 N/A 3.4–5.0 Alanine aminotransferease, IU/L 29 38 N/A 30–65 Aspartate aminotransferase, IU/L 106 152 N/A Lactic acid, mmol/L Fibrinogen, mg/dL Lactate dehydrogenase, IU/L Brain natriuretic peptide, pg/mL pH 1.2 6.0 4500–12 000 4.3 N/A 544.7 1206 N/A N/A N/A N/A 10 N/A N/A 7.41 7.21 1.9 7.21 15–37 0.4–2.0 180–480 100–190 0–100 7.35–7.45 pCO2, mm Hg 56 75 71 pO2, mm Hg 38 57 40 32–45 72–104 HCO3, mmol/L 35 28.6 28 22–26 11 12 12 12 Urine Protein (dipstick) Blood (dipstick) N/A N/A Negative Negative Abbreviation: N/A, not available. assay was strongly positive for IgM (optical density [OD], 3.28) and negative for IgG (OD, 0.24) to Seoul virus antigens. Autopsy showed cardiomegaly, hepatomegaly, nephromegaly, and splenomegaly with the presence of a splenic infarct; pleural, pericardial, and peritoneal effusions were noted. There were no signs of hemorrhage within the endocardium or myocardium. Microscopic review of the lung tissue showed diffuse changes suggestive of nonspecific or viral pneumonia with intra-alveolar hemorrhage and focal thrombus formation. The liver showed severe autolysis without inflammation. The renal cortex showed large glomeruli. No signs of inflammation or tubular necrosis were identified. Immunohistochemical identification of hantavirus in kidney and lung tissue was unsuccessful. An environmental assessment of the patient’s home showed evidence of rodent infestation (urine, feces). Unfortunately, no rodents were trapped and tested for Seoul infection. There were no reports of a similar illness among family members. Discussion Figure 1. Immunoblasts (white arrows) seen on bronchoalveolar lavage. Magnification 3400. 92 d CID 2012:54 (1 January) d BRIEF REPORT We believe this case is suggestive of domestically acquired Seoul hantavirus infection in the United States, showing an overlap between HPS and HFRS. Although hantaviral immunohistochemistry studies on tissues obtained at autopsy were negative, his clinical presentation, high anti-Seoul hantavirus IgM titer with a negative IgG titer, failure to detect another etiological agent, and presence of the rodent reservoir throughout Texas suggest that this case was likely caused by Seoul virus. Although there was no known prior medical disease reported in our patient, the finding of severe pulmonary hypertension on echocardiography and right-sided axis on the initial EKG may be attributable to his obese condition, causing previously undiagnosed obstructive sleep apnea and/or obesity hypoventilation syndrome, or to occupational lung disease. However, neither alone nor together would these findings explain why the patient had noncardiogenic pulmonary edema upon presentation. Our patient showed features compatible with both syndromes caused by hantavirus. His initial presentation with respiratory failure and noncardiogenic pulmonary edema, as documented by his low B-type natriuretic peptide blood test, was more consistent with HPS. His subsequent development of flushing of the skin, conjunctival injection, renal involvement, and intraalveolar hemorrhage was characteristic of HFRS. The prior understanding that Old World hantaviruses cause HFRS and are limited to the European and Asian continents has been revised in the past decade or so. Growing evidence, including this case, suggests that the syndrome caused by these strains is no longer limited to 1 syndrome or another; rather, patients infected by these strains present with varying degrees of overlap between the 2 syndromes. Seoul virus is a known Old World hantavirus that occurs across Asia and Europe [1]. Although mainly an urban disease due to the host distribution, cases have been identified among farmers and workers, as well as laboratory workers, in diseaseendemic areas. All cases of HFRS reported previously have presented with a mild to moderate form of the disease. Since 1993, 37 cases of Hantavirus have been reported in Texas [5], 6 due to Bayou strain, 29 to Sin Nombre, and, in 2 cases, to an unknown strain. This is the first reported case to occur due to Seoul virus. Rattus norvegicus and Rattus rattus are the primary rodent reservoirs of Seoul virus. These species of rats are distributed worldwide, including the United States. In the last decade, studies in limited US urban areas have shown a seroprevalence of 50%–58% [3] of Seoul virus antibodies in rats and 0.5%–1.6% [6] in humans. No previous epizootiologic and epidemiologic studies have been conducted previously in Brazoria County, although Seoul virus has been isolated from Norway rats in a neighboring county [7]. Seoul virus may cause a less severe form of HFRS clinically distinct from HPS, with a mortality rate of 1%–2% [1]. Although pulmonary symptoms have occasionally been described with other viruses causing HFRS [8–10], there has not been a case of Seoul virus showing a clear overlap between both syndromes. HFRS and HPS share some clinical and laboratory features. The earliest clinical manifestations described are headache, chills, myalgia, malaise, and a fever of rapid onset [1, 8, 11]. This is usually followed by nausea, vomiting, and abdominal pain. Respiratory symptoms, such as cough, sore throat, and dyspnea, are less commonly seen in HFRS [8] but are the primary symptoms reported in HPS [11, 12]. Microvascular instability with vascular leakage is the pathologic hallmark of both syndromes, with vascular changes occurring in the lungs in HPS and in the kidneys in HFRS. HPS is characterized by rapid development of respiratory failure and cardiogenic shock, with a mortality rate of about 35%–40% [1, 11, 12]. HFRS usually presents with various degrees of renal involvement, occasionally with frank hemorrhage, and has a mortality rate ranging from ,1% to 12%, depending on the causative virus. Pulmonary edema is not a frequent complication of HFRS [10]; when present, it usually occurs during the final stages of the disease (oliguric and diuretic phase). Laboratory findings common to both syndromes are leukocytosis with left shift, low albumin, thrombocytopenia, high hematocrit due to capillary leak, azotemia, transaminitis, and presence of immunoblasts (activated lymphocytes with plasmacytoid features) that can be seen in lungs, blood, bone marrow, liver, or spleen. There are no specific therapies available to treat diseases caused by hantavirus, with the exception of intravenous ribavirin, which has shown some benefit in the treatment of Hantaan virus infections [1]. Supportive care remains the cornerstone of management and includes early use of vasopressors, mechanical ventilation, and cautious use of intravenous fluid. Notes Acknowledgment. We thank Dr Adam Macneil from the Special Pathogens Branch at the Centers for Disease Control and Prevention for information on prior Seoul virus cases in the United States as well as for details on the serologic testing done to our patient. Potential conflicts of interest. All authors: No reported conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed. References 1. Jonsson CB, Figueiredo LT, Vapalahti O. A global perspective on hantavirus ecology, epidemiology, and disease. Clin Microbiol Rev 2010; 23:412–41. 2. Woods C, Palekar R, Kim P, et al. Domestically acquired Seoul virus causing hemorrhagic fever with renal syndrome–Maryland, 2008. Clin Infect Dis 2009; 49:e109–12. 3. Easterbrook JD, Kaplan JB, Vanasco NB, et al. A survey of zoonotic pathogens carried by Norway rats in Baltimore, Maryland, USA. Epidemiol Infect 2007; 135:1192–9. 4. Childs JE, Korch GW, Smith GA, Terry AD, Leduc JW. Geographical distribution and age related prevalence of antibody to Hantaan-like virus in rat populations of Baltimore, Maryland, USA. Am J Trop Med Hyg 1985; 34:385–7. 5. Rivers MN, Alexander JL, Rohde RE, Pierce JR Jr. Hantavirus pulmonary syndrome in Texas: 1993-2006. South Med J 2009; 102:36–41. 6. Smith HM, Reporter R, Rood MP, et al. Prevalence study of antibody to ratborne pathogens and other agents among patients using a free clinic in downtown Los Angeles. J Infect Dis 2002; 186:1673–6. 7. Yanagihara R. Hantavirus infection in the United States: epizootiology and epidemiology. Rev Infect Dis 1990; 12:449–57. BRIEF REPORT d CID 2012:54 (1 January) d 93 8. Park SC, Pyo HJ, Soe JB, et al. A clinical study of hemorrhagic fever with renal syndrome caused by Seoul virus infection. Korean J Intern Med 1989; 4:130–5. 9. Rasmuson J, Andersson C, Norrman E, Haney M, Evander M, Ahlm C. Time to revise the paradigm of hantavirus syndromes? Hantavirus pulmonary syndrome caused by European hantavirus. Eur J Clin Microbiol Infect Dis 2011; 30:685–90. 94 d CID 2012:54 (1 January) d BRIEF REPORT 10. Paakkala A, Mustonen J. Radiological findings and their clinical correlations in nephropathia epidemica. Acta Radiol 2007; 48:345–50. 11. Macneil A, Ksiazek TG, Rollin PE. Hantavirus pulmonary syndrome, United States, 1993-2009. Emerg Infect Dis 2011; 17:1195–201. 12. Khan AS, Khabbaz RF, Armstrong LR, et al. Hantavirus pulmonary syndrome: the first 100 US cases. J Infect Dis 1996; 173: 1297–303.