Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
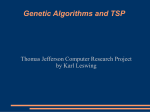
1765 CONCISE COMMUNICATION A Deletion Mutation in Region V of the Cytomegalovirus DNA Polymerase Sequence Confers Multidrug Resistance Sunwen Chou,1,2 Richard C. Miner,3 and W. Lawrence Drew3 1 Medical and Research Services, VA Medical Center, and 2Division of Infectious Diseases, Oregon Health Sciences University, Portland; 3 Departments of Laboratory Medicine and Medicine, University of California, San Francisco–Mount Zion Medical Center, San Francisco A patient with AIDS and cytomegalovirus (CMV) retinitis received ganciclovir and foscarnet for 20 and 5 months, respectively, with evidence of periodic disease progression. After this therapy, a CMV isolate from the patient was resistant to ganciclovir, foscarnet, and cidofovir. Sequence analysis showed a known ganciclovir resistance mutation in the viral UL97 phosphotransferase (L595F) and a new mutation in conserved region V of the DNA polymerase gene (pol) sequence (codons 981–982 deleted). The pol mutation was transferred to a laboratory CMV strain (Towne) by homologous recombination and selection with either ganciclovir or foscarnet. Recombinant viruses containing this deletion showed a 6–8-fold increased ganciclovir resistance and a 3–5-fold increased resistance to both foscarnet and cidofovir, compared with the wild-type CMV. A single mutation in region V of CMV pol can, therefore, confer multiple drug resistance in a clinical isolate. Although mutations in the viral UL97 phosphotransferase gene are the most common genetic basis for ganciclovir resistance in clinical cytomegalovirus (CMV) isolates [1], mutations in the viral DNA polymerase (pol) gene have recently attracted interest as potential causes of multidrug resistance [2–8]. Published data indicate that some pol mutations in codons 380–545 confer dual ganciclovir-cidofovir resistance and that other mutations in codons 696–845 confer primarily foscarnet resistance, with some also having low-grade cross-resistance to ganciclovir [2–7]. In addition, a mutation at codon 987 in conserved region V of pol was described in a CMV laboratory strain (AD169) propagated in the presence of ganciclovir [8]. The mutation conferred ganciclovir and cidofovir resistance. Here, we report another mutation in pol region V that was found in a clinical CMV isolate resistant to ganciclovir, foscarnet, and cidofovir, and we examine its phenotypic correlates by transferring it to a CMV laboratory strain. Materials and Methods Viral isolates and susceptibility testing. CMV was isolated from the semen of a subject with AIDS and CMV retinitis 20 months Received 24 May 2000; revised 10 August 2000; electronically published 17 October 2000. Presented in part: Interscience Conference on Antimicrobial Agents and Chemotherapy, San Francisco, September 1999 (abstract 1950). Financial support: Department of Veterans Affairs; National Institutes of Health (AI-39938). Reprints or correspondence: Dr. Sunwen Chou, VA Medical Center P3ID, 3710 SW US Veterans Hospital Rd., Portland, OR 97201 ([email protected]). The Journal of Infectious Diseases 2000; 182:1765–8 q 2000 by the Infectious Diseases Society of America. All rights reserved. 0022-1899/2000/18206-0025$02.00 after initiation of antiviral therapy. After a 4-week initial induction therapy with twice-daily intravenous (iv) ganciclovir, the drug was continued as a once-daily iv dose, with 2 temporary increases to twice daily for 2 weeks at 5 and 9 months when disease progressions were noted. At 15 months, therapy was changed to ganciclovir and foscarnet, which were each administered iv on alternate days; however, by the time the isolate was obtained, the retinitis had progressed, and salvage therapy was attempted with intravitreal foscarnet. CMV was isolated and propagated in human foreskin fibroblasts or lung fibroblasts. Laboratory CMV strain Towne (ATCC VR977) was used as a control for phenotypic and genotypic analyses. Susceptibility to ganciclovir, foscarnet, and cidofovir was determined by the drug concentration required to inhibit viral plaque formation in human foreskin fibroblasts cell culture by 50% (IC50) [9, 10]. The IC50 cutoff used to define resistance in clinical CMV isolates was 6 mM for ganciclovir, 400 mM for foscarnet, and 2 mM for cidofovir [9, 10]. With extracellular viral inocula from CMV laboratory strains and recombinants, susceptibility testing was controlled by a simultaneous assay of the reference Towne strain, to compensate for variability resulting from the condition of the cell cultures. The ratio of IC50 obtained for recombinant viruses versus wild-type control was used to assess the change in drug susceptibility. All assays on recombinant viruses resulting from marker transfer were done 3 times (with wild-type control), and a mean value was obtained. Genetic analyses. The entire UL97 (2.1 kb) and pol (3.7 kb) coding sequences of the clinical CMV isolate were determined from polymerase chain reaction (PCR) products of infected cell extracts, using a fluorescent dye terminator cycle sequencing kit (BigDye; PE Biosystems, Foster City, CA) and an automated sequencer (ABI 377; PE Biosystems), as described elsewhere [2, 11]. Sequence differences from reference strains AD169 and Towne (GenBank data) 1766 Chou et al. were compared with known drug-resistant mutations and interstrain variation in susceptible clinical isolates [2]. Marker transfer. The pol mutation present in the clinical isolate was transferred by homologous recombination into laboratory strain Towne. A segment of DNA from the isolate was amplified by PCR, using primers pol1507 (50-CTGGTGGCCGTGCCCGACGAC-30) and U531 (50-CGTACGGCGAATTCCAGGTCTCGCGCATCGCCTG-30), and then was digested with restriction enzymes BamHI and EcoRI to produce a 3.47-kb fragment extending from codon 340 of pol to 0.76 kb past the end of the pol coding sequence. This fragment was cloned into the Bluescript vector pBSIIKS1, and the sequence of the insert was checked for absence of sequence errors introduced during PCR or cloning. Marker transfer was accomplished using a calcium phosphate cotransfection technique, as described elsewhere [6–7, 11]. In brief, 15 mg of Towne strain viral DNA was coprecipitated with 2 mg of the EcoRI/BamHI-digested mutant cloned fragment and transfected into human fibroblast cultures. Viral cytopathology was observed at 2 weeks. Recombinant virus containing the desired mutation was selected by propagation with drug (ganciclovir or foscarnet) and then triply plaque-purified without drug. The entire 2.1-kb UL97 and 3.7-kb pol coding regions of the plaque-purified recombinant virus were sequenced and compared with Towne strain and the original clinical isolate. The virus was also tested by plaque reduction for susceptibility to ganciclovir, foscarnet, and cidofovir in parallel with the parental strain Towne. Results The posttreatment clinical isolate was highly resistant to ganciclovir, foscarnet, and cidofovir (table 1). Sequence analysis of the entire viral UL97 and pol coding sequences showed a mutation at codon 595 of UL97 (L595F), a known ganciclovir resistance marker [12], and a 2-codon deletion mutation (codons 981–982 deleted [d981–2]) in pol. The pol sequence of the isolate (GenBank AF291828) was otherwise remarkably similar to strain AD169, with only 2 other nucleotide differences and no amino acid differences. The deletion mutation d981–2 is located in conserved region V (figure 1) of the CMV pol gene near a previously reported mutation (A987G) that was associated with dual ganciclovir and cidofovir resistance in a laboratory CMV strain. Because of the location of this mutation in a conserved domain of pol, marker transfer experiments were done to confirm the phenotypic correlates of this mutation. Recombinant viruses containing the codon 981–982 deletion were produced by cotransfection of Towne strain DNA and a cloned segment of the clinical isolate containing the mutation. Because the recombination rate is low, this classical marker transfer method requires drug selection to isolate the recombinant viruses containing the putative resistance mutation. To reduce the chance that spontaneous drug-resistant point mutations would be selected, passage under drug was minimized, and separate transfection experiments were done and were followed by foscarnet alone or ganciclovir alone for recombinant selection. In one experiment, the initial supernatant virus from the JID 2000;182 (December) Table 1. Phenotypes of cytomegalovirus (CMV) isolate and recombinant strains. Virus Clinical isolate a Recombinant T1299-1-1-1 Towne control IC50 ratio T1299:control b Recombinant T1265-5-4-6 Towne control IC50 ratio T1265:control Ganciclovir Foscarnet Cidofovir 150 48 5 3 5.8 5 1.5 8.3 47 5 12 7.7 5 .08 6.1 11000 298 5 55 84 5 13 3.6 268 5 51 67 5 9.8 4.0 10.6 1.7 5 0.32 0.60 5 0.07 2.8 1.8 5 0.29 0.34 5 0.15 5.1 NOTE. Data are mean IC50 5 SD, given in mM. a Codon 981-2 deletion mutant selected under foscarnet. b Codon 981-2 deletion mutant selected under ganciclovir. transfection was propagated once each in 100, 300, and 400 mM foscarnet, after which the viral DNA showed the mixed presence of the d981–2 deletion. The virus was then triply plaque-purified, producing T1299-1-1-1. In another experiment, virus from the initial transfection culture was propagated once in 15 mM ganciclovir and 3 times in 20 mM ganciclovir, after which the viral DNA showed the dominant presence of the d981–2 deletion. The virus was then triply plaque-purified, producing T1265-5-4-6. The supernatant from 5–7-day cultures of plaque-purified T1265 and T1299 had infectivity titers of 3 3 10 6 to 4 3 10 6 pfu/mL and was used for subsequent plaque reduction assays. Sequence analyses of viruses T1299-1-1-1 and T1265-5-4-6 showed the UL97 sequence to be the same as the parental Towne strain and the pol sequence to contain the codon 981–2 deletion, with no other amino acid changes from Towne strain. At the nucleotide level, the pol sequence for both recombinants was the same as that of the Towne through codon 920. Thereafter it crossed over to the sequence of the clinical isolate (cloned segment) and crossed back to the Towne sequence from codon 1036 (T1265-5-4-6) or codon 1062 (T1299-1-1-1) through the end of the pol coding sequence. Plaque reduction susceptibility testing of the recombinant viruses showed a 6–8-fold increased IC50 for ganciclovir and a 3–5-fold increased IC50 for cidofovir and foscarnet, compared with a simultaneous Towne strain control (table 1). The 2 recombinant viruses had the same phenotypes, despite having been selected under different drugs (ganciclovir or foscarnet). Discussion A single region V pol mutation was associated with multiple drug resistance in a clinical CMV isolate, and transfer of the mutation to a laboratory strain confirmed that it conferred decreased susceptibility to all 3 of the currently licensed systemic anti-CMV drugs. The mutation was found in a patient who had not responded well to prolonged ganciclovir therapy, which had been combined with foscarnet in the last several months of treatment. It supports the conclusion that mutations in the CMV pol gene can confer a variety of phenotypes, in- JID 2000;182 (December) CMV DNA Mutation and Multidrug Resistance 1767 Figure 1. Drug-resistant mutations in cytomegalovirus (CMV) DNA polymerase gene. Shown are codon ranges corresponding to conserved functional domains, locations of known resistance mutations in clinical CMV isolates [2, 4–7] (authors’ unpublished data), and the associated drug susceptibility phenotypes. CDVr, cidofovir resistant; GCVr, ganciclovir resistant; PFAr, foscarnet resistant; wt, wild type. cluding cross-resistance to drugs to which the patient has not been exposed. Region V was the first locus in the CMV pol gene to be linked to ganciclovir resistance. A codon 987 mutation (A987G) was found in a laboratory strain (AD169) serially propagated with drug [8], and we subsequently observed the same mutation in 2 clinical isolates (authors’ unpublished data). Marker transfer [5, 8] of the A987G mutation conferred a 4–6-fold increase in ganciclovir resistance and an 8–11-fold increase in cidofovir resistance; no foscarnet resistance was observed [5]. The present deletion mutation at codons 981–982 in the same conserved region likewise confers ganciclovir and cidofovir resistance, and we additionally documented resistance to foscarnet by marker transfer. Although the degree of resistance transferred to the Towne strain was modest (3–4-fold), it may well be clinically relevant, because the patient had been treated with foscarnet and ganciclovir with suboptimal response. The mutant laboratory strains also propagated well under 400 mM foscarnet, a property not observed with the wild-type Towne or AD169 CMV strain. After cotransfection of wild-type and mutant viral DNA, the mutant viruses were selected with ganciclovir or foscarnet alone, but they had closely similar crossresistances to both drugs, regardless of which one was used for selection in culture. This makes it less likely that the observed cross-resistances were an artifact of the drug used for culture isolation of the recombinant. The foscarnet and cidofovir IC50 values for the clinical isolate were higher than that of the recombinant virus containing the d981–2 mutation. This raises the possibility that some other viral genetic factor besides the pol mutation enhances the multidrug resistance of the clinical isolate. However, differences in IC50 values for the same drug, between resistant clinical isolates and the corresponding mutant laboratory strains, have been observed regularly in marker transfer studies [3–8, 11]. IC50 values obtained with cell-associated clinical CMV isolates may not be directly comparable with values obtained with extracellular viral stocks of laboratory CMV strains. For example, mutations at pol codons 700 and 715 that have been linked to clinical foscarnet resistance conferred foscarnet IC50 values 180– 210 mM (an ∼5-fold increase) when transferred to strain AD169 [4]. Yet, many baseline clinical isolates have foscarnet IC50 values in this range, whereas most resistant clinical isolates have foscarnet IC50 values 1 400 mM [10]. There is continued interest in studying drug-resistant mutations in the CMV pol gene as a guide to functionally significant domains and as a means of focusing the genotypic testing of anti–viral drug resistance. Region V is normally very highly conserved among clinical isolates [2], but the finding of 2 drugresistant mutations within this region suggests that it may be permissive of sequence variation that confers drug resistance while maintaining normal viral replication. Viruses containing the d981–2 mutation had the normal cytopathology of CMV and produced high-titer cell-free stock 5–7 days after inoculation; there was no evidence of the slow-growth phenotype that has been observed with some other pol mutations (e.g., at codons 700 and 715) [4]. Region V has homologies with DNA polymerases from a number of other sources, including herpes simplex virus, and may be involved in template and primer positioning [13], although no direct crystallographic data are available. Attention to region V for purposes of genotypic diagnosis of CMV resistance has been recommended [2] because of the occurrence of the A987G mutation in clinical isolates. If A987G were the only mutation requiring detection, a specific test for that mutation, such as by restriction digestion of a suitable PCR product, might be suitable, because region V is rather remote from other regions where resistance mutations are located. With the current finding of another region V mutation, it would seem prudent to use screening methods that can detect any sequence change in this region. 1768 Chou et al. Acknowledgments We thank Matthew Shiveley, Camie Meichsner, Barbara Sisson, Kevin Michels, and Gail Marousek for technical assistance. References 1. Chou S, Guentzel S, Michels KR, Miner RC, Drew WL. Frequency of UL97 phosphotransferase mutations related to ganciclovir resistance in clinical cytomegalovirus isolates. J Infect Dis 1995; 172:239–42. 2. Chou S, Lurain NS, Weinberg A, et al. Interstrain variation in the human cytomegalovirus DNA polymerase sequence and its effect on the genotypic diagnosis of antiviral drug resistance. Antimicrob Agents Chemother 1999; 43:1500–2. 3. Lurain NS, Thompson KD, Holmes EW, et al. Point mutations in the DNA polymerase gene of human cytomegalovirus that result in resistance to antiviral agents. J Virol 1992; 66:7146–52. 4. Baldanti F, Underwood MR, Stanat SC, et al. Single amino acid changes in the DNA polymerase confer foscarnet resistance and slow-growth phenotype, while mutations in the UL97-encoded phosphotransferase confer ganciclovir resistance in three double-resistant human cytomegalovirus strains recovered from patients with AIDS. J Virol 1996; 70:1390–5. 5. Cihlar T, Fuller MD, Cherrington JM. Characterization of drug resistance– associated mutations in the human cytomegalovirus DNA polymerase gene by using recombinant mutant viruses generated from overlapping DNA fragments. J Virol 1998; 72:5927–36. JID 2000;182 (December) 6. Chou S, Marousek G, Guentzel S, et al. Evolution of mutations conferring multidrug resistance during prophylaxis and therapy for cytomegalovirus disease. J Infect Dis 1997; 176:786–9. 7. Chou S, Marousek G, Parenti DM, et al. Mutation in region III of the DNA polymerase gene conferring foscarnet resistance in cytomegalovirus isolates from 3 subjects receiving prolonged antiviral therapy. J Infect Dis 1998; 178:526–30. 8. Sullivan V, Biron KK, Talarico C, et al. A point mutation in the human cytomegalovirus DNA polymerase gene confers resistance to ganciclovir and phosphonylmethoxyalkyl derivatives. Antimicrob Agents Chemother 1993; 37:19–25. 9. Landry ML, Stanat S, Biron K, et al. A standardized plaque reduction assay for determination of drug susceptibilities of cytomegalovirus clinical isolates. Antimicrob Agents Chemother 2000; 44:688–92. 10. Drew WL, Miner R, Saleh E. Antiviral susceptibility testing of cytomegalovirus: criteria for detecting resistance to antivirals. Clin Diagn Virol 1993; 1:179–85. 11. Chou S, Erice A, Jordan MC, et al. Analysis of the UL97 phosphotransferase coding sequence in clinical cytomegalovirus isolates and identification of mutations conferring ganciclovir resistance. J Infect Dis 1995; 171:576–83. 12. Wolf DG, Smith IL, Lee DJ, Freeman WR, Flores-Aguilar M, Spector SA. Mutations in human cytomegalovirus UL97 gene confer clinical resistance to ganciclovir and can be detected directly in patient plasma. J Clin Invest 1995; 95:257–63. 13. Andrei G, Snoeck R, De Clercq E, Esnouf R, Fiten P, Opdenakker G. Resistance of herpes simplex virus type 1 against different phosphonylmethoxyalkyl derivatives of purines and pyrimidines due to specific mutations in the viral DNA polymerase gene. J Gen Virol 2000; 81:639–48.