Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
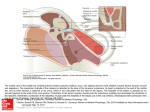
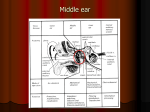
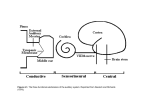
Otosclerosis Introduction - Otosclerosis : fibrous osteodystrophy of the human otic capsule - May : CHL , SNHL and mixed HL ( progressive HL ) - Cause ( suggest ) : Hereditary , endocrine , biochemical , metabolic , infectious ( eg. Measles ) , traumatic , vascular & autoimmune Embryology - At 4 th wk : otic capsule arises from mesenchyme - At 8 th wk : cartilaginous framework is begun - At 16 th wk : endochondral bone replacement BUT in some people ; complete bone replace not occur & leave cartilage frame work - Fissula ante fenestram (ant to OW ): last area bone replacement , this region is affected in 80-90% of pt Histology 3 form: 1 otospongiosis ( early phase ) : active phase มี ostetoblast , histiocyte,osteclast ซึ่ง resorb bone around preexisting bl vv ทำให้มมี vascular channel & dilatation of microcirculation ซึ่ง otoscopic exam Schwartz sign 2 transitional phase : osteocytes becomes more involve amorphous ground substance 3 otosclerosis ( late phase ) : sclerotic , dense bone Pathophysiology CHL : due to fixation of stapes footplate มักเริ่ ม involve ที่ Fissula ante fenestram นอกจำกนี้ ้ำกมีกำร involve only stapes footplate & spare annular lig ซึ่งเรี ยกว่ำ Biscuit Footplate ซึ่ง้ำกมี stapes op จะทำให้มเสี่ ยงสู งต่อ SNHL SNHL มี 3 mech : 1 toxic metabolite injury to neuroepi 2 vascular compromise 3 direct extension to cochlea Shambaugh suggest criteria to identify pt with SNHL due to OS 1 Schwartze sign in either ear 2 FH of OS 3 Unilat CHL consistent with OS & bilat , sym SNHL 4 Audiogram with a flat or cookie – bite curve with excellent discrimination 5 progress pure cochlear loss beginning at he usual age of onset for OS 6 CT show demineralization of cochlea typical of OS 7 stapedial reflex demonstrating biphasic on-off effect seen before stapedial fixation นอกจำกนี้ OS อำจมำ present ดมวย dizziness ~ 30% pt เนื่องจำกมี involve lateral semicircular canal อำกำรทำง vestibular ไม่ค่อย severe ( dizziness associate OS OS inner ear syn ) ตมอง DDX : Meniere dz , superior semicircular canal dehiscence (SSCD) Epidemiology - OS autosomal-dominant hereditary - ส่วนให้ญ่พบใหน Caucasians pt และ Associate FH ( Clayton et al. : OS ass. COL1a1 gene ) - OS advance more progress in female > male , female : male 2:1 - Age variable , HL between 15-45 yr ( ~ 33 yr ) - ใหน Juvenile OS : Dz progress than adult - Hormonal factor may play a role , clinical worsen during pregnancy History & Physical examination - OS present with slowly HL over progressive yrs - Pt มักจะไดมยน ิ เสี ยงดีใหน noisy situation ( paracusis of Willis ) - Present tinnitus ~ 75 % - Otoscopy : TM is normal in most pt , Schwartze sign may be present - Tuning fork : พบ CHL Rinne - ve Initial phase Rinne - ve may be limited to 256 Hz Progress Dz มี Footplate fixation Rinne - ve at 512 Hz & 1024 Hz ( air-bone gap ~ 10-15 dB at 256 Hz และ ~ 20-25 dB at 512 Hz Rinne – ve ) Weber test : lateralize to greater degree of CHL Audiologic testing Audiogram :Cahart notch is most common seen in OS Speech discrimination is excellent Tympanogram : Impedance can show reduce TM compliance ( type A ,As ) Stepedial reflexes : normal or abnormal depending degree of fixation ( diphasic reflex with on-off pattern , absent reflex) Vestibular test ควรจะทำใหน case with dizziness เพื่อที่จะ R/O Dz อย่ำงอื่น HRCT : assess osicular chain , bony labyrinth ซึ่ งพบว่ำมี - Early Dz : radiolucent areas around Cochlea Halo sign - Mature case : diffuse sclerosis CT scan helpful R/O middle ear Dz : mass ,vascular anomalies Differential diagnosis OS : progressive CHL or mixed HL with absence of trauma or infection , TM normal (may be Schwartze sign ) Carhart notch highly suggest OS Definite Dx : made during exploratory tympanotomy The most common conditions that mimic OS : 1. ossicular chain discontinuity : พบใหน pt with Hx of recurrent COM ซึ่งจะทำให้มมี incus necrosis , TM may be normal or thickness and sometime abnormal detected by tymanogram นอกจำกนี้พบว่ำมี A-B gap ร่ วมดมวย เนื่องจำกมี fibrous union at SI jt โดยจะพบที่ high frequency > low frequency 2. exert a mass effect on TM or ossicular chain 3. Conginital stapedial footplate fixation : พบที่อำยุ 3 ปี แต่ใหนบำงรำยอำจเพิ่ง detectไดมที่ อำยุ ~ 10 ปี juvenile OS ( De la Cruz ) 4. Malleus head fixtion : cause infection , tympanosclerosis โดยที่ malleus fix กับ epitympanum ทำให้ม immobile of all ossicle 5. Paget Dz (osteitis deformans ) : histology similar OS but Paget Dz begin involve periosteal layer & involve endochondral bone last 6. Osteogenesis imperfecta (van der Hoeve-de Kleyn syndrome) : autosomal dominant defect of osteoblast activity ซึ่ งพบว่ำมี stapes fixation & unique blue sclera ~ 40-60% Management 90 % of pt with histologic evidence of OS asymptomatic In symptomatic pt : CHL & SNHL begin at 20 yr and progress , CHL stabilize at a maximum 50-60 dB Amplification - Typical HA , bone-anchored HA (BAHA) - ใหชมใหน pt with HL & not be suitable candidate for Sx - ข้ อดี o Avoid potential risk of profound HL from Sx - ข้ อเสีย o Usually not used at night o Physical sensation of device in EAC negative sensation - In pt with severe to profound SNHL อำจใหชม cochlear impant Medical management - In 1923 Escot : first to suggest use calcium fluoride - Shambaugh use sodium fluoride for stabilize OS : fluoride ion replace hydroxyl radical form stable fluorapatite complex instead of hydroxyapatite crystal (fluorapatite complex resist osteoclast activites ) - Recommended Dose 20-120 mg per day - Evaluate efficacy : o Disappear Schwartze sign o Stabilization of hearing o Improvement CT appearance of otic capsule - Side effect : o usually minor GI irritation ( prevent : low dose , enteric coat ) o occasional complaint of jt , bone , muscle pain resolves with temporary discontinuation of therapy o Rare : fluid retention , cutaneous eruption & eye problem - 80 % pt improve or show no worsen symptoms Surgical management - Stapedectomy is indicated when the stapes fix โดยดูจำก A-B gap at least 30 dB for speech frequency & negative Rinne test at 256 , 512 Hz ( Shambaugh) - Successful stapedectomy : correct CHL , remove Carhart’snotch & closure pre-op A-B gap Factors - Age : o In the young pt พบว่ำมี anomalies of malleus or incus สูงโดยเฉพำะ congenital OS (25%)> juvenile OS (3%) o In older pt พบว่ำมี poorer result in High frequency range ้ลังจำกผ่ำตัด - Lifestyle & occupation : o Repeat exposure barometric pressure change (scuba diver) greater risk to post op fistulae , prosthesis dislocate o Pt whose work or hobbies dictate excellent balance questionable candidate for Sx o Pt whose work about taste (chef ) recommend to amplification because risk to stretching or cutting chorda tympani n. - Otologic problem o Meniere Dz & OS : greater risk of cochlear HL after stapedectomy o TM perforate & OS : shoukd be closure TM befofre stapedectomy and พบว่ำ incidence SNHL ค่อนขมำงสูง after stapedectomy o Severe Eustachian tube dysfunction & cholesteatoma : not good candidate for stapedectomy Contraindication( Shambaugh) - Poor speech discrimination & Hx of vertigo in recent month (because possibility of endrolymohatic hydrop labyrinth open) - Pt with only hearing ear should be avoid (relative) - Pt with ME infection or effusion (absolute) Technique of stapedectomy Preoperative preparation 1 patient counseling - option : observation , fluoride use and trial hearing aid - Pt must be informed of risk ot stapedectomy o Post op deafness of less than 2% o Stretching or contusion chorda tympani alteration test ( symptom can self limit & disappear in a few wk or month ) o Dehiscence of fallopian canal over OW จะทำให้มมี expose or prolapsed Facial nerve risk to injury o Post op TM perforate ~ 2% o Acute balance disturbance is common after stapedectomy , can resolve in 3-7 days , long term is rare 2 Anesthesia - can be perform under LA or GA - LA : slightly less bleeding & can assess intraoperative hearing - GA : pt prefer - The EAC is infiltrated with 1% lidocaine with 1 :100,000 epinephrine for hemostasis Operative 1 obtaining the tissue graft - autograft tissue used to cover the OW o vein ; harvested from back of hand o fat ; harvested from ear lobule o Temporalis fascia ; harvested through a small incision above & behind ear o Perichondrium ; harvested from tragus 2 Exposure of the OW - Flap is elevated from 6 o’ clock to 12 o’ clock - Special care : separated the attachment of posterior fold of pars tensa to mid point of sulcus posteriorly - In most ears, to gain exposure OW & stapes scutum ( medial most posterosuperior EAC wall ) is removed 3 1 2 3 4 1 2 3 Removal of the Stapes Superstructure separate SI jt , using angled jt knife cut stapes tendon , using middle ear scissor remove superstructure : 3 technique o In footplate is rigidly fixed : fracture downward using sharp pick in the cup in head of stapes ( Fx at base of crura ) In some surgeon create safety hole at footplate prior Fx o Using a microcrurotomy bur in microdrill to sever crura o Using Argon or CO2 laser vaporize superstructure Footplate removal and Creation of a Fenestra : 3 option total footplate removal o mucosa is removed from footplate & surrounding bone o create small hole at central footplate using fine pick or laser and then footplate cut across o Removed piece of footplate , avoid dropping fragment into vestibule or aspirate perilymph Posterior half footplate removal o Similar to total footplate removal but only Posterior half is removed o Less postoperative vertigo and better high frequency hearing Small fenestra stapedectomy (stapedotomy) o Using Argon or CO2 laser , micropick , microdrill o Create hole ~ 0.7 mm diameter for ideal prosthesis ~ 0.6 mm diameter o Laser creating a rosette of opening Stapedotomy Stapedectomy 5 Tissue Seal of the Oval Window o Tissue seal : vein , perichondrium , fascia o No living tissue : Gelfoam 6 Prosthesis Placement categorize prosthesis into 4 group : 1 Cup piston prosthesis of Shea & Robinson prosthesis 2 Original Shea Teflon piston prosthesis 3 McGee/Fisch-type piston prosthesis 4 House wire prosthesis 1 2 3 4 Postoperative care Given adequate analgesic Avoid straining or blowing nose Antibiotic are not routine Keep dry ear until healing TM Special Problem During & After Stapedectomy Floating Footplate Problem - nonfixed stapedial footplate after the crural arches have been Fx - Removing floating footplate : use diamond drill or laser at promontory edge of OW Small Rt angle hook to lift footplate - If footplate depress into vestibule graft & prosthesis place lat to depressed footplate Obliterate Otospongiosis - occur at margins of OW drill out is required - approximate locate OW by crura & fallopian canal - Use small diamond drill , Argon or CO2 laser is carefully thinned down unltil blue area and made round opening Biscuit Footplate - the thickened footplate with well-defined margins produced by a primary focus in footplate - Use small diamond drill , Argon or CO2 laser cut across center until foot plate can be extracted in 2 piece Dehiscent , Prolapsed Facial nerve - facial nerve protruding down over the footplate - a small fenestra can be made in the footplate - more difficult & dangerous problem to revision stapedectomy ( become embedded & pull down by fibrosis ) Postoperative Granuloma - granuloma develop within the first 2 wk postop cause sudden hearing loss & disturbance of balance - Hallmark finding: grayish-red mass in the posterosuperior quadrant of TM - Should be explore & remove and then cover by living tissue - Early operation can save hearing Fixed incus and / or Malleus - Ankylosis of incus and / or Malleus occur by itself or combine stapes - Prolong fixed stapes Ankylosis of incus and / or Malleus - Should be correct Fixed incus and / or Malleus : o If body incus & not malleus fix separate incus from head stapes & remove o If head malleua & not incus fix cut neck malleus & remove head malleus o If both body incus&head malleus fixremove both and then insert TORP o If incus and/or malleus,not stapes fixremove then insert PORP TORP PORP Round Window Closure - Partial involvement of margin of round window is common - Tiny opening of RW or may be fibrous occlude RW but not disturb hearing - Complete bone closure RW with stapes ankylosis cause severe MHL ; Stapedectomy can improve hearing , Attempt open RW should be avoid Fracture of the Long Process of the Incus - reconstruction by TORP with wire Acut otitis media - immediate postoperative period - culture & appropriate ATB - post op TM perforate should be treated by ATB & rare require Sx repair Perilymph Gusher ; rare - profuse flow of perilymph when open vestibule อันเนื่องจำก abnormal of cochlear aqueduct and / or IAC - elevate head of table to reduce pressure, usually stop flow of perilymph - seal OW by tissue graft and then place prosthesis - bed rest and elevate head 30 degree until dry ear 24hr - may be lumbar drain is placed - complicationmay permanent cochlear loss - further operation on this ear or other ear contraindication Facial palsy - facial paralysis of Bell’s palsy can occur 5-7 d after stapedectomy owing to activation of Herpes infection - in most case recovery in one to several wk - Postoperative facial palsy treat with large coticosteroid as idiopathic Bell’s palsy - Decompression of nerve might be indicate in rare case Postoperative Perilymh fistula - rare ; cause immediate &late cochlear loss - symptom: endolymphatic hydrop - should be explore ME , avoid enter to vestibule - found fistulae and then seal by CNT graft - prognosis : vertigo is favorable ; hearing is poor - Perilymh fistula is more common after wire& Gel foam or wire fat stapedectomy Postoperative Follow-up - 2-4 wk post op good fain in hearing & discrimination - Best level of hearing ~ 3 mo-1yr (evaluate by audiogram) THANK YOU BY PORNTHAPE KASEMSIRI Aj SUTHEE , Advisor Ref : Bailey 4th edition , Glasscock-Shambaugh 5th edition