Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
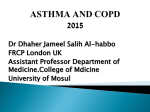
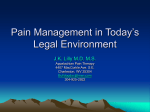
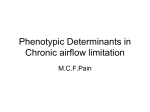
AD_HTT_029_036____AUG20_04 13/8/04 10:42 AM Page 29 How to Treat pull-out section read online @ www.australiandoctor.com.au You can now earn CPD points with How to Treat by completing quizzes online (www.australiandoctor.com.au/cpd) or in every issue. See page 36 for details and this week’s quiz. INSIDE Measuring oxygen levels in the body Normal and deficient oxygen levels Investigations Oxygen delivery systems Cost and practical advice The author Associate Professor Matthew T Naughton, head, general respiratory and sleep medicine, department of allergy, immunology and respiratory medicine, Alfred Hospital and Monash University, Victoria. Oxygen therapy Background IN 1674, John Maylow observed the death of a mouse in a sealed bell containing a burning candle, thus identifying the importance of hypoxia. In 1775, Joseph Priestly observed a candle’s flame was dependent upon ‘phlogiston’ and would not burn in the presence of ‘dephlogisticated air’. He concluded that “pure air might be peculiarly salutary to the lungs in certain morbid cases”. In 1895, liquid air became available and, later, oxygen was used to treat chlorine poisoning in WWI. Oxygen became a therapeutic tool in the 1920s, with the work of Dr Alvan Barach, who recognised the association between hypoxaemia and the oedema of right heart failure, and the benefits of oxygen therapy in patients with COPD. In the 1960s, long-term oxygen therapy was observed to reverse polycythaemia. In the 1980s, two landmark papers on use of this type of therapy in COPD were published (see page 32), cementing its use in severe COPD. Since then, the indications have broadened to other causes of hypoxia-related dyspnoea, although the weight of evidence in favour of its use for such causes is not great. At sea level, the air we breathe contains 21% oxygen, with the balance mainly as nitrogen. It exerts a pressure of 1 atmosphere, or 760mmHg. A pressure gradient of 713mmHg (760 minus water vapour pressure of 47mmHg) drives oxygen across the pulmonary alveolar membrane into the pulmonary capillary. This occurs in the first third of the 0.75 second transit time that deoxygenated hypercapnic blood has in contact with aerated alveoli. www.australiandoctor.com.au 20 August 2004 | Australian Doctor | 29 AD_HTT_029_036____AUG20_04 13/8/04 10:42 AM Page 31 How are oxygen levels in the body measured? The oxygen-dissociation curve The oxygen dissociation curve summarises the relationship between the PaO2 and the SaO2 or SpO2 (figure 1). The curve may shift to the right, aiding the unloading Figure 1: Oxygen dissociation curve. Note that a shift of the curve to the right, which aids oxygen unloading from the haemoglobin molecule, occurs with fever, acidosis, polycythaemia (higher 2,3 DPG levels) and hypercapnia. A PaO2 level of about 60mmHg should equate to an SaO2 of 90%. Figure 2: Sampling arterial blood gases. A: Allen’s test to ensure both radial and ulnar arteries are patent. B: Collection of sample with a 25-gauge needle. A 100 Oxyhaemoglobin saturation (Sp02, %) IN the blood, oxygen levels can be measured directly by arterial puncture, as either partial pressure of oxygen dissolved in arterial blood (PaO2 [in mmHg]), or as the oxygen saturation of arterial haemoglobin (SaO2 [%]). The association of PaO2 and SaO2 is illustrated by the oxygen dissociation curve (figure 1). Indirectly, oxygen levels can be measured by pulse oximetry, as oxygen bound to haemoglobin (SpO2 [%]). Arterial blood gases are usually measured from samples taken from the radial artery after an Allen’s test to ensure both radial and ulnar arteries are patent (figure 2). The sample is collected with a 25-gauge needle into a vented heparinised syringe. Local anaesthetic can be used to minimise discomfort during collection of the sample. After collection it is important to evacuate air from the syringe, which is then capped and mixed to ensure the sample is mixed with heparin. Sampling of arterial blood gases provides additional information about oxygen levels, such as PaO2, SaO2, PaCO2 and pH. Usually, levels of blood glucose, bicarbonate and haemoglobin varieties (carboxyhaemoglobin and methaemoglobin) can also be measured with this sample. Pulse oximetry (figure 3) is an indirect and non-invasive means of measuring the percentage of haemoglobin bound to oxygen (SpO2). This portable device uses a detector placed on the finger or an ear lobe to measure the absorption of two wavelengths of light (by oxyhaemoglobin and reduced haemoglobin) from two light-emitting diodes during a pulse wave across arterialised blood in a capillary bed. The proportion of oxygensaturated haemoglobin molecules relative to the total available haemoglobin molecules provides the SpO 2 value as a percentage. This measures functional saturation and ignores abnormal haemoglobin species such as carboxyhaemoglobin and methaemoglobin. Oximeter data are robust and stable and, provided they display a crisp waveform with a pulse that matches the ECG, reasonably accurate readings can be obtained. Hypotension, darkly painted finger nails, dyes (methylene blue), hyperbilirubinaemia and movement artefact can provide false readings. 80 60 40 20 further manipulated (beneficially or detrimentally) by centrally acting drugs such as narcotics, and vasoactive drugs such as salbutamol. Common medical conditions that alter VQ matching are COPD, pneumonia, post-operative atelectasis, bronchiectasis, pulmonary embolus and cardiogenic pulmonary oedema. Low levels of oxygen therapy, such as 1-2L/min, easily correct this form of hypoxaemia. 0 0 20 40 60 80 Diffusion impairment 100 Partial pressure of oxygen (Pa02, mmHg) of oxygen from haemoglobin molecules in conditions such as acidosis, fever, polycythaemia (via elevated 2,3diphosphoglycerate) and hypercapnia. A left shift because of alkalosis, anaemia, elevated carboxyhaemoglobin level or hypocapnia results in oxygen being held more strongly by the haemoglobin molecule. Haemoglobinopathies can also shift the oxygen dissociation curve by altering the O2binding affinity of haemoglobin molecules. What are normal oxygen levels? In young healthy people the PaO2 and SpO2 should be 85100mmHg and >95%, respectively (figure 1). During sleep, in normal subjects values may drop to as low as 80mmHg and 95%, respectively. When is a low oxygen level of concern? Respiratory failure is defined as a PaO2 <60mmHg or SpO2 <90%. With severe stable disease, PaO2 may be as low as 45-60mmHg, and SpO2 may fall to 80-90%. With acute deterioration, these values may fall to as low as 35mmHg and 65-80%, respectively. Patients are usually unconscious when PaO2 reaches 30mmHg or SpO2 drops to 60%. Low oxygen levels can have several effects (table 1). Acute hypoxaemia results in confusion, dyspnoea, loss of consciousness, and elevation in pulmonary and systemic blood pressure. Chronic hypoxaemia results in pulmonary hypertension, right heart failure (cor pulmonale) and secondary polycythaemia. Causes of low oxygen levels Hypoxaemia arises from five possible causes: ■ Reduced fractional inspired O2. ■ Hypoventilation. ■ Perfusion/ventilation inequality. ■ Diffusion impairment. ■ Shunt effects. Table 1: Effects of hypoxaemia Acute ■ Dyspnoea ■ Pulmonary vasoconstriction ■ Tachycardia ■ Diastolic dysfunction ■ Confusion ■ Poor judgment ■ Nausea, vomiting ■ Loss of consciousness Chronic ■ Right heart failure ■ Cor pulmonale ■ Polycythaemia Inhalation of hypoxic air Hypoxaemia from the inhalation of hypoxic air (or gas) occurs most often when people are trapped in enclosed containers with poor ventilation or ‘hyopoxic air’. Another cause is exposure to hypobaric air at high altitude. To restore normal oxygen content, the inspired oxygen concentration should be increased to more than 21% by the use of supplemental oxygen cylinders or by increasing the partial pressure (by descending to lower altitude). If these measures are unavailable, pulmonary oedema may result and periodic breathing (a waxing and waning pattern similar to that seen in heart failure patients with Cheyne-Stokes respiration) may develop during sleep. In such situations, acetazolamide (Diamox) may help via a diuretic effect and stimulation of ventilation through metabolic acidosis. B Shunt effects Figure 3. Two varieties of portable oximeters. A: Battery-operated Nonin 8500 pulse oximeter (Nonin Inc, Minneapolis, MN). B: Battery or electrically powered Oxypleth Pulse Oximeter with built-in memory (Novametrix Medical Systems, Wallingford, CT). A Perfusion/ventilation inequality Hypoxaemia may occur when there is an imbalance of airflow (ventilation) and blood Blood shunted from the right to the left heart chambers can avoid oxygenation and result in hypoxaemia. Such conditions include: ■ Cardiac shunts (atrial septal defect, ventricular septal defects, patent ductus arteriosus, patent foramen ovale). ■ Scleroderma. ■ Arteriovascular malformations (eg, Osler’s disease). ■ Severe liver disease. Characteristically, in patients with significant shunt, high concentrations of oxygen therapy (100% oxygen for 15 minutes) only partly improve hypoxaemia. Respiratory failure B Hypoventilation Hypoventilation in normal lungs can lead to hypoxaemia. This can occur in stroke, drug overdose or as a drug side effect, and in muscle or nerve pathology (diaphragm paresis). Such patients are best served with ventilation assistance (eg, non-invasive ventilatory support). Abnormalities of the alveolicapillary membrane function causing hypoxaemia are seen most commonly in idiopathic pulmonary fibrosis and other conditions in which there is widespread lung parenchymal disease (eg, lymphangitis carcinomatosa, Pneumocystis carinii pneumonia). Moderate-to-high concentrations of oxygen therapy (2-15L/m) are required to overcome hypoxaemia in such patients. flow (perfusion) matching in the lung (V/Q mismatch). The lungs have a remarkable capacity to maintain a precise gradient of blood and gas flow, which allows optimal exchange of oxygen and carbon dioxide. The matching of airflow and blood flow responds to gravity in different postures (upright, seated, supine, upside down) by changing the distribution of blood and gases. This delicate balance can be www.australiandoctor.com.au Respiratory failure is a clinical diagnosis that is supported by either arterial blood gases or oximetry readings. Type-one respiratory failure is defined as hypoxaemia with normal or reduced CO2 levels and in this group oxygen therapy should be trialled. Typetwo respiratory failure, defined as hypoxaemia with hypercapnia, should be treated with ventilatory assistance — either invasive, via intubation, or non-invasive, via face or nose mask — plus oxygen therapy if required. Chronicity of hypoxaemia can be gauged by pH levels on arterial blood gas analysis. Chronicity of hypercapnia can be gauged by elevated bicarbonate. Acute hypoxaemia or hypercapnia is usually indicated by the development of lactic acidosis on arterial blood gas sample (pH <7.35). A rule of thumb in respiratory failure is that if PaCO2 rises by 10mmHg, the pH falls acutely by only 0.1 and, in the long term, is compensated by a 3mmol/L rise in bicarbonate level. 20 August 2004 | Australian Doctor | 31 AD_HTT_029_036____AUG20_04 13/8/04 10:42 AM Page 32 how to treat - oxygen therapy Oxygen therapy Pressure versus concentration What are the aims of oxygen therapy The aims of oxygen therapy are to achieve normoxia (SpO 2 >90% or PaO 2 >60mmHg), reduce dyspnoea and alleviate polycythaemia, right heart failure and pulmonary hypertension. Who benefits from oxygen therapy? Long-term oxygen therapy Long-term oxygen therapy (LTOT) is defined as the use of supplemental oxygen for more than 15 hours/day, ideally 24 hours/day, usually at preset and fixed flows of 0.5-5.0L/min. COPD: Most commonly, LTOT is indicated for severe COPD in which the PaO2 is <55mmHg when awake, at rest and on optimal medical management (see Summary: optimal management of COPD, page 34). It can also be prescribed if the PaO2 is <60mmHg (or SpO 2 <90%) in polycythaemia, pulmonary hypertension or cor pulmonale. There is level-1 evidence of improved survival, reduced level of right heart failure, improved quality of life and neuropsychological functioning, improved exercise performance and maintenance of independent activities of daily living in these patients. Two trials conducted in the 1980s are the backbone 32 Pressure Indications Normobaric oxygen 1 atmosphere Dyspnoea Portable Cost Yes Inexpensive Hyperbaric oxygen 2-2.8 atmospheres Nitrogen narcosis, carbon monoxide poisoning, chronic ulceration No Expensive Cumulative survival data from the North American Oxygen Therapy Trial (NOTT) (12 vs 24 hours of oxygen) and the UK Medical Research Council (MRC) Trial (nil vs 15 hours of oxygen) trials in patients with COPD. (Adapted from Rees PJ, Dudley F. ABC of oxygen: oxygen therapy in chronic lung disease. BMJ 1998; 317:871-74). 100 O2 24 h/day 90 O2 15 h/day 80 Table 3: Indications for long-term supplemental (normobaric) oxygen Proven COPD ■ PaO2 <55mmHg or ■ PaO2 <60 mmHg with concurrent: — Cor pulmonale — Polycythaemia — Pulmonary hypertension Not proven ■ Cystic fibrosis ■ Congestive heart failure ■ Bronchiectasis ■ Pulmonary hypertension (primary or secondary) ■ Scleroderma ■ Hypoxaemic congenital heart disease ■ Sleep apnoea of support for the use of LTOT in COPD. The Medical Research Council study, published in 1981, studied patients with an FEV 1 of 0.7L, modest pulmonary hypertension (a mean pressure of 34mmHg), PaO2 of 50mmHg, and PaCO 2 of 55mmHg.1 Thirty of the 45 subjects in the control group who had no oxygen therapy died, compared with 19 out of 42 in the active group treated with oxygen 15 hours daily. The predicted five-year survival in the control group was only 18% and the average annual percentage mortality risk was 30%, reflecting the poor prognosis of this condition. The pulmonary artery pressure was unchanged in the group on oxygen but rose by a mean of 2.7mmHg/year in the control group. The Nocturnal Oxygen Therapy Trial conducted in North America recruited patients with an FEV1 of 0.7L and pulmonary artery pressure of 30mmHg.2 The study compared 12 hours of overnight oxygen with continuous oxygen (in practice, 17.7 hours/day). Annual mortality was 21% in the overnight oxygen group compared with 11% in the continuous oxygen group. At six months the pulmonary artery pressure at rest in the continuous oxygen group had fallen slightly. The two trials were not blinded with respect to the air cylinders used but are accepted as adequate evidence that LTOT improves prognosis in COPD. The combined results of the two trials suggests that the nearer the use of oxygen is to 24 hours/day, the better | Australian Doctor | 20 August 2004 O2 12 h/day Cumulative % survival OXYGEN therapy can be delivered in two forms — as an increased pressure (>1 atmosphere) or at an increased concentration under normobaric conditions (table 2). The former, known as hyperbaric oxygen therapy, is delivered via a hyperbaric chamber at 2-2.8 atmospheric pressures with up to 100% oxygen. Hyperbaric oxygen is used to treat conditions such as nitrogen narcosis, acute carbon monoxide poisoning, gas gangrene, ischaemic skin grafts and other slowly healing peripheral limb ulcers. It is also increasingly used by sports physicians to speed recovery time for elite sportspeople with soft tissue injuries. Complications of hyperbaric oxygen therapy include barotrauma such as pneumothorax , oxygen toxicity, seizures and changes in visual acuity. Increased oxygen concentration delivered by cylinders or oxygen concentrators under normobaric conditions is the form of oxygen therapy that most medical practitioners will come into contact with. The remainder of this article refers to this type of therapy. Table 2: Oxygen delivery systems 70 Controls (no added O2) 60 50 40 30 20 10 0 O the outlook. If oxygen is used for at least 15 hours/day, the pulmonary artery pressure may fall, and at least the expected rise seems to be prevented. In addition to the improved prognosis, there are mild neuropsychological benefits and improvements in quality of life. The mechanism of this improvement in prognosis is unclear. Changes in pulmonary artery pressure are not great, and improved survival might be related to reduction in arrhythmias related to hypoxia. The effects of long-term oxygen in COPD have been extended to include other respiratory conditions, although no evidence of clear benefit exists. Other conditions: LTOT is used in many other conditions that have hypoxiainduced dyspnoea as part of their symptomatology (see table 3) but where evidence of the benefit is either lacking or negative. Pulmonary conditions include cystic fibrosis, interstitial lung disease, bronchiolitis obliterans, bronchiectasis, pulmonary hypertension and recurrent pulmonary emboli. Guidelines for eligibility are similar to those for COPD. Patients with ‘brittle’ asthma, or those with severe asthma who are geographically isolated, are considered for the provision of oxygen cylinders for emergency use while awaiting ambulance assistance. Patients with lung cancer often complain of dyspnoea, which much of the time is not related to hypoxaemia. Often it relates to weight and muscle loss, irritation of lung parenchyma (eg, lymphangitis), aspiration, fibrosis related to radiotherapy or 10 chemotherapy, or the underlying and pre-existing COPD. Obstructive sleep apnoea is not an indication for LTOT. It is best treated with positive airway pressure or other measures to alleviate the upper airway obstruction. However, on occasions when it coexists with COPD, LTOT is given with positive airway pressure during sleep. Cardiac conditions, including congenital heart disease and severe left-sided cardiac failure with chronic pulmonary oedema, may also require LTOT. Central sleep apnoea in the setting of heart failure and Cheyne-Stokes respiration may benefit from overnight LTOT. Less common indications include conservatively managed small pneumothoraces and pneumatosis coli, a condition in which small bubbles of nitrogen-filled gas form in the intestinal wall. Increased concentrations of oxygen in the blood are thought to reduce these gas bubbles. Intermittent oxygen for exercise Supplemental oxygen can be prescribed to help in the rehabilitation of non-hypoxaemic patients with lung disease who become hypoxaemic on exertion (SpO 2 <90%) and whose exercise capacity (eg, the distance walked, or time at a certain cadence on an exercise bike) improves by >50% with oxygen therapy, compared with room air. The exercise capacity is usually established in a blinded and randomised fashion, with nasal cannulae (connected to air or oxygen), an oximeter and exercise (treadmill [sixminute walk], shuttle test or www.australiandoctor.com.au 20 30 Time (months) 40 exercise bike). Oxygen for air travel During long flights, cabin pressure may drop to the level equivalent to an altitude of 2400 metres (about 8000 feet), analogous to an inspired oxygen concentration of 15% at sea level. Patients with respiratory and/or cardiac compromise may be at risk of hypoxaemia on such flights. Risk of hypoxaemia can be assessed by the hypoxic altitude simulation test (HAST), during which oxygen levels are observed while the subject breathes a gas mixture of 15% oxygen, with the balance as nitrogen, for 5-15 minutes in an oxygen hood. Depending on the equipment used, supplemental oxygen requirements can also be assessed. Airlines need to be contacted well in advance if oxygen therapy is required during flight. Most airlines require medical clearance forms to be completed before accepting carriage of the passenger. The airlines provide cylinders for international flights. For domestic flights, passengers can provide their own oxygen (checked before departure by airline engineers), although some domestic airlines also provide oxygen. Depending on the length of the flight, purchase of an additional seat may be required to carry the oxygen cylinders. Most patients with stable respiratory disorders already on LTOT do not need additional flow rates for air travel. Oxygen at night Patients with significant nocturnal hypoxaemia, as determined by continuous pulse 50 60 oximetry or sleep studies, may benefit from LTOT. In patients with COPD but no daytime hypoxaemia or sleep apnoea, nocturnal oxygen over three years has been found to reduce pulmonary artery pressures but not alter survival. In general, if hypoxaemia (SpO 2 <90%) occurs for more than 5% of the night in the absence of sleep apnoea or hypercapnia, supplemental nocturnal oxygen can be considered. Nebulisers Nebulisers for use with bronchodilators can be either electrically or gas driven. Gas-driven nebulisers require about 4-8L/min gas flow to operate. Usually, high-flow air is preferable to drive nebulisers, particularly in the case of patients with COPD, in whom avoidance of oxygen-induced hypercapnia is the aim. Patients with life-threatening asthma may run their nebulisers with high-flow oxygen. Contraindications to oxygen therapy Contraindications to oxygen therapy include: ■ Patients with dyspnoea in the absence of hypoxaemia. ■ Current smokers. ■ Inadequately treated patients (such as those using insufficient doses of bronchodilators). ■ Heart failure (untreated or yet to be excluded). ■ Patients insufficiently motivated to undertake the discipline required in oxygen therapy. Carbon monoxide has an affinity for haemoglobin 240 times greater than that of oxygen, so high blood levels (associated with smoking) may take up to four weeks to abate. AD_HTT_029_036____AUG20_04 13/8/04 10:42 AM Page 33 Investigations Initial investigations INITIALLY it is important to establish the nature and severity of lung disease and determine whether it is responsible for hypoxaemia and dyspnoea. Determine whether the patient has been optimally managed and undergone pulmonary reha- bilitation. Organise an ECG, CXR, lung function tests, echocardiogram (left and right heart function and pulmonary pressures). Establish haemoglobin levels: if the patient has anaemia, this needs further investigation, because it may be the cause of dyspnoea. If they have polycythaemia, repeat the blood count after three months’ LTOT to see whether it abates, and, if successful, consider lifelong LTOT. An assessment of overnight oxygen levels may also be required. Consider pulmonary emboli if the patient is immobile. Subsequent reviews At one month, almost 50% of all patients initiated on LTOT for an exacerbation of their condition improve spontaneously with medical therapy (ie, after a course of bronchodilators, antibiotics, steroids, rehabilitation and correction of coexistent medical problems) and no longer require LTOT. An arterial blood gas measurement at this time also allows assessment of hypercapnia. An important aspect of clinical management of patients receiving LTOT is an annual review of oxygen treatment to assess ongoing requirements (via oximetry or, if required, arterial blood gas measurements), adherence to treatment and any side effects of treatment. How is oxygen delivered? LONG-term oxygen therapy is delivered via a concentrator or cylinders (figure 5, table 4). The oxygen concentrator is an electrically driven floor-standing pump that entrains room air through a molecular sieve filter and extracts nitrogen, thus providing 95-99% pure oxygen at flow rates of 1-2L/min, or 75% oxygen at 5L/min. The devices weigh 10kg, stand about 0.75m tall and are on wheels so they can be rolled about a home. They have an hour meter to allow objective assessment of adherence to treatment. In some Australian states, concessions from the electricity provider are available when they are in use. Small, easily carried batterydriven concentrators have recently become available. These devices cost about $8000 and are limited by the battery life to about one hour’s use. Oxygen cylinders contain compressed oxygen and deliver 100% oxygen at the outlet. The cylinders range in size from C to G (table 4). They have the capacity to provide high-flow pure oxygen at rates only limited by the attached regulator. Recent developments have reduced the weight of the cylinders and the overall device so that they can be easily used for mobile patients, either as a carry bag or in a trolley. Oxygen concentrators have a built-in flow meter, usually with a maximum flow-rate capacity of 5L/min. They can be set at lower maximum levels to avoid excessive flow rates. Oxygen cylinders have flow Figure 5: Oxygen concentrator (top) and C-sized cylinder on wheelchair (below). Figure 6: Gas flow regulators. From left to right: low-flow oxygen (0-2.5L/min), high-flow oxygen (0-15L/min), and high-flow air regulators (0-15L/min). Figure 7: Pulsed system oxygen-conserving device. Oxygen-conserving devices Two types of oxygen-conserving devices exist — a reservoir system, and the more commonly used pulse system (figure 7). The devices are placed between the patient and the oxygen source to ensure the oxygen is delivered only during inspiration and not wasted during expiration. They are valuable for use with cylinders, especially portable systems, where they can increase the life of a C-sized cylinder 3-7-fold (210 hours), depending on the chosen device. They can be triggered by negative pressure sensed by the nasal prongs at the nares during an inspiratory effort, so they may not trigger if the patient mouth breathes. Oxygen-conserving devices may be useful for patients with an oxygen concentrator who require higher flows than can normally be delivered (ie, >5L/min), by collecting the oxygen during the patient’s expiration. The oxygen interface Table 4: Oxygen cylinders and contents Size 3 Volume (m ) Duration of use at flow rate of 2L/min Traveller 0.3-0.6 1-2 hours C 0.55 3 hours D 1.5 11 hours E 3.8-5.2 30 hours G 7.6-8.8 48 hours meters attached to the pressure regulator (figure 6). Three flow meters are available for low (0.52.5L/min), medium (0-15L/min) or high flows (0-30L/min). Low flow rates are generally used in patients in whom oxygen induced hypercapnia is being avoided. Liquid oxygen systems are available in large hospitals and conserve space by storing oxygen in liquid form in large permanently standing structures. The oxygen is delivered from the tanks through coils, where it vaporises and flows to the wall outlets. The oxygen delivery ‘interface’ may be nasal prongs, oxygen mask, transtracheal, or nasal trough. The most common are nasal prongs, which are convenient and comfortable, with flow rates up to 6L/min, and which can be worn while eating. In patients requiring LTOT, the inspired concentration of oxygen can vary from 24% to 35% at 2L/min. Some oxygen cannulae can be incorporated into eye wear, making the LTOT less conspicuous. Simple oxygen masks are used if the required flow rate is greater than 6L/min, to avoid nasal irritation at high gas-flow rates. Masks should be avoided for flows of <5L/min, as rebreathing of CO2 may occur. Rebreathing can be prevented by making large holes on the side of the mask to allow ‘entrainment’ of room air to mix with the oxygen Masks, which can also be used with humidification, are less comfortable and can cause perspiration. In acute situations when highflow oxygen is required (eg, cardiogenic pulmonary oedema, pulmonary embolus), special Venturi masks have the capacity to control the amount of entrained air with a specific flow of oxygen, up to 40L/min. Oxygen can also be delivered by a trans-tracheal approach. A minitracheostomy is made, through which a fine bore catheter is placed long term, and oxygen directly bled into the trachea. An advantage of this system is that it can be worn inconspicuously under a shirt or cravat. Also, higher concentrations of inspired oxygen can be achieved because of the patient inhales greater amounts of oxygen. Oxygen can also be delivered to patients with large tracheostomies via tracheostomy hoods. Such patients require artificial humidification of their oxygen, because their normal humidification system is lost (as are their basic normal airway defence mechanisms, such as coughing). Humidification is rarely needed at domiciliary flow rates of <5L/min. Dryness at the nares may be relieved by the use of non-petroleum-based gels or ointments (eg, ointments made from sesame seed oil). Hazards of oxygen therapy Patient safety issues ALTHOUGH oxygen is not flammable, it is an essential component of fire, and fires will start more easily and burn more intensely in the presence of high concentrations of oxygen. Oxygen should therefore be used with extreme caution near heat sources (heaters, electric blankets) or naked flame (pilot lights, candles, smokers or open fires). Severe facial burns requiring skin grafts have been reported in COPD patients who smoke and use intranasal oxygen. Oxygen should be used in well-ventilated areas to reduce elevated concentrations. Tubing from either concentrators or cylinders is often long (about 10m) and trails behind the patient in their home, creating a tripping hazard. Patients should be educated in the safe handling of gas cylinders and concentrators by the oxygen supplier at the time of delivery. Because of the potential hazards of oxygen therapy, patients should receive continuing education on LTOT and hazard avoidance. Although fires precipitated by LTOT are rare, when Patients should be advised to treat oxygen therapy like a drug. they do occur, it is often in patients who have restarted smoking. Medical issues Patients need to be educated on the reasons for oxygen therapy, safety aspects and any new changes in technology. Patients should be advised to treat oxygen therapy like a drug, and as such be reviewed regularly. At flows as low as 24L/min (<35% concentration), oxygen therapy can be associated with hypercapnia, especially in COPD patients (see Author’s case study). Such patients generally have mild stable hypercapnia that is exacerbated by the acute application of high-flow oxygen. The mechanisms for developing acute hypercapnia are complex and include: ■ An increased dead space. ■ V/Q mismatch. www.australiandoctor.com.au Loss of ventilation drive. Anxiolysis and propensity to sleep (and further hypoventilate). ■ Dislodged CO 2 from the haemoglobin molecule, elevating the PaCO2 (Haldane effect). Symptoms of mild hypercapnia are blurred vision and early morning headaches, whereas severe hypercapnia causes confusion and loss of consciousness. Patients should minimise use of sedatives, narcotics, antiepileptics and alcohol if possible. Patients receiving LTOT may become housebound and develop associated psychological problems ■ ■ and social isolation. At high flow rates (eg, >60% inspired oxygen), oxygen therapy can be associated with pulmonary (atelectasis and fibrosis), cardiac and ocular pathology. Complications include ocular effects such as retrolental fibroplasia and disturbed vision, reported mainly in children and infants exposed to high concentrations of oxygen. In adults, blurred vision as well as confusion, headaches, vomiting and loss of consciousness may result from hypercapnia. Cardiac consequences are cont’d next page 20 August 2004 | Australian Doctor | 33 AD_HTT_029_036____AUG20_04 13/8/04 10:42 AM Page 34 how to treat - oxygen therapy from previous page only now starting to be identified. In patients with left heart failure, high levels (>40% or >5L/min) of inspired and blood oxygen levels result in reduced cardiac output and elevation in pulmonary capillary wedge pressure (indicating worsening heart failure). The mechanisms are poorly understood but may reflect loss of beneficial heightened chemosensitivity input to the brainstem cardiovascular control centre, or the development of oxygen radicals, which are toxic to endothelium and interfere with release of nitric oxide. Thus, any patients with congestive heart failure using devices other than normal intranasal oxygen should be closely watched for adverse effects. Consideration of ability to drive should be made on a case-by-case basis. Ideally, patients who feel breathless while driving should not attempt to drive. Detection of smoking Cigarette smoking causes many conditions that might ultimately require LTOT. Unfortunately, many addicted patients are unable to quit smoking despite disabling dyspnoea. Guidelines for the provision of oxygen from government funding exclude current smokers. This is because cessation of smoking and subsequent reduction in carbon monoxide binding to haemoglobin molecules results in greater capacity for oxygen carriage (which might take four weeks) and often results in near normalisation of PaO2 and SpO2 level, thus negating the need for LTOT. Obviously, smokers in the household of a patient receiving oxygen therapy present a fire risk. Evidence of smoking can be established by measuring carboxyhaemoglobin in arte- rial blood gases (normal <0.1%; exposure to smoke, car fumes, passive smoking 0.1-5%; smokers >5%). Alternatively, a spot urine test can be analysed for cotinine, a byproduct of nicotine. False-positive urinary cotinine result may occur in the presence of nicotine replacement therapy (patches or gum) or exposure to highconcentrate passive smoke. Cost and practical advice Set-up OXYGEN therapy requires assessment of the patient and approval by a respiratory physician. When a patient meets the criteria for oxygen therapy, applications can be placed with the district health care service. Patients are usually provided with an oxygen concentrator and a single, back-up D-sized cylinder. Oxygen equipment is usually rented via external oxygen companies. Prices start from $90 a month for an oxygen concentrator. Concentrators cost about $2600. Rental for an oxygen cylinder with an oxygen-conserving device and trolley is about $60 a month. Prices vary from company to company, state to state, and often according to whether the equipment is government or privately funded. Some companies charge delivery fees and others charge separate refill fees for portable cylinders. Rental for an oxygen cylinder with an oxygen-conserving device and trolley is about $60 a month. Medical review Annual review is recommended to ensure adherence to oxygen therapy, maintenance of SpO2 >90% and absence of side effects (mainly hypercapnia). Equipment review Annual servicing is required by the oxygen distribution company at a prescribing physician. Standard concentrators need to be serviced about every 20,000 hours, portable concentrators about every 5000-10,000 hours. Exposure of the concentrator to water (humidity) may reduce the lifespan of the nitrogen filter. Funding for long-term oxygen therapy cost borne by the health care provider (eg, Program of Appliances for Disabled People in Victoria) at which time, usage is recorded and reported back to the Funding for LTOT is provided for patients who are medically eligible and in some cases there are asset and income criteria. Most sources impose funding limits per month per patient. Australian state funding sources include public hospitals, where Author’s case study A 48-YEAR-old man with severe smoking-related emphysema (FEV1 of about 500mL) was treated with maximal medical therapy (an anticholinergic, inhaled steroid and long-acting bronchodilator) and 1L/min oxygen intranasally. He had recently stopped smoking (negative urinary cotinine and carboxyhaemoglobin <0.1%). While driving to hospital, the patient was caught in dense traffic, inhaled exhaust fumes, developed acute bronchospasm and called an ambulance for help. He was administered high-flow oxygen (10L/min) via a standard face mask and transferred to the hospital’s emergency department. On arrival he was unconscious, normotensive and tachycardic, with an SpO2 of 99%. A CXR in emergency (figure 8) and a previously conducted high-resolution CT scan of the chest (figure 9) confirmed severe COPD without acute changes. His ECG showed sinus tachycardia. Arterial blood gases (figure 10) revealed severe type 2 respiratory failure (elevated PaCO 2 and low pH). Intubation was considered but, in view of his extremely severe COPD, he was started on non-invasive ventilatory support and his inspired oxygen reduced to a level providing an SpO2 of 90%. In four hours his conscious state improved and in three 34 Figure 8: Chest X-ray showing severe hyperinflation, as indicated by the presence of more than six ribs anteriorly or 10 ribs posteriorly. | Australian Doctor | 20 August 2004 entitlements may vary from state to state, and aids and equipment programs, for which eligibility criteria may vary from state to state. Australian federal funding sources include the Department of Veterans’ Affairs, a residential care subsidy for residents of federally accredited nursing homes or hostels, and funding through an extended aged-care in the home package. Other sources include some health insurance companies, WorkCover or the Transport Accident Commission (or state equivalent), when oxygen is required as a result of a work or motor vehicle injury, respectively. Summary The most common indication (about 75%) for long-term oxygen therapy (LTOT) is COPD. ■ Eligibility for LTOT is a PaO2 <55mmHg, or <60mmHg on room air with signs of right heart failure, polycythaemia or pulmonary hypertension, in an optimally treated non-smoking patient. ■ Oxygen concentrators are the most efficient delivery system; rental cost is about $100 a month. ■ 50% of COPD patients started on LTOT in hospital can stop after one month. ■ LTOT improves quality of life and survival in COPD. ■ Evidence to support LTOT in other conditions is limited and based on COPD data. ■ Evidence of current smoking can be obtained by finding an elevated carboxyhaemoglobin level on arterial blood gas analysis, or by a positive cotinine finding in a spot urine test. ■ Early morning global throbbing headache and blurred vision (and ultimately loss of consciousness) may result from hypercapnia. Hypercapnia can be minimised by keeping SpO2 92%, and avoiding factors that might suppress respiratory drive, such as drugs (sedatives, alcohol, antiepileptics), metabolic alkalosis (steroids, diuretics), obesity, obstructive sleep apnoea, and medical conditions such as Cushing’s syndrome and hypothyroidism. ■ Figure 9: High-resolution CT scan of chest showing severe emphysema. Figure 10. Arterial blood gas profile showing extreme hypercapnic acidosis related to hyperoxia, with improvement in respiratory failure after introduction of non-invasive ventilatory support and low-flow oxygen to keep SpO2 >90%. Optimal management of COPD ■ Stop smoking. ■ Consider alpha-1 antitrypsin deficiency. ■ Assess disease severity. ■ Search for and treat coexistent medical disorders (eg, obesity, diastolic dysfunction, anaemia, hypothyroidism, sleep apnoea). ■ Institute pulmonary rehabilitation. ■ Maximise use of inhaled anticholinergics, bronchodilators and steroids (correct technique). ■ Minimise oral steroid use (3-10 days maximum for acute exacerbation). ■ Arrange vaccination (annual influenza and five-yearly pneumococcal vaccination). ■ Consider palliative surgical procedures (transplantation, lung volume reduction surgery) in extreme cases. days he was discharged home on oxygen therapy and nocturnal non-invasive therapy. Issues of importance from this case are: ■ The brittle nature of severe COPD. The development of oxygen-induced hypercapnia. ■ The avoidance of intubation and intensive care with the use of non-invasive ventilatory support. ■ www.australiandoctor.com.au What not to miss in patients on established LTOT ■ Hypercapnia in patients using excessive LTOT flow rates. ■ Inadequate time spent on LTOT (should aim for 15-24 hours/day). ■ Development of cardiac dysfunction. ■ Progression of underlying lung disease. ■ Ongoing cigarette smoking. AD_HTT_029_036____AUG20_04 13/8/04 10:42 AM Page 36 how to treat - oxygen therapy GP contribution Case study DR MARTINE WALKER Mosman, NSW JIM was a 73-year-old retired historian. Our practice inherited Jim after the departure of his long time GP to the north coast. He had never smoked but by the time I met him Jim had severe emphysema from alpha-1 antitrypsin deficiency. He was a veteran who had served in the New Guinea jungles in WWII. He had a devoted wife and two married children. Despite maximal medical therapy including anticholinergics, steroids, beta-agonists and antihypertensives, Jim’s deteriorating respiratory function became evident as he found even the smallest exertions exhausting. He began waking with headaches, presumably because of hypoxia. After assessment by a respiratory physician, which included arterial blood gases, Jim was found to fit the criteria for home oxygen, which he used initially for 16 hours a day. With his motor scooter, which was eventually supplied by the Department of Veter- ans’ Affairs, Jim was a familiar site around our area — oxygen cylinder on board. He became frustrated with the limitations in mobility associated with his portable oxygen cylinders. He was particularly put out that he could no longer commute to the university, where he had continued to be involved with research. Airlines were particularly unco-operative in Jim’s attempts to attend conferences, cylinders in tow. After two years on oxygen Jim developed a lower respiratory tract infection, which was initially thought to be a reactivation of TB. After a distressing hospital stay, Jim requested that all supports be withdrawn. He died peacefully at home with his wife and children around him. Questions for the author Assuming LTOT will have an increasing role as the community ages, are there any impending advances to make LTOT less intrusive on daily life? Smaller lighter oxygen cylinders and concentrators have been, and will continue to be, developed. Small tracheostomies with a single cannula can be used (‘minitrach’), which can be quite inconspicuous with a collared shirt or cravat. Unfortunately, there is a considerable extra cost and risk associated with minitrachs, which limit their general use. Clearly, discussion assessing quality versus quantity of life need to be conducted as part of the palliative care aspects of end-stage lung disease. In such patients who are comfortable without supplemental oxygen, the use of oxygen should be reassessed. Patients in our practice find crusting of their nose and dryness of their airways significant problems in their use of LTOT. What hints do you have to solve these and the other practical problems associated with LTOT? For oxygen flow rates < 3L/min, humidifiers are not required. Crusting for the nose can best be treated with non-petrochemical topical gels such as sesame seed oil (eg, Nozoil, distributed by ENT Technologies Pty Ltd, West Perth), RoEzit gel (available from BOC Gases, Australia) or saline nasal sprays. Could you comment on the use of LTOT in children (eg, premature babies who have had long periods of ventilation). How long on average do they require oxygen therapy? Are there any special issues or concerns with respect to LTOT in babies? I am not a paediatrician and do not look after such patients. However, in general, most paediatricians would be concerned about the toxic side effects of medium- to longterm moderate-to-high flow oxygen (retrolental fibroplasia and pulmonary toxicity). However, these toxic side effects are problematic with flows used in intensive care wards, rather than the flow rates seen in the ambulatory patient population. Further reading available on request References 1. Report of the Medical Research Council Working Party. Long-term domiciliary oxygen therapy in chronic hypoxic cor pulmonale complicating chronic bronchitis and emphysema. Lancet 1981; 1:681-86. 2. Nocturnal Oxygen Therapy Trial Group. Continuous or nocturnal oxygen therapy in hypoxaemia chronic obstructive lung disease. Annals of Internal Medicine 1980; 93:391-98. Online resources The BOC Group: www.boc.com Air Liquide Australia Limited: www.airliquide.com.au Acknowledgement Ms Brigitte Borg, respiratory scientist, Alfred Hospital, for reading the manuscript and adding valuable and practical comments. Australian Doctor How To Treat CPD Instructions Earn 2 CPD points by completing this quiz online or on the attached card. Mark your answers on the card and drop in the post (no stamp required) or fax to (02) 9422 2844. For immediate feedback click the ‘Earn CPD pts’ link at www.australiandoctor.com.au Note that some questions have more than one correct answer. The mark required for CPD points is 80%. Your CPD activity will be updated on your RACGP records every January, April, July and October. 1. Pulse oximetry measures the percentage of oxygen bound to haemoglobin (SpO2). Which ONE statement about pulse oximetry and the assessment of SpO2 is false? a) Respiratory failure is present if SpO2 is <90% . . . . . . . . . . . . . . . . . . . . . . . . . . . . .❏ b) Abnormal haemoglobin varieties (eg, carboxyhaemoglobin and methaemoglobin) can be assessed by pulse oximetry . . . . . . . . . . .❏ c) Pulse oximetry is an indirect and noninvasive method of assessing oxygen levels in the body . . . . . . . . . . . . . . . . . . . . . . . . . . . .❏ d) The presence of hypotension may make the measurement of SpO2 inaccurate . . . . . . . . .❏ 2. Brian, 65, is a heavy smoker. He has had COPD for some years and is now housebound. Coexistent medical disorders have been excluded. To optimise Brian’s management, which ONE action are you least likely to take? a) Give annual influenza vaccination and fiveyearly pneumococcal vaccine . . . . . . . . . . . .❏ b) Perform pulmonary function tests . . . . . . .❏ c) Advise him to use regular oral steroids . . . . . . . . . . . . . . . . . . . . . . . . . . . . .❏ d) Encourage him to participate in pulmonary rehabilitation if this is available locally . . . . . .❏ HOW TO TREAT 3. Brian claims he will stop smoking if oxygen is provided to improve his symptoms. He understands that there is no government funding for oxygen if he continues to smoke. Which ONE statement concerning carbon monoxide and smoking is true? a) Carbon monoxide has an affinity for haemoglobin 10 times greater than that of oxygen . . . . . . . . . . . . . . . . . . . . . . . . . . . . .❏ b) High carbon monoxide levels rapidly decrease over five days after cessation of smoking . . . . . . . . . . . . . . . . . . . . . . . . . . . .❏ c) PaO2 and SpO2 may be nearly normalised after smoking cessation . . . . . . . . . . . . . . . .❏ d) Measuring arterial blood gases is the only way to check that he has stopped smoking . . . . . . . . . . . . . . . . . . . . . . . . . . . .❏ 4. Brian’s PaO2 on maximal inhaled therapy is 58mmHg. He has not smoked for six weeks and this is confirmed on measurement of arterial blood gases. Under which THREE circumstances could Brian receive government-funded long-term oxygen therapy? a) Polycythaemia . . . . . . . . . . . . . . . . . . . . . .❏ b) Pulmonary hypertension . . . . . . . . . . . . . .❏ c) COPD . . . . . . . . . . . . . . . . . . . . . . . . . . . .❏ d) Cor pulmonale . . . . . . . . . . . . . . . . . . . . .❏ 5. Dorothy, 58, has emphysema secondary to alpha-1 antitrypsin deficiency. She has never smoked and has been compliant with adequate doses of inhaled medications. After hospital admission for an acute exacerbation of COPD, oxygen therapy has been prescribed, as well as oral steroids for one week. Regarding long-term oxygen therapy, which ONE statement is true? a) Long-term oxygen therapy involves use of oxygen for 12 hours/day . . . . . . . . . . . . . . . .❏ b) Dorothy’s SpO2 or PaO2 should be reassessed after four weeks . . . . . . . . . . . . .❏ c) Long-term oxygen therapy is indicated in obstructive sleep apnoea . . . . . . . . . . . . . . .❏ d) There is evidence that long-term oxygen therapy is beneficial in other conditions such as interstitial lung disease and cystic fibrosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . .❏ 6. Dorothy requests information about various options in long-term oxygen therapy. Which ONE statement about oxygen therapy is not true? a) Oxygen concentrators are the most efficient delivery system . . . . . . . . . . . . . . . . . . . . . . .❏ b) Oxygen should always be delivered by mask . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .❏ c) Oxygen-conserving devices are useful with oxygen cylinders . . . . . . . . . . . . . . . . . . . . . .❏ d) Annual review is recommended . . . . . . . .❏ 7. Dorothy begins oxygen therapy. The following week she complains of early morning headaches as well as some blurred vision. Arterial blood gases confirm hypercapnia. Which ONE of the following is least likely to have contributed to this? a) Alcohol consumption . . . . . . . . . . . . . . . .❏ b) Use of excessive long-term oxygen therapy flow rates . . . . . . . . . . . . . . . . . . . . . . . . . . .❏ c) Nocturnal sedation . . . . . . . . . . . . . . . . . .❏ d) Use of regular paracetamol . . . . . . . . . . . .❏ 8. Under which ONE of the following circumstances is oxygen therapy least likely to be beneficial? a) In the patient who becomes hypoxic (SpO2 <90%) with exercise . . . . . . . . . . . . . .❏ b) Dyspnoea due to congestive cardiac failure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .❏ c) Dyspnoea secondary to radiotherapyinduced fibrosis . . . . . . . . . . . . . . . . . . . . . . .❏ d) Significant nocturnal hypoxia . . . . . . . . . .❏ 9. John, 52 and healthy, is attempting to climb Mt Kilimanjaro. He has developed some confusion and mild dyspnoea. Which TWO options are indicated to relieve his symptoms? a) Increase inspired oxygen concentration to 21% by use of an oxygen cylinder . . . . . . . .❏ b) Descend . . . . . . . . . . . . . . . . . . . . . . . . . .❏ c) Use bronchodilators . . . . . . . . . . . . . . . . .❏ d) Provide moderate to high concentrations of oxygen therapy (5-15L/min) . . . . . . . . . . . . .❏ 10. Low levels of oxygen therapy (1-2L/min) easily correct the hypoxaemia related to conditions causing V/Q mismatch. In which ONE condition does V/Q mismatch not occur? a) Pulmonary embolus . . . . . . . . . . . . . . . . .❏ b) Idiopathic pulmonary fibrosis . . . . . . . . . .❏ c) COPD . . . . . . . . . . . . . . . . . . . . . . . . . . . .❏ d) Bronchiectasis . . . . . . . . . . . . . . . . . . . . .❏ NEXT WEEK Editor: Dr Lynn Buglar The next How to Treat investigates the safety and risks associated with the administration of blood and blood products in Australia. The authors are Dr Joanne Co-ordinator: Julian McAllan Pink, National Transfusion Medicine Service manager, Australian Red Cross Blood Service; and Dr Denis Spelman, head of the microbiology department and deputy director of the infectious diseases unit, Alfred Hospital, Melbourne, Victoria. 36 | Australian Doctor | 20 August 2004 www.australiandoctor.com.au