Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
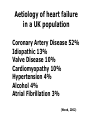
Epidemiology of heart failure Darrel Francis Clinical Senior Lecturer in Cardiology Imperial College School of Medicine • Difficulties of case definition • Aetiology • Prevalence and Incidence • Temporal trends • Global burden Case definition The greatest challenge in the epidemiology of heart failure: difficulty defining cases • Symptoms are protean • Signs are commonly found in subjects without heart failure – Tachycardia, crepitations, leg oedema(!) • Tests: what is normal? why is this a challenge? Why are normal ranges so important here? After all, we can study blood pressure without predeciding normal range… BP is easier because there is only one way to measure it (or at least experts have developed conventions) There is more than one “test” for heart failure! • No tests, just symptoms + signs Criterion Category I: history Rest dyspnea Orthopnea Paroxysmal nocturnal dyspnea Dyspnea while walking on level area Dyspnea while climbing Point value[*] 4 4 3 2 1 Category II: physical examination Heart rate abnormality (1 point if 91 to 110 beats per 1 or 2 minute; 2 points if more than 110 beats per minute) Jugular venous elevation (2 points if greater than 2 or 3 6 cm H2O; 3 points if greater than 6 cm H2O plus hepatomegaly or edema) Lung crackles (1 point if basilar; 2 points if more than 1 or 2 basilar) Wheezing 3 Third heart sound 3 Category III: chest radiography Alveolar pulmonary edema Interstitial pulmonary edema Bilateral pleural effusion Cardiothoracic ratio greater than 0.50 Upper zone flow redistribution 8 to 12 points = definite HF 5 to 7 points = possible HF <4 points = unlikely HF 4 3 3 3 2 Boston Criteria for diagnosing Heart Failure from Marantz et al Circulation 1988;77:607-12. “No tests” gives very poor validity • Less than half of those identified by clinical judgement alone are confirmed by subsequent tests • Even more unreliable for women than for men ESC gives guidelines for definition of HF Eur Heart J 2005; 26: 1115–1140 . There is more than one “test” for heart failure! • No tests, just symptoms + signs • Brain Natriuretic Peptide (blood test) • Radionucleide ventriculography (MUGA) or contrast ventriculography • 2d Echocardiography • Magnetic Resonance Imaging • Tissue Doppler Imaging Impact of difficult case definition? • Difficult to safely compare absolute rates beyond study – may be due to ascertainment method, not a true difference in the population • Reasonably safe to look for relationships (e.g. with age) within any one study Aetiology Aetiology of heart failure in a UK population Coronary Artery Disease 52% Idiopathic 13% Valve Disease 10% Cardiomyopathy 10% Hypertension 4% Alcohol 4% Atrial Fibrillation 3% (Wood, 2002) A more honest breakdown? Cowie, Hillingdon heart failure study, Eur Heart J 1999; 20: 421–428 Aetiology does change • In the 1950’s, Hypertension was the commonest aetiology – Garrison GE, McDonough JR, Hames CG, Stulb SC. Prevalence of chronic congestive heart failure in the population of Evans County, Georgia. Am J Epidemiol 1966;83:338-344. • Since then, primary prevention (antihypertensive therapy) has dramatically reduced this proportion – Kannel WB, Ho K, Thorn T. Changing epidemiological features of cardiac failure. Br Heart J 1994;72:S3-S9 Prevalence Case study: Heart of England Screening study Invited random sample (n=1617) of all men and women aged over 45 years registered at GP practices in the West Midlands. All patients who agreed to participate were assessed in their own general practice by clinical history (including prescribed drugs), determination of New York Heart Association functional class, clinical examination, resting 12 lead electrocardiography, and echocardiography including Doppler studies. Defined heart failure according to ESC criteria: appropriate symptoms (NYHA II or worse) plus objective evidence of cardiac dysfunction. EF<40%: "definitely impaired“ 40-50%: "borderline" (40-50%) Did not attempt to diagnose diastolic dysfunction. Davis et al, BMJ 2002;325:1156-60. Heart of England Screening study Over 2% of patients (3% of men and 1.7% of women) screened had definite heart failure. Probable heart failure was seen in around a further 1% of patients. From these prevalence rates they estimate: about 369,000 men aged >45 in the UK with definite heart failure, and 300,000 women, giving a total of around 669,000. If probable cases of heart failure are included, there are an estimated 497,500 men and 404,000 women, a total of 901,500 people aged 45 and over who have heart failure in the UK today. Prevalence of heart failure increases steeply with age, so that while around 1% of men and women aged under 65 have heart failure, this increases to about 7% of those aged 75-84 years and 15% of those aged 85 and above. Potentially complex contributory factors Does the “2%” prevalence cover all types of patient? Percent of Population Prevalence of Congestive Heart Failure by Age and Sex NHANES: 1999-2002 9.8 10.9 10 8 6 4.1 4 1.8 2 6.2 5.8 0.3 0.3 0.5 2.3 1.5 0.4 0 20-34 35-44 45-54 55-64 Ages Men Source: CDC/NCHS and NHLBI. Women 65-74 75+ Prevalence of heart failure, adults aged between 45 and 84, UK studies compared Source Study Year RCGP 4th National Study of Morbidity Statistics from General Practice 1991/92 Engl & Wales McDonagh et al, 1997 MONICA 1992 Mair et al, 1996 Two general practices in Liverpool 1994 Office for National Statistics,Key 2000 Health Statistics from General Practice 1998 Davies et al, 2001 Notes: Heart of England Screening Study Place MEN WOMEN 45-54 55-64 65-74 75-84 % % % % 45-54 55-64 65-74 75-84 % % % % 0.5* 3.2 Glasgow 2.5 3.2 Liverpool 2.7 5.3 10.4 ** 0.3 1.4 4.5 10.9 0.3 2.7 4.2 7.3 Engl & Wales 1995/99 W Midlands 8.0 0.4* 2.3 7.1 2.0 3.6 1.2 5.1 13.3 ** 0.2 0.9 3.6 9.9 0 0.9 1.7 6.6 * for those aged 45-64 years ** for those aged 75 & over Sources: Royal College of General Practitioners, the Office of Population Censuses and Surveys and the Department of Health (1995) Morbidity Statistics from General Practice, Fourth National Study 1991-1992. HMSO: London; Mair FS, Crowley T and Bundred P (1996) Prevalence, aetiology and management of heart failure in general practice. British Journal of General Practic McDonagh TA, Morrison CE, Lawrence A, Ford I, Tunstall-Pedoe H, McMurray JJV (1997) Syptomatic and asymptomatic left ventricular systolic dysfun Office for National Statistics (2000) Key Health Statistics from General Practice. The Stationery Office: London. Davies MK, Hobbs FDR, Davis RC, Kenkre JE, Roalfe AK, Hare R, Wosornu D, Lancashire RJ (2001) Prevalence of left-ventricular systolic dysfunction and heart failure in the Echocardiographic Heart of England Screening study: a population based study. The Lancet 358:439-444. Prevalence of heart failure by deprivation, 1998, England and Wales 250 Prevalence per 1,000 population Most deprived (Q5) Least deprived (Q1) 200 150 100 50 0 45-54 55-64 65-74 75-84 85 and over Total Age group Ellis C et al (2001) Health Statistics Quarterly 11: 17-24 www.heartstats.org Prevalence of treated heart failure by age, sex and deprivation category, 1998, England and Wales 45-54 55-64 65-74 75-84 85 & over Total 1.7 2.8 2.7 2.6 3.5 10.0 12.7 13.1 14.4 18.3 39.7 43.2 41.8 48.0 50.6 102.7 120.5 101.6 109.6 107.5 213.2 193.2 184.8 195.4 169.5 25.9 28.8 26.8 29.3 30.5 1.4 1.3 1.5 2.0 2.6 5.4 7.8 8.5 9.6 14.0 27.0 35.4 32.5 37.7 43.9 83.0 99.7 101.6 106.8 93.6 195.7 199.2 183.0 184.9 186.1 19.8 23.6 23.0 25.1 26.8 Men Q1 (least deprived) Q2 Q3 Q4 Q5 (most deprived) Women Q1 (least deprived) Q2 Q3 Q4 Q5 (most deprived) Notes: Data from the General Practice Research Database. Deprivation categories were derived using the Townsend Material Deprivation Score at ward level. The category Q1 contains the 20% least deprived wards in England and Wales and category Q5 contains the 20% most deprived wards. Source: Ellis C, Gnani S and Majeed A (2001) Prevalence and management of heart failure in General Practice in England and Wales, 1994-1998. Health Statistics Quarterly 11: 17-24. Temporal trends Prevalence is rising… Discharges in Thousands Congestive Heart Failure Episodes by Sex United States: 1970-2002 600 500 400 300 200 100 0 70 72 74 76 78 80 82 84 86 88 90 92 94 96 98 00 02 Years Source: CDC/NCHS. Males Females Why is prevalence rising? Levy, NEJM 2002; 347:1397-1402 Survival Levy, NEJM 2002; 347:1397-1402 Levy, NEJM 2002; 347:1397-1402 Levy, NEJM 2002; 347:1397-1402 Levy, NEJM 2002; 347:1397-1402 Survival after diagnosis of cancer or heart disease 100 Men: 80 Survival % 60 MI Bladder Ca 40 Prostate Ca Bowel Ca Heart Failure 20 Lung Ca 0 0 12 24 36 48 60 Months from diagnosis Stewart S, EJHF 2001; 3:315-322 Survival after diagnosis of cancer or heart disease in women: Where does breast cancer lie? 100 80 Survival % Breast cancer Ca 60 MI 40 Ovarian Ca Bowel Ca Heart Failure 20 Lung Ca 0 0 12 24 36 48 60 Months from diagnosis Epidemiology of Heart failure •Numbers heavily depend on methods – clinical assessment is unreliable •Marked increase in prevalence with age •Risk factors are similar to those of coronary artery disease •Mortality worse than most cancers •Increasing survival with modern therapy leads to increasing prevalence Today a problem of the developed world, but…