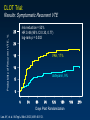
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Oncology Grand Rounds University of North Carolina Lineberger Comprehensive Cancer Center April 21, 2009 An Oncologists Perspective on Cancer and Thrombosis Gary H. Lyman, MD, MPH, FRCP(Edin) Professor of Medicine and Director Health Services, Effectiveness and Outcomes Research Duke University School of Medicine and the Duke Comprehensive Cancer Center Cancer and Venous Thromboembolism (VTE) Armand Trousseau • Association recognized since Trousseau’s observation more than 130 years ago1 • Of all cases of VTE, approximately 20% occur in cancer patients.2 • VTE affects 4-20% of cancer patients antemortem but has been reported in up to 50% on postmortem examination.3-4 • Cancer-associated VTE has important clinical and economic consequences5-7 Patients with cancer: 20% All deep venous thrombosis and pulmonary embolism 1. Trousseau, Armand. In Clinique Medicale de l'Hôtel-Dieu de Paris, 2nd ed. Paris: J.B. Bailliere et Fils; 1865 2. Lee AY. Br J. Haematol. 2005;128:291-302. 3. Gao S et al: Expert Rev Anticncer Ther 2004; 4: 303-320. 4. Lyman GH et al: J Clin Oncol 2007; 25: 5490-5505. 5. Sorensen HT, et al. N Engl J Med. 2000;343:1846-1850. 6. Prandoni P, et al. Blood. 2002;100:3484-3488. 7. Khorana AA, et al. J Clin Oncol. 2006;24:484-490. Pathogenesis: Virchow’s Triad Stasis Blood Components [Hypercoagulability] Vessel Damage Bed rest and immobility, extrinsic compression of vessel by mass Tumors and macrophages produce procoagulants, inflammatory cytokines Direct tumor invasion, indwelling catheters, chemotherapy, erythropoietin, antiangiogenic agents Growth Invasion Metastases Angiogenesis Hemostatic System Tumor Cells Procoagulant Activity Cytokines Growth Factors Fibrinolytic Activity Kuderer NM et al J Clin Oncol 2009 (in press) Risk of VTE Varies Over Natural History of Cancer 8 Risk (Odds Ratio) 7 Hospitalization Chemotherapy 6 5 End of life Metastasis Diagnosis 4 Risk of VTE in the cancer population 3 2 1 Remission Risk of VTE in the general population 0 Time Rao MV, et al. In: Khorana and Francis, eds. Cancer-Associated Thrombosis; 2007. VTE within Two years of Cancer Diagnosis Metastatic Disease Local-Regional Disease • The California Cancer Registry linked to the California Discharge Data, 1993 - 1995. • Among 235,149 cancer cases, 3775 (1.6%) were diagnosed with VTE within 2 years including 463 (12%) at the time cancer and 3312 (88%) subsequently. Chew, H. K. et al. Arch Intern Med 2006;166:458-464. Incidence of VTE in US Patients With and Without Cancer, 1979-1999 National Hospital Discharge Survey VTE Incidence (%) 4 Cancer 3 No cancer 2 1 0 1979 1981 1983 1985 1987 1989 Years Stein PD, et al. Am J Med. 2006;119:60-68. 1991 1993 1995 1997 1999 Risk Factors for VTE in Patients with Cancer Patient-related factors • Older age • Gender • Race (higher in African Americans, lower in Asians) • Patient comorbidities • History of VTE Cancer-related factors • Site of cancer • Advanced stage • Initial period after diagnosis Treatment-related factors • • • • • • Major surgery Hospitalization Chemotherapy Hormonal therapy Antiangiogenic agents ESAs, ?Transfusions Biomarkers • • • • Platelet and leukocyte counts Tissue factor P-selectin D-dimer Rao MV, et al. In: Khorana and Francis, eds. Cancer-Associated Thrombosis; 2007. Risk Factors for VTE in Patients with Cancer Patient-related factors • Older age • Gender • Race (higher in African Americans, lower in Asians) • Patient comorbidities • History of VTE Cancer-related factors • Site of cancer • Advanced stage • Initial period after diagnosis Treatment-related factors • • • • • • Major surgery Hospitalization Chemotherapy Hormonal therapy Antiangiogenic agents ESAs, ?Transfusions Biomarkers • • • • Platelet and leukocyte counts Tissue factor P-selectin D-dimer Important Consequences of VTE in Cancer Patients • Increased morbidity – Hospitalization – Anticoagulation – Postphlebitic syndrome • Increased mortality • Increased risk of recurrent VTE • Bleeding complications • Cancer treatment delays • Increased healthcare costs Important Consequences of VTE in Cancer Patients • Increased morbidity – Hospitalization – Anticoagulation – Postphlebitic syndrome • Increased mortality • Increased risk of recurrent VTE • Bleeding complications • Cancer treatment delays • Increased healthcare costs Effect of VTE on Risk of Death Stratified by Stage, Adjusted for Age and Race • CA Cancer Registry linked to Discharge Data • Overall Mortality – HR=3.7 [1.3-14.4] • Multivariate analysis – Stratified by stage – Adjusted for age, race – VTE is a significant predictor for 1 year mortality for each cancer type Chew, H. K. et al. Arch Intern Med 2006;166:458-464. VTE in Diffuse Large B-cell Lymphoma Retrospective review of patients with DLBCL treated 1990-2001 Symptomatic VTE at diagnosis or during initial treatment. – 27/211 patients (12.8%). Median survival (years) – Controls: 5.20 [1.80 – 8.60] – VTE: 1.04 [0.75 – 1.33] – P = 0.038 Multivariate Analysis for Mortality* Variable HR P-value Age 1.02 .014 IPI 1.45 .015 VTE 1.92 .025 * Adjusted for sex, race, and stage Komorokji RS et al. Leuk Lymph 2006; 47: 1029-1033 Unsuspected PE On Routine Cancer Staging Impact on Survival Retrospective review of 70 patients with unsuspected PE found on staging CT – 2003–2006 – VTE, anticoagulation or multiple cancers excluded 2:1 matching based on – Cancer type – Age – Stage Unsuspected PE: – Subsegmental: 24.3% – Proximal: 75.7% O’Connell CL et al: ASH 2008 HR=1.79 [95% CI: 1.10-2.90; P=0.018] Unsuspected VTE in Cancer Patients Results from Autopsy Series Roswell Park Cancer Institute Consecutive autopsies in 506 cancer patients Causes of Death, n (%) – Major – – – – Infection 184 (36%) Hemorrhage 55 (11%) VTE 35 (7%) MI 35 (7%) – Contributing – – – – Infection 68 (13%) Hemorrhage (25%) VTE 91 (18%) MI 13 (3%) Ambrus J et al J Med 1975; 6: 61-64 University of Missouri 578 consecutive autopsies 145 cancer patients, n (%) – PE 24 (17%) – Fatal PE 20 (14%) 433 noncancer patients – PE 55 (13%) – Fatal PE 343 (8%) P<.05 Author’s conclusions: – 1 in 7 hospitalized cancer pts died of PE – 60% of fatal PEs occur in early or limited metastatic disease Shen VS et al. South Med J 1980; 73: 841-843 Causes of Early Death in Ambulatory Cancer Patients Results from Prospective Study of Series Patient Population – Prospective study of 4466 patients starting new chemotherapy – Consecutive patients accrued at 117 US practices – Median followup of 75 days, 141 (3.2%) died. Causes of Death, n (%) – All 141 (100) – Progression of cancer 100 (70.9) – Thromboembolism 13 (9.2) – – – – – – – Breast Cancer 40% Colon Cancer 14% Small Cell Lung 5% Arterial 8 (5.6) Venous 5 (3.5) Infection 15 (10.6) Respiratory failure 5 (3.5) Bleeding 2 (1.4) Other 9 (6.4) Unknown 5 (3.5) Non-small Cell Lung 18% Ovarian 8% Non-Hodgkin's Lymphoma 13% Hodgkin's Lymphoma 2% Distribution of Cancer Type Khorana AA et al. J Thromb Haemost 2007; 5: 632-634 Recommendations for Venous Thromboembolism Prophylaxis and Treatment in Patients with Cancer ASCO Clinical Practice Guideline Lyman GH et al: J Clin Oncol 2007; 25:5490-5505 Clinical Questions 1. Should patients with cancer receive anticoagulation for VTE prophylaxis while hospitalized? √ 2. Should ambulatory patients with cancer receive anticoagulation for VTE prophylaxis during systemic chemotherapy? √ 3. Should patients with cancer undergoing surgery receive perioperative VTE prophylaxis? 4. What is the best method for treatment of patients with cancer with established VTE to prevent recurrence? √ 5. Should patients with cancer receive anticoagulants in the absence of established VTE to improve survival? √ Lyman GH et al: J Clin Oncol 2007; 25:5490-5505 ASCO Recommendations for VTE Prophylaxis in Patients with Cancer Hospitalized Cancer Patients • Hospitalized patients with cancer should be considered candidates for VTE prophylaxis in the absence of bleeding or other contraindications to anticoagulation. Lyman GH et al: J Clin Oncol 2007; 25:5490-5505 Risk of Inpatient VTE By Site of Cancer – Solid Tumor Discharge database of the University HealthSystem Consortium • 115 U.S. academic medical centers • 66,106 adult neutropenic cancer patients hospitalized 1995 - 2002 Rate (%) 12 10 8 6 4 2 0 Khorana et al, J Clin Oncol 2006; 24: 484-490 Risk of Inpatient VTE by Type of Cancer – Hematologic Malignancies Percent (%) 7 6 5 4 3 2 1 0 All Leukemia NHL Hodgkin Account for one-third of all VTE NHL=Non-Hodgkin’s lymphoma Khorana AA, et al. J Clin Oncol. 2006;24:484-490. Myeloma Discharge database of the University HealthSystem Consortium • 133 U.S. academic medical centers • 1,015,598 adult cancer patients hospitalized 1995 - 2003 7.0 6.5 6.0 5.5 5.0 4.5 4.0 3.5 3.0 2.5 2.0 1.5 1.0 0.5 0.0 VTE: 34,357 (3.4%) PE: 11,515 (1.1%) 20 P<0.0001 Inpatient Mortality (%) Rate of VTE (%) VTE Inpatient Risk and Mortality 1995 1996 1997 1998 1999 2000 2001 2002 2003 VTE- patients on chemo VTE-all patients DVT-all patients PE-all patients Khorana AA et al. Cancer 2007; 110: 2339-2346 18 16 14 12 10 8 6 4 2 0 P<0.0001 1995 1996 1997 1998 1999 2000 2001 2002 2003 VTE No VTE Anticoagulant Prophylaxis to Prevent Screen-Detected VTE High Risk Hospitalized Medical Patients • 3 large, randomized, placebo-controlled, double-blind trials in medical patients at high risk including cancer – MEDENOX (enoxaparin)1 ~ 15% – PREVENT (dalteparin)2 ~5% – ARTEMIS (fondaparinux)3 ~15% • Screening for asymptomatic DVT with venography or ultrasound 1. Samama MM, et al. N Engl J Med. 1999;341:793-800. 2. Leizorovicz A, et al. Circulation. 2004;110:874-879. 3. Cohen AT, et al. BMJ. 2006;332:325-329. Anticoagulant Prophylaxis to Prevent Screen-Detected VTE High Risk Hospitalized Medical Patients: VTE Study RRRRRR MEDENOX1 P < 0.001 63% PREVENT2 P = 0.0015 45% Placebo 47% Enoxaparin 40 mg 5.5 Placebo 5.0 Dalteparin 5,000 units Fondaparinux 2.5 mg MM, et al. N Engl J Med. 1999;341:793-800. Leizorovicz A, et al. Circulation. 2004;110:874-9. 3Cohen AT, et al. BMJ 2006; 332: 325-329. 2 14.9 2.8 10.5 Placebo ARTEMIS3 1Samama Thromboprophylaxis Patients with VTE (%) 5.6 Incidence of Major Bleeding (%) Anticoagulant Prophylaxis to Prevent Screen-Detected VTE High Risk Hospitalized Medical Patients: Major Bleeding 1.8 1.7% 1.6 1.4 1.2 1.1% 1.0 LMWH 0.8 Placebo 0.49% 0.6 0.4 0.16% 0.2% 0.2 0.0 Medenox Prevent Study Samama MM, et al. N Engl J Med. 1999;341:793-800. Leizorovicz A, et al. Circulation. 2004;110:874-9. Cohen AT, et al. BMJ 2006; 332: 325-329.. Artemis ASCO Recommendations for VTE Prophylaxis in Patients with Cancer Ambulatory Cancer Patients 1. Routine prophylaxis with an antithrombotic agent is not recommended. 2. Patients receiving thalidomide or lenalidomide with chemotherapy or dexamethasone are at high risk for thrombosis and warrant prophylaxis. LMWH or adjusted dose warfarin (INR~1.5) is recommended. • This recommendation is based on extrapolation from studies of post-operative prophylaxis in orthopedic surgery and a trial of adjusted dose warfarin in patients with breast cancer. 3. Randomized clinical trials evaluating antithrombotic agents in pts with myeloma on thalidomide or lenalidomide are needed. 4. Research is also urgently needed to identify better markers in ambulatory patients with cancer likely to develop VTE. Lyman GH et al: J Clin Oncol 2007; 25:5490-5505 Prospective Study of Adult Cancer Patients Receiving Systemic Chemotherapy • Prospective observational study conducted at 117 randomly selected US practice sites. Proportion with VTE • Data obtained on 4,458 consecutive adult patients initiating a new chemotherapy regimen between March 2003 and February 2006. • There were no exclusions for age, prior history or comorbidities with nearly 40% of patients age 65 and older. .04 .03 .02 .01 0.00 Kuderer NM et al; J Clin Oncol 2008 (ASCO 2008). 0 10 20 30 40 50 60 70 80 90 Time (Days) 100 110 120 130 140 150 Reported Cause of Early Mortality Cancer Patients Starting New Chemotherapy 1.00 [HR=5.48, 95%CI: 2.21-13.61; P<.0001] Cause of Death No VTE N=4,365 VTE N=93 All N=4,458 PD 2.1 2.2 2.1 Infection 0.3 0 0.3 0 5.4 0.1 Pulmonary 0.2 0 0.2 Bleeding 0.1 0 0.1 Other vascular 0.2 0 0.2 Unknown 0.3 0 0.3 All 3.2 7.6 3.3 .99 .98 .97 .96 PE .95 .94 No VTE .93 .92 .91 VTE .90 0 10 20 30 40 50 60 70 80 90 100 110 120 130 140 150 Time (Days) Kuderer NM et al; J Clin Oncol 2008 (ASCO 2008) RCTs of Thromboprophylaxis in Ambulatory Cancer Patients Warfarin • Double-blind, placebo-controlled RCT demonstrated the efficacy of low-intensity warfarin (INR 1.3-1.9) in patients receiving chemotherapy for metastatic breast cancer • 311 women with metastatic breast cancer on 1st- or 2nd-line chemotherapy • Randomized to 1 mg warfarin for 6 weeks, then warfarin titrated to INR 1.3-1.9 or placebo • 1 VTE in warfarin group vs 7 in placebo arm – 85% risk reduction, P = .03, with no increased bleeding INR=international normalized ratio Levine M, et al. Lancet. 1994;343:886-889. RCTs of Thromboprophylaxis in Ambulatory Cancer Patients Low Molecular Weight Heparin Trial N Treatment Chemo Duration VTE Major Bleeding FAMOUS 385 Dalteparin Placebo 64% 12 months 2.4% 3.3% 0.5% 0 TOPIC-I 353 Certoparin Placebo 100% 6 months 4% 4% 1.7% 0 TOPIC-2 547 Certoparin Placebo 100% 6 months 4.5%† 8.3% 3.7% 2.2% PRODIGE 186 Dalteparin Placebo - 6-12 months 11% 17% 5.1% 1.2% SIDERAS 141 Dalteparin Placebo/Control 54% Indefinitely 5.9% 7.1% 2.9% 7.1% PROTECHT 1166 Nadroparin 2:1 Placebo 100% < 4 months with chemo 1.4% 2.9% 0.7% 0 Solid tumors (Stage III/IV) Breast (Stage IV) NSCLC (Stage IV) Glioma Solid Tumors (Stage IV) Solid Tumors (Stage III/IV) 1. Kakkar AK, et al. J Clin Oncol. 2004;22:1944-1948. 2. Haas SK, et al. J Thromb Haemost. 2005(suppl 1): abstract OR059. 3. Perry JR et al. Proc ASCO 2007. 2011 4. Sideras K et al. Mayo Clin Proc 2006; 81:758-767. 5. Agnelli G et al. Am Soc Hemat Sunday December 7, 2008 The PROTECHT Study RCT of Thromboprophylaxis in Cancer Patients Receiving Chemotherapy DESIGN Placebo-controlled, double blind, multicenter RCT Nadroparin 3,800 anti Xa IU daily vs placebo: 2:1 1150 patients receiving chemotherapy for locally advanced or metastatic cancer. Start with new CTX; continue for maximum of 4 m Mean treatment duration: 90 days Primary outcome: clinically detected thrombotic events, i.e., composite of venous and arterial TE* Main safety outcome: Major bleeding * deep vein thrombosis of the lower and upper limbs, visceral and cerebral venous thrombosis, pulmonary embolism, acute myocardial infarction, ischemic stroke, acute peripheral arterial thromboembolism, unexplained death of possible thromboembolic origin Agnelli G et al: ASH 2009 The PROTECHT Study RCT of Thromboprophylaxis in Cancer Patients Receiving Chemotherapy RESULTS • Primary Efficacy Outcome: Any TE Event* – – – – Nadroparin: 16 of 769 (2.1%) Placebo: 15 of 381 (3.9%) Relative risk reduction: 47.2%, (interim-adjusted p=0.033) Absolute risk decrease: 1.8%; NNT = 53.8 • Venous thromboembolism (VTE): – – Nadroparin: 11 of 769 (1.4%) Placebo: 11 of 381 (2.9%) NS • Major Bleeding: – – – Nadroparin: 5 (0.7%) Placebo: 0 (p= 0.177) Absolute risk increase: 0.7%; NNH = 153.8 Agnelli G et al: ASH 2009 ASCO Recommendations for VTE Prophylaxis in Patients with Cancer Relative contraindications for anticoagulation • • • • • • • • • Active, uncontrollable bleeding Active cerebrovascular hemorrhage Dissecting or cerebral aneurysm Bacterial endocarditis Pericarditis, active peptic or other GI ulceration Severe, uncontrolled or malignant hypertension Severe head trauma Pregnancy (warfarin) Heparin-induced thrombocytopenia (heparin, LMWH) • Epidural catheter placement Lyman GH et al: J Clin Oncol 2007; 25:5490-5505 Risk of VTE in Cancer Patients Receiving Thalidomide Meta-analysis of RCTs [Estimates ± 95% CI] • Search identified 17 RCTs including 3,977 patients • Incidence of VTE – All Studies: 11.7% [8.1% - 16.5%] • Multiple Myeloma: 17.7% [10.9% - 22.1%] • Solid Tumors: 5.3% [2.1% - 12.8%] • Relative Risk for VTE – All Studies: 2.4 [1.9 – 3.0], P<.001 • Multiple Myeloma: 3.1 [2.1 – 4.4], P<.001 • Solid Tumors: 3.5 [1.1 – 10.6], P=.028 – Prophylaxis (all studies) • No prophylaxis: 3.5 [2.5 – 4.9], P<.001 • Prophylaxis: 1.9 [1.4 – 2.5], P<.001 Gray KN et al: ASH 2008 Thromboembolism With Bevacizumab Arterial Thromboembolism Pooled analysis of 5 clinical trials of bevacizumab in metastatic colorectal, breast, or non-small cell lung cancer (N=1,745) Chemotherapy* plus bevacizumab (n=963) Chemotherapy* alone (n=782) 12 ATE/VTE Rate (%) 10 8 6 HR=2.0 (95% CI, 1.05-3.75) P=.031 4 2 0 Arterial thromboembolism (ATE) VTE Thromboembolism With Bevacizumab Venous Thromboembolism: Meta-Analysis of RCTs Relative Risk = 1.33 [95% CI: 1.13 – 1.56] Absolute Risk Increase: 2.2% [95% CI: 1.1% - 3.3%] Nalluri, S. R. et al. JAMA 2008;300:2277-2285. Thromboembolic Complications in Cancer Patients Receiving ESAs Hb Stopping Value ESA Cont RR 95% CI < 12 g/dL 50 50 (0) >12 - <13 g/dL 148 141 0.70 0.29, 1.67 >13 - <14 g/dL 1,596 1,290 1.71 1.23, 2.40 >14 - <15 g/dL 1,151 914 1.92 1.22, 3.02 >15 - <16 g/dL 368 303 1.66 1.08, 2.54 (Unclear) 42 39 5.59 0.71, 43.94 Comparative Effectiveness Review # 3 Comparative Effectiveness of Epoetin and Darbepoetin for Managing Anemia in Patients Undergoing Cancer Treatment RR TE = 1.67 [1.35 – 2.06] Bohlius, J. et al. JNCI 2006 98:708-714 Predictors of Venous Thromboembolism Multivariate Logistic Regression Analysis Retrospective cohort study of cancer pts at 60 US hospitals: 1995 – 2003. Patients: N = 504,208 RBC trans: 70,542 (14%) Platelet trans: 15,237 (3%) RBC transfusions VTE: 7.2% ATE: 5.2% Mortality 1.34 [95% CI:1.29-1.38] Khorana, A. A. et al. Arch Intern Med 2008;168:2377-2381. ASCO Recommendations for VTE Prophylaxis in Patients with Cancer Preventing Recurrence in Cancer Patients with Established VTE 1. LMWH is the preferred approach for the initial 5 to 10 days of anticoagulant treatment of the patient with cancer with established VTE. 2. LMWH given for at least 6 months is also the preferred approach for long-term anticoagulant therapy. Vitamin K antagonists with a targeted INR of 2-3 are acceptable for long-term therapy when LMWH is not available. 3. After 6 months, indefinite anticoagulant therapy should be considered for patients with active cancer. 4. The insertion of a vena cava filter is only indicated for patients with contraindications to anticoagulant therapy and in those with recurrent VTE despite adequate longterm therapy with LMWH. Lyman GH et al: J Clin Oncol 2007; 25:5490-5505 Recurrent VTE and bleeding during anticoagulant treatment Patients with cancer and venous thrombosis 30 30 Cancer 21% 20 10 No Cancer 7% Hazard ratio 2.2 [1.2-4.1] Major Bleeding, % Recurrent VTE, % Hazard ratio 3.2 [1.9-5.4] 20 Cancer 12% 10 No Cancer 5% 0 0 0 1 2 3 4 5 6 7 8 9 101112 Time (months) Prandoni P et al. Blood 2002; 100: 3484-3488. 0 1 2 3 4 5 6 7 8 9 10 11 12 Time (months) RCTs of Long-term Treatment in Cancer Patients with VTE: RCTs of LMWH vs. Vitamin K Antagonists in Cancer Recurrent VTE, % Major Bleed, % Death, % Study No. Long-Term Treatment Meyer1 2002 71 Warfarin 21.1* 22.7 67 Enoxaparin 1.5 mg/kg 10.5* 11.3 Lee2 2003 336 Warfarin 17* 4 41 336 Dalteparin 200/150 IU/kg 9* 6 39 30 Warfarin 10 2.9 8.8 29 Enoxaparin 1.0 mg/kg 6.9 6.5 6.5 32 Enoxaparin 1.5 mg/kg 6.3 11.1 19.4 100 Warfarin 10* 7 19 100 Tinzaparin 175 IU/kg 6* 7 20 Deitcher3 2006 Hull4 2006 * P < .05 1. Meyer G, et al. Arch Intern Med. 2002;162:1729-1735. 2. Lee AY, et al. N Engl J Med. 2003;349:146-153. 3. Deitcher SR, et al. Clin Appl Thromb Hemost. 2006;12:389-396. 4. Hull RD, et al. Am J Med. 2006;119:1062-1072. The CLOT Trial Study Schema Control Group Dalteparin 200 IU/kg OD Vitamin K antagonist (INR 2.0 to 3.0) x 6 mo Experimental Group Dalteparin 200 IU/kg OD x 1 mo 5 to 7 days then ~150 IU/kg OD x 5 mo 1 month Lee AY, et al. N Engl J Med. 2003;349:146-153. 6 months CLOT Trial: Results: Symptomatic Recurrent VTE risk reduction = 52% HR 0.48 (95% CI 0.30, 0.77) log-rank p = 0.002 Probability of Recurrent VTE, % 25 20 VKA, 17% 15 10 dalteparin, 9% 5 0 0 30 60 90 120 150 Days Post Randomization Lee AY, et al. N Engl J Med. 2003;349:146-153. 180 210 CLOT Trial: Results: Bleeding Dalteparin VKA N=338 N=335 19 (5.6%) 12 (3.6%) associated with death 1 0 critical site* 4 3 14 9 Major bleed pvalue 0.27 transfusion of > 2 units of RBC or drop in Hb > 20 g/L Any bleed 46 (13.6%) 62 (18.5%) *intracranial, intraspinal, pericardial, retroperitoneal, intra-ocular, intraarticular Lee AY, et al. N Engl J Med. 2003;349:146-153. 0.09 ASCO Recommendations for VTE Prophylaxis in Patients with Cancer Improving survival in absence of established VTE 1. Anticoagulants are not recommended to improve survival in patients with cancer without VTE. 2. People with cancer should be encouraged to participate in clinical trials designed to evaluate anticoagulant therapy as an adjunct to standard anticancer therapies. Lyman GH et al: J Clin Oncol 2007; 25:5490-5505 Systematic Review of Anticoagulants as Cancer Treatment: Impact on Survival 1-Year Overall Mortality by Type of Anticoagulation Treatment Cancer Citation SCLC Altinbas Mixed Rate 1 Rate 2 0.5 2 1 RR [95% CI] .696 .476 1.018 .054 P Value .487 .700 Kakkar .542 .592 .915 .766 1.093 .327 Mixed Klerk .608 .727 .836 .711 .983 .028 Mixed Sideras .603 .600 1.005 .766 1.319 .972 .88 .79 .015 .862 .724 1.026 .093 .86 .72 1.03 .095 LMWH SCLC Lebeau .601 .698 UFH .98 SCLC Chahinian .728 .802 .908 .775 1.063 .233 Breast Levine .382 .403 .948 .719 1.251 .705 SCLC Maurer .242 .278 .869 .608 1.240 .438 NSCLC Zacharski (1) .802 .796 1.008 .875 1.161 .915 SCLC Zacharski (2) .600 .840 .714 .497 1.027 .059 CRC Zacharski (3) .588 .529 1.111 .727 1.697 .625 Prostate Zacharski (4) .357 .300 1.190 .366 3.871 .770 HN Zacharski (5) .850 .667 1.275 .895 1.817 .172 NSCLC (early) Zacharski (6) .143 .300 .476 .137 1.651 .224 Warfarin .94 .85 1.04 .239 Combined .91 .85 .003 Anticoagulation Kuderer NM, et al. Cancer. 2007;110:1149-1161 .97 Control SCLC=small cell lung cancer; NSCLC=non-small cell lung cancer; HN=head and neck; CRC=colorectal cancer Systematic Review of Anticoagulants as Cancer Treatment: Impact on Survival Major Bleeding Complications by Type of Anticoagulation Treatment Rate 1 Rate 2 0.1 0.2 0.5 1 2 5 10 Study SCLC Altinbas .000 .000 1.025 .021 50.418 .990 NSCLC Haas (2) .037 .023 1.642 .605 4.453 .325 Mixed Sideras .029 .071 .412 .083 2.051 .261 Mixed Klerk .034 .006 5.203 .615 44.006 .089 Mixed Kakkar .005 .000 2.906 .119 70.874 .492 Breast Haas (1) .017 .000 7.120 .370 136.830 .127 1.68 .86 3.27 .128 1.007 .064 15.943 .996 1.01 .06 15.94 .996 LMWH SCLC Lebeau .007 .007 UFH RR [95% CI] P Value Cancer SCLC Zacharski (2) .400 .080 5.000 1.217 20.549 .008 SCLC Maurer .067 .018 3.798 1.091 13.223 .023 SCLC Chahinian .068 .000 12.548 .727 216.606 .023 Prostate Zacharski (4) .571 .200 2.857 .763 10.695 .069 NSCLC (early) Zacharski (6) .524 .250 2.095 .885 4.960 .072 NSCLC Zacharski (1) .323 .071 4.521 2.092 9.768 .000 HN Zacharski (5) .500 .381 1.312 .652 2.642 .443 CRC Zacharski (3) .618 .206 3.000 1.473 6.109 .001 Breast Levine .007 .013 .523 .048 5.709 .588 4.16 <.001 3.49 <.001 Warfarin 2.98 Combined 2.59 1.94 Control Kuderer NM, et al. Cancer. 2007;110:1149-1161 Anticoagulation 2.13 Systematic Review of Anticoagulants as Cancer Treatment: Impact on Survival Findings • Anticoagulation significantly decreased 1-year overall mortality with a relative risk of 0.905 [95% CI, 0.847-0.967]; P=.003 Conclusions • Anticoagulants, particularly LMWH, significantly improved overall survival in cancer patients without VTE while increasing the risk for bleeding complications • Improved survival with anticoagulation may be dependent on tumor type • However: given the limitations of available data, the use of anticoagulants as antineoplastic therapy cannot be recommended until additional RCTs confirm these results Kuderer NM, et al. Cancer. 2007;110:1149-1161. Ongoing Randomized Clinical Trials Testing the Effect of LMWH on Survival in Cancer Patients Principal Investigator Study LMWH Tumor Type(s) INPACT Nadroparin Advanced prostate, non-small cell lung, pancreatic H. Buller FOCUS Dalteparin Ovarian A. Lee FRAGMATIC Dalteparin Lung S. Noble ABEL Bemiparin Small cell lung R. Lecumberri TILT Tinzaparin Non-small cell lung (I, II, III-A) G. Meyer & P. Girard GASTRANOX Enoxaparin Gastric (III/IV) A. K. Kakkar INPACT=Improving with Nadroparin the Prognosis in Advanced Cancer Treatment; FOCUS=Fragmin® in Ovarian Cancer: Utility on Survival; FRAGMATIC=Fragmin® Added to Standard Therapy in Patients with Lung Cancer; ABEL=Adjuvant Bemiparin in Small Cell Lung Carcinoma; TILT=Tinzaparin in Lung Tumors. Courtesy Dr Anna Falanga Clinical Risk Model for Chemotherapy-associated VTE Patient Characteristics Characteristic Development Cohort N (%) Validation Cohort N (%) P value 2,701 (100) 1,365 (100) ─ 60 (2.2) 28 (2.1) .72 1,083 (40.1) 2,473 (91.6) 332 (12.3) 515 (37.7) 1,242 (91) 166 (12.2) .14 .54 .9 Stage IV Platelet count ≥350,000/mm3 997 (36.9) 604 (22.4) 477 (34.9) 295 (21.6) .06 .59 ESA Recent surgery 764 (28.3) 829 (30.7) 358 (26.2) 473 (34.7) .17 .01 All All VTE Age >65 yr PS 0-1 BMI >35 PS=performance status; BMI=body mass index; ESA=erythropoiesis-stimulating agents. Khorana AA et al. Blood. 2008; 111:4902-4907 Clinical Risk Model for Chemotherapy-associated VTE Predictors of VTE: Multivariate Analysis β OR* P-value 1.46 .43 4.3 1.5 .05 Platelet count >350,000/mm3 .6 1.8 .03 Hemoglobin <10 g/dL or use of ESA .89 2.4 .001 Leukocyte count >11,000/mm3 .77 2.1 .008 BMI >35 .9 2.5 .01 Characteristic Site of cancer Very high risk (stomach, pancreas) High risk (lung, lymphoma, gynecologic, genitourinary excluding prostate) *Odds ratio adjusted for stage Khorana AA et al. Blood. 2008; 111:4902-4907 Clinical Risk Model for Chemotherapy-associated VTE Risk Score Based on Pretreatment Risk Factors Risk Factors Risk score 1. Site of cancer a) Very high risk cancer (stomach, pancreas) 2 b) High risk (lung, lymphoma, gynecologic, bladder, testicular) 1 2. Platelet count >350,000/mm3 1 3. Hemoglobin level < 10 g/dL or use of Red cell growth factors 1 4. Leukocyte count >11,000 /mm3 1 5. BMI > 35 kg/m2 1 Khorana AA et al. Blood. 2008; 111:4902-4907 Clinical Risk Model for Chemotherapy-associated VTE Risk Score Based on Pretreatment Risk Factors Risk Factors Risk score 1. Site of cancer a) Very high risk cancer (stomach, pancreas) 2 b) High risk (lung, lymphoma, gynecologic, bladder, testicular) 1 2. Platelet count >350,000/mm3 1 3. Hemoglobin level < 10 g/dL or use of Red cell growth factors 1 4. Leukocyte count >11,000 /mm3 1 5. BMI > 35 kg/m2 1 Khorana AA et al. Blood. 2008; 111:4902-4907 Clinical Risk Model for Chemotherapy-associated VTE Risk Score Based on Pretreatment Risk Factors Risk Factors Risk score 1. Site of cancer a) Very high risk cancer (stomach, pancreas) 2 b) High risk (lung, lymphoma, gynecologic, bladder, testicular) 1 2. Platelet count >350,000/mm3 1 3. Hemoglobin level < 10 g/dL or use of Red cell growth factors 1 4. Leukocyte count >11,000 /mm3 1 5. BMI > 35 kg/m2 1 Khorana AA et al. Blood. 2008; 111:4902-4907 VTE Prediction Risk Score Chemotherapy – Associated Thrombosis Rate of VTE (%) 8% 7.1% 7% Development cohort Development cohort 6% Validation Validationcohort cohort 6.7% 5% 4% 3% 1.8% 2% 1% 2.0% 0.8% 0.3% 0% n=734 n=374 RISK SCORE: Low (0) Khorana AA et al. Blood. 2008; 111:4902-4907 n=1,627 n=842 Intermediate (1-2) n=340 n=149 High (>3) Venous Thromboembolism and Overall Survival by VTE Risk Score Categories Overall Survival Venous Thromboembolism .10 1.00 Low High P<.001 .08 Overall Survival .95 P < 0.001* .06 .04 Intermediate P < 0.001* P<.001 P<.001 .90 High .85 Mortality Intermediate .80 .02 P<.001 Low Grp Low Intermed High % 1.2 5.9 12.7 HR 1.0 3.56 [1.91-6.66] 6.89 [3.50-13.57] .75 0.00 0 10 20 30 *Overall test of significance 40 50 60 70 80 90 100 110 Time (Days) Kuderer NM et al; Blood 2008 (ASH 2008) 120 0 10 20 30 *Overall test of significance 40 50 60 70 Time (Days) 80 90 100 110 120 LMWH prophylaxis NIH trial in cancer outpatients Phase III Multicenter Trial of Thromboprophylaxis in High Risk Ambulatory Cancer Patients Receiving Chemotherapy Trial Design Phase III, multicenter, randomized controlled trial of primary LMWH thromboprophylaxis in ambulatory cancer chemotherapy patients Patient Population 400 consenting adult solid tumor or lymphoma patients starting a new chemotherapy regimen Considered high risk based on the VTE model, ie, risk score for VTE ≥3 Study Outcomes Primary Outcomes: Symptomatic and asymptomatic VTE Secondary Outcomes: Overall mortality, bleeding complications Correlative Studies Blood for biomarkers and microarray studies Fig. 1. Study Schema. (R=randomization, H&P=history and physical examination, US=ultrasound, CT=computed tomography scan of the chest). All time points are ± 1 week. Baseline CT up to 4 weeks prior to enrollment will be accepted. Cancer and Venous Thromboembolism Conclusions VTE is a common complication of cancer and cancer treatment and is associated with considerable morbidity, mortality and costs. The US Surgeon General has recently issued a Call to Action to Prevent Deep Vein Thrombosis and Pulmonary Embolism including new research initiatives to lower the burden of this serious illness. Hospitalized medical and surgical cancer patients are at increased risk for VTE and should be considered for pharmacologic prophylaxis if no contraindication to anticoagulation is present. Cancer patients treated for documented VTE should be considered for continued anticoagulation, preferably with LMWH, for up to six months or longer in patients with active malignancy. Cancer and Venous Thromboembolism Conclusions Routine thromboprophylaxis of ambulatory cancer patients is not currently recommended. While results from prospective controlled trials are needed, thromboprophylaxis may be considered in selective high risk settings such as multiple myeloma patients receiving thalidomide or lenalidomide along with chemotherapy and/or dexamethasone. Consideration of prophylactic anticoagulation cancer patients must always balance the VTE with the increased risk of bleeding. in risk of Improved methods for the identification of ambulatory cancer patients at increased risk for VTE and targeted thromboprophylaxis are needed and under active investigation. Acknowledgments Duke University University of Rochester – Nicole Kuderer MD – Alok Khorana MD – Thomas Ortel MD – Charles Francis MD – Jeffrey Crawford MD – Mark Taubman MD – Eva Culakova PhD – Rami Komrokji, MD – Marek Poniewierski MD – Debra Wolff, MS PCNP ASCO VTE Guideline Panel Members – Anna Falanga, Co-Chair Just Wait Until Next Year……….. Official Duke University Slide for Presentations at the University of North Carolina Cancer and Thrombosis What to Look For…….. • Cancer Investigation, 2009 – Special Issue on Cancer and Thrombosis • Journal of Clinical Oncology, 2009 – Special Issue on Cancer and Thrombosis • ASCO 2009 – – Education Session on Cancer and Thrombosis 3 Chapters in the Education Book • NHLBI Trials on going at Duke/Rochester and UNC • ISTH 2009: Boston July 11-16 • 5th International Conference on Thrombosis and Hemostasis: Issues in Cancer, Stresa, Italy, April 23-25, 2010 • Any much more…………. ASCO VTE Guideline Panel Members Gary H. Lyman, MD, MPH, FRCP (Edin), Co-Chair Duke University Anna Falanga, MD, Co-Chair Ospedali Riuiniti, Bergamo, Italy Daniel Clarke-Pearson, MD University of North Carolina Christopher Flowers, MD, MS Emory University Charles W. Francis, MD University of Rochester Leigh Gates, Patient Representative University of Colorado Mohammad Jahanzeb, MD University of Tennessee Ajay Kakkar, MD, PhD Barts and The London School of Medicine ASCO VTE Guideline Panel Members Alok A. Khorana, MD University of Rochester Nicole M. Kuderer, MD Duke University Mark Levine, MD, PhD McMaster University Howard A. Liebman, MD University of Southern California David S. Mendelson, M.D. Premiere Oncology Gary Edward Raskob, PhD University of Oklahoma Paul A. Thodiyil, MD New York Methodist Hospital David Trent, MD, PhD Virginia Cancer Center ASCO Recommendations for VTE Prophylaxis in Patients with Cancer Summary Patient Group Recommended Not Recommended Hospitalized VTE prophylaxis with anticoagulants patients with cancer If bleeding or contraindication to anticoagulation Ambulatory patients with cancer receiving chemotherapy Myeloma patients receiving thalidomide or lenalidomide + chemotherapy/ dexamethasone. LMWH or adjusted dose warfarin. Otherwise, no routine prophylaxis Patients with cancer undergoing surgery Prophylaxis with low-dose UFH or LMWH Prophylaxis with mechanical methods for patients with contraindications to pharmacologic methods Consider mechanical methods when contraindications to anticoagulation. Patients with cancer with established VTE Pharmacologic treatment for at least 6 months. Consider continued anticoagulation beyond 6 months in those with active cancer. To improve survival - Lyman GH et al: J Clin Oncol 2007; 25:5490-5505 - Not recommended Symptomatic VTE in Hematopoietic Stem Cell Transplantation (HSCT) Implications for VTE Prevention ● Retrospective review of 1514 HSCT patients ● Median F/U: 642 days ● Symptomatic VTE: 75 (4.6%) – ● Catheter-related: 55 (73%) Clinical bleeding: 230 (15.2%) – Fatal bleeding: 55 (3.6%) – OR with anticoagulation: 3.1 – OR with VOD: 2.2 Gerber, D. E. et al. Blood 2008;112:504-510 Meta-analysis: Anticoagulant Prophylaxis to Prevent Symptomatic VTE Hospitalized Medical Patients • 9 studies with 19,958 patients • Anticoagulant prophylaxis: – Pulmonary embolism (PE): • • – RR = 0.38; CI 0.21-0.69 ARD = 0.25%; NNT = 400 Symptomatic DVT: • • – RR = 0.43; CI 0.26-0.71 ARD = 0.29%; NNT = 345 Fatal PE: • • – Pulmonary Embolism n=8) RR = 0.47; CI 0.22-1.00 ARD = 0.43%; NNT = 233 Major bleeding • • RR = 1.32; CI 0.73-2.37 ARD = 0.14%; NNH = 714 Dentali F, et al. Ann Intern Med. 2007;146:278-288. Major Bleeding (n=7) Risk Factors for Early Mortality in Patients Receiving Cancer Chemotherapy Variables VTE* Patient Demographics Age ECOG >1 Charlson comorbidity index >1 Body mass index [kg/m2] Stage IV Cancer Type Colorectal Small cell lung cancer Non-small cell lung cancer Ovary Breast Lymphoma Relative Dose Intensity <85% Unknown Year 2003 2004 2005 Baseline Laboratory Values WBC >11,000/mm3 Creatinine >1.5 mg/dL Alkaline phosphatase >120 U/L Protein <5.5 g/dL Albumin <3.5 g/dL Kuderer NM, et al. ASCO 2008 Hazard Ratio P value 95% CI 3.059 1.309 7.153 .010 1.021 1.287 1.338 .959 2.304 1.004 .830 .911 .927 1.509 1.038 1.996 1.966 .992 3.516 1.666 1.530 3.072 1.543 1.059 1.580 .765 .609 1.590 .565 .442 .756 3.626 3.842 5.937 4.211 2.536 3.304 .992 2.071 .617 1.132 1.595 3.789 1.166 .821 .300 .685 .461 .100 1.983 1.464 .898 .017 .260 .137 .016 <.0001 .009 .199 .365 .001 .397 .898 .224 .026 .973 .018 .039 .571 .505 .031 1.976 2.214 1.678 3.194 2.373 1.331 1.223 1.146 1.698 1.594 2.932 4.008 2.455 6.009 3.532 .001 .009 .008 <.0001 <.0001 *Time-dependent covariate Coagulation Proteases in Tumor Biology Tissue Factor/FVIIa Growth Factor Xa Invasion Thrombin Metastasis Angiogenesis Fibrin generation plays additional roles in these processes Fibrinogen Kinetics in Cancer Patients Patients: 25 patients with known advanced or active cancer Methods: Plasma and urine fractional fibrinogen catabolic rates were estimated Findings: Significantly shortened fibrinogen survival found in patients with active cancer Categories N T½ TO* Controls 6 3.89 .828 All Cancers 25 3.01 1.433 Leukemia 6 3.19 Lymphoma 4 2.88 1.881 <.05 Solid Tumor 15 2.98 1.617 <.05 GI 3 No Chemo 15 3.28 Chemo 10 2.61 .671 <.05 NS 2.52 2.234 <.05 *TO= mean turnover in mg/ml/day Lyman GH et al. Cancer 1978; 41: 1113-1122 P NS Risk of VTE in Cancer Patients by Type of Malignancy Population-based, case-control study [MEGA] of risk factors for VTE • 6 clinics in Holland • 3220 consecutive patients, 18 to 70 years, with a first DVT or PE • 2131 control participants (partners of the patients) Type of Cancer Adjusted Odds Ratio (95% CI) Hematologic 28 (4-199.7) Lung 22.2 (3.6-136.1) Gastrointestinal 20.3 (4.9-83) Breast 4.9 (2.3-10.5) Prostate 2.2 (0.9-5.4) Risk was greatest in first few months following diagnosis of cancer Patients with distant metastases and carriers of factor V Leiden mutation were are further increased risk. Blom JW, et al. JAMA. 2005;293:715-722. The Surgeon General’s Call to Action to Prevent Deep Vein Thrombosis and Pulmonary Embolism September 15, 2008 Risk Factors for Inpatient VTE: Multivariate Analysis* Characteristic OR P value Lung 1.3 <0.001 Stomach 1.6 0.0035 Pancreas 2.8 <0.001 Uterine 2 <0.001 Brain 2.2 <0.001 Age > 65 1.1 0.005 Arterial Thromboembolism 1.4 0.008 Major Comorbidities** 1.3-1.6 <0.001 Site of Cancer * Adjusted for sex, race, HBP, DM, CHF, hepatic disease (NS) ** lung/renal disease, infection, obesity Khorana et al, J Clin Oncol 2006; 24: 484-490 VTE Risk and Prevention in Multiple Myeloma Chemotherapy ± Thalidomide Zangari et al: Brit J Haematol 2004; 126: 715-721 Ambulatory Cancer Patients: Prophylaxis in Multiple Myeloma Patients • Prophylaxis with low-molecular-weight heparin (LMWH) or adjusted dose warfarin (INR~1.5) is recommended in multiple myeloma patients receiving thalidomide or lenalidomide plus chemotherapy or dexamethasone (high VTE risk) • However: – No RCTs available – Recommendation is based on extrapolation from nonrandomized trials or randomized studies in other similar high-risk categories – Well-designed RCTs are urgently needed Lyman GH et al: J Clin Oncol 2007; 25:5490-5505 VTE Risk and Prevention in Multiple Myeloma Melphalan + Prednisone ± Thalidomide VTE • No anticoagulation (first two years): 11/65 (17%) • Enoxaparin 40 mg QD for four months: 2/65 (3%) (P=.005) Palumbo A et al: The Lancet 2006; 367: 825-831 Older Age and History of Arterial Thromboembolism Chemotherapy* plus bevacizumab Chemotherapy* alone (control group) 20 ATE Rate (%) 16 12 8 4 0 Total cohort No risk factors Age ≥65 yr ATE history n=963 bev n=872 ctrl n=602 bev n=490 ctrl n=339 bev n=279 ctrl n=89 bev n=59 ctrl ATE history + age ≥65 yr n=67 bev n=46 ctrl Reduction in thrombosis Increase in bleeding ASCO Recommendations for VTE Prophylaxis in Patients with Cancer Preventing Recurrence in Cancer Patients with Established VTE 5. In patients with central nervous system malignancies and in the elderly, anticoagulation is recommended for established VTE as described for other patients with cancer . 6. Careful monitoring of anticoagulation is necessary to limit the risk of hemorrhagic complications. 7. Anticoagulation should be avoided in the presence of active intracranial bleeding or preexisting bleeding diathesis such as thrombocytopenia (platelet count <50,000/mm3) or coagulopathy. Lyman GH et al: J Clin Oncol 2007; 25:5490-5505 The CLOT Trial • multinational, open-label, randomized study Cancer patients with proximal DVT, PE or both R Control Group: dalteparin + VKA Experimental Group: dalteparin alone • treatment period 6 months (or until death) • primary endpoint: symptomatic VTE recurrence • follow-up for survival up to 12 months Lee AY, et al. N Engl J Med. 2003;349:146-153. CLOT Trial Results: Survival in Solid Tumor Patients ± metastatic disease P = 0.62 HR=0.50[.27 to .95]; P=.03 HR=1.1[.87 to 1.4]; P=.46 For patients without metastatic disease, the hazard ratio was 0.50 (95% CI, 0.27 to 0.95; P = .03) for the overall comparison between the treatment groups. For patients with metastatic disease, the hazard ratio was 1.1 (95% CI, 0.87 to 1.4; P = .46) for the overall comparison between the treatment groups. Lee, A. Y.Y. et al. J Clin Oncol; 23:2123-2129 2005 Mortality and PFS in Univariate Analysis by VTE Risk Score Categories Outcomes (at 4 months) Risk Group Low Intermed. High N=1,206 N=2,709 1.2% 5.9% 12.7% 5.6% 1.0 3.56 [1.91-6.66] 6.89 [3.50-13.57] - 93% 82% 72% 84% 1.0 2.77 [1.97-3.87] 4.27 [2.90-6.27] - N=543 All N=4,458 Overall Mortality Risk (%) HR [+/- CI] PFS Risk (%) HR [+/- CI] Kuderer NM et al; Blood 2008 (ASH 2008) VTE Risk Score Independent Predictor for: PFS Multivariate Analysis* Variables P-value HR Lower VTE Risk Score(1) Upper 0.001 1.00 <0.001 2.077 1.397 3.086 High Risk Group (III) <0.001 2.344 1.465 3.751 0.028 2.043 1.079 Patient Characteristics Progression-Free Survival Intermed. Risk Group (II) VTE(2) Progression-Free Survival 95% CI for HR 3.870 Low Intermediate .90 P < 0.001* Age 0.107 1.008 0.998 ECOG >1 0.001 1.498 1.175 Charlson >1 0.047 1.256 1.003 1.574 BMI [kg/m2] <0.001 0.962 0.944 0.981 Stage IV(3) <0.001 1.982 1.567 2.506 <0.001 0.792 0.700 0.896 P<.001 1.017 1.909 .80 High P<.001 .70 Year 0 10 20 30 40 50 60 70 80 90 100 110 120 Time (Days) *Overall test of significance *Adjusted for: Cancer Type, and Relative Dose Intensity (1) Comparison to low risk group (I) (3) Comparison to stages I-III (2) Time-dependent covariate Kuderer NM et al; Blood 2008 (ASH 2008) LMWH prophylaxis NIH trial in cancer outpatients Inclusion Criteria: Age 18 years or older A histologic diagnosis of malignancy (not basal cell or squamous cell); At planned initiation of a new systemic chemotherapy regimen (including patients starting on first chemotherapy or patients previously treated but starting on a new regimen); A risk score for VTE ≥3. Any counts meeting criteria drawn within 2 weeks prior to enrollment are considered acceptable. Exclusion Criteria: Patients will be excluded from the trial if they have any of the following: – Active bleeding or at high risk of serious bleeding complication in the opinion of the investigator – Diagnosis of primary brain tumor, multiple myeloma, acute leukemia, chronic myelogenous leukemia or myelodysplastic syndrome – Planned stem cell transplant – Life expectancy < 6 months – Known allergy to heparin or LMWH – Incapable of daily self-injection – Acute or chronic renal insufficiency with creatinine clearance < 30 mL/min – History of heparin-induced thrombocytopenia – Allergy to contrast agents – Need for anticoagulant therapy – Platelet count < 50,000/mm3 – Pregnancy Procoagulant activities Fibrinolytic activities Tumor cells Cytokines and factors Activation of coagulation Activation of vascular blood cells Falanga A: Cancer Invest 2009; 27: 105-115 growth Extracellular matrix remodeling Angiogenesis Survival of Cancer Patients Developing VTE Compared to Matched Controls Data from the Danish National Registry of Patients, the Danish Cancer Registry, and the Danish Mortality Files Control patients, who did not have VTE, were matched by – cancer type – Sex – Age – year of diagnosis Sorensen, H. T. et al. N Engl J Med 2000;343:1846-1850 One-Year Mortality Cancer with VTE 12% Cancer w/o VTE 36% HR = 2.20 [2.05-2.40] P<.0001 RCTs of Thromboprophylaxis in Ambulatory Cancer Patients Low Molecular Weight Heparin: Meta-Analysis Summary Estimates [N=6 RCTs] • Venous Thromboembolism – Relative Risk: 0.64 [95% CI: 0.44 – 0.94] – Absolute Risk Reduction: 1.8% [95% CI: 0.2% - 3.4%] • Major Bleeding – Relative Risk: 1.85 [95% CI: 0.93 – 3.68] – Absolute Risk Increase: 0.9% [95% CI: 0% - 1.8%] Kuderer NM et al: ASCO 2009 VTE Risk Score Independent Predictor for: Mortality Multivariate Analysis Variables VTE Risk Score(1) P-value HR* 95% CI for HR 0.028 Intermed. Risk Group (II) 0.025 2.222 1.106 4.464 High Risk Group (III) 0.008 2.926 1.332 6.428 <0.001 4.472 1.928 10.370 Age 0.026 1.018 1.002 1.035 ECOG >1 0.027 1.613 1.055 2.464 Charlson >1 0.014 1.582 1.096 2.284 BMI [kg/m2] <0.001 0.941 0.910 0.973 Stage IV(3) <0.001 2.659 1.755 4.028 0.016 0.771 0.624 0.953 VTE(2) Patient Characteristics Year *Adjusted for: Cancer Type, and Relative Dose Intensity (1) Comparison to low risk group (I) (3) Comparison to stages I-III (2) Time-dependent covariate Kuderer et al. Oral Presentation ASH 2008 Cancer and Venous Thromboembolism The Need for Risk Stratification 4.5 Chemotherapy End of Life 4 3.5 Relative Risk 3 2.5 Hospitalization Metastasis Diagnosis 2 1.5 Remission 1 Average Risk 0.5 0 1 2 3 Time 4 5 6 Importance of Guidelines to Clinical Outcomes “Clinicians armed with appropriate assessments and the best evidence-based practice guidelines can reduce some of the unpleasant and frequent side-effects that often accompany cancer and chemotherapy treatment, obtain the best possible clinical outcomes, and avoid unnecessary costs.” Statement from Centers for Medicare and Medicaid Services, August 2005 Candidate Biomarkers • • • • • Platelet count Leukocyte count Tissue factor P-selectin Others (D-dimer, C-reactive protein) Soluble P-Selectin and VTE in Cancer Ay C, et al. Blood. 2008;112:2703-2708 Mechanisms for ESAs to Increase Thrombosis Rheological effects of increased or increasing red cell mass Young red cells in circulation augment platelet reactivity (red cell–platelet interaction) ESAs synergize with TPO to activate platelets (ESA–TPO interactions) Direct, receptor-mediated effects on endothelium that enhance interaction with platelets (ESA–endothelial interactions) TPO, thrombopoietin Lancet 2003;362:1265 Highlights from ASCO 2009 Advances in Supportive Care Managing Disease and Treatment-Related Complications Venous Thromboembolism and Thromboprophylaxis Low-molecular-weight heparin for venous thromboprophylaxis in ambulatory cancer patients: A meta-analysis Nicole M. Kuderer, Alok A. Khorana, Charles W. Francis et al Duke University, Durham, NC; University of Rochester, Rochester, NY • Literature Search: – Medline, EMBASE, Cochrane Library, Conference Proceedings, Hand Searching of References • Major Inclusion Criteria: – RCT of LMWH VTE prophylaxis in adult ambulatory cancer patients – Treatment Group: LMWH – Control Group: placebo or no Rx • Major Exclusion Criteria: – Non-cancer patients – Non-randomized trials – Surgery, Catheter trials, or intraportal heparin infusion – Combination of anticoagulants Venous Thromboembolism Study name Statistics for each study Relative Risk [95% CI] Relative Risk Lower limit Upper limit Z-Value FAMOUS 0.775 0.211 2.840 -0.385 0.700 TOPIC-1 1.006 0.360 2.808 0.011 0.991 TOPIC-2 0.529 0.251 1.111 -1.681 0.093 PRODIGE 0.659 0.292 1.489 -1.003 0.316 PROTECHT 0.495 0.217 1.132 -1.665 0.096 Sideras 0.824 0.231 2.938 -0.299 0.765 0.642 0.441 0.936 -2.301 0.021 Overall Overall p-Value 0.1 0.2 0.5 1 Favors Prophylaxis 2 5 10 Favors Control Major Bleeding Study name Statistics for each study Relative Lower Risk limit Upper limit Relative risk [95% CI] Z-Value p-Value FAMOUS 2.906 0.119 70.874 0.655 0.513 TOPIC-1 7.040 0.366 135.290 1.294 0.196 TOPIC-2 1.607 0.534 4.837 0.844 0.399 PRODIGE 4.394 0.523 36.887 1.364 0.173 PROTECHT5.457 0.303 98.434 1.150 0.250 Sideras 0.412 0.083 2.051 -1.083 0.279 Overall 1.846 0.927 3.675 1.744 0.081 0.1 0.2 0.5 Favors Prophylaxis 1 2 5 10 Favors Control Risk - Benefit Comparison VTE – Prophylaxis with LMWH Venous Thromboembolism Study name Statistics for each study Absolute risk difference [95% CI] Risk Standard Lower Upper difference error Variance limit limit Z-Value p-Value Benefit Harm FAMOUS -0.006 0.016 0.000 -0.037 0.025 -0.385 0.700 TOPIC-1 0.000 0.021 0.000 -0.040 0.041 0.011 0.991 TOPIC-2 -0.040 0.023 0.001 -0.085 0.006 -1.723 0.085 PRODIGE -0.047 0.047 0.002 -0.139 0.045 -1.002 0.316 PROTECHT -0.015 0.010 0.000 -0.033 0.004 -1.519 0.129 -0.013 0.042 0.002 -0.095 0.070 -0.300 0.764 -0.018 0.008 0.000 -0.034 -0.002 -2.265 Sideras Overall Venous Thrombosis ARD* Major Bleeding Events ARD* 0.023 All Bleeding Events ARD*1 -0.25 -0.13 0.00 Favors Prophylaxis 0.13 0.25 Favors Control Major Bleeding Study name 1.8% ↓ 1Kuderer 0.9% ↑ et al. Cancer 2007 2.4% ↑↑ Statistics for each study Relative Lower Risk limit Relative risk [95% CI] Upper limit Z-Value p-Value FAMOUS 2.906 0.119 70.874 0.655 0.513 TOPIC-1 7.040 0.366 135.290 1.294 0.196 TOPIC-2 1.607 0.534 4.837 0.844 0.399 PRODIGE 4.394 0.523 36.887 1.364 0.173 PROTECHT5.457 0.303 98.434 1.150 0.250 -1.083 0.279 Sideras 0.412 0.083 Overall 1.846 0.927 2.051 3.675 1.744 0.081 0.1 *ARD = Absolute Risk Difference 0.2 0.5 Favors Prophylaxis 1 2 5 10 Favors Control Conclusions VTE – Prophylaxis with LMWH • While ambulatory cancer patients experienced a 36% relative risk reduction in VTE with LMWH, the average absolute risk reduction for VTE was only 1.8%. • Concern remains about the potential increase in major bleeding with an absolute risk increase in major bleeding of 0.9%. • Major bleeding was not a primary outcome in any of the studies and were not powered to adequately assess major bleeding. • Weighing risks and benefits, routine VTE prophylaxis in the general outpatient cancer population cannot be recommended at this time. • Studies are ongoing to better identify cancer outpatients at increased risk for VTE, in whom prophylaxis may have a more favorable risk-benefit ratio. ASCO Guidelines for Thromboprophylaxis Hospitalized cancer patients Should be considered candidates for VTE prophylaxis in the absence of contraindications Surgical cancer patients All patients undergoing major surgical intervention for malignant disease should be considered for prophylaxis Prophylaxis should be continued for at least 7-10 days postoperatively and may be extended into the post discharge period for selected high-risk patients Ambulatory cancer patients Routine prophylaxis not recommended Exception: Patients receiving thalidomide or lenalidomide with chemotherapy or dexamethasone Lyman et al. JCO 2007 ASCO Guidelines for Thromboprophylaxis Hospitalized cancer patients Should be considered candidates for VTE prophylaxis in the absence of contraindications Surgical cancer patients All patients undergoing major surgical intervention for malignant disease should be considered for prophylaxis Prophylaxis should be continued for at least 7-10 days postoperatively and may be extended into the post discharge period for selected high-risk patients Ambulatory cancer patients Routine prophylaxis not recommended Exception: Patients receiving thalidomide or lenalidomide with chemotherapy or dexamethasone Risk Model Patient Characteristic Score Site of Cancer Very high risk (stomach, pancreas) High risk (lung, lymphoma, gynecologic, GU excluding prostate) Platelet count > 350,000/mm3 2 1 1 Hb < 10g/dL or use of ESA 1 Leukocyte count > 11,000/mm3 1 BMI > 35 kg/m2 1 Khorana AA et al. Blood 2008 VTE Prediction Risk Score Chemotherapy – Associated Thrombosis Development cohort Validation cohort 8% .10 Rate of VTE (%) 6% 5% 7.1% High Venous Thromboembolism 7% .08 6.7% P < 0.001* .06 P<.001 .04 Intermediate .02 P<.001 4% Low 0.00 0 3% 10 20 40 *Overall test of significance 50 60 70 80 90 100 110 120 Time (Days) 1.8% 2% 1% 30 2.0% 0.8% 0.3% 0% n=734 n=374 RISK SCORE: Low (0) n=1,627 n=842 Intermediate (1-2) n=340 n=149 High (>3) Khorana AA et al. Blood. 2008; 111:4902-4907 Mortality and PFS By VTE Risk Score Outcomes Low Risk Intermediate Risk High Risk All N=1,206 N=2,709 N=543 N=4,458 1.2% 5.9% 12.7% 5.6% Mortality Risk (%) HR [+/- CI] 1.0 3.6 [1.9-6.7] 6.9 [3.5-13.6] - Progression-free survival Risk (%) HR [+/- CI] 93% 82% 72% 84% 1.0 2.8 [2-3.9] 4.3 [2.9-6.3] - Kuderer NM et al. ASH 2008 PHACS Study LMWH prophylaxis x 12 weeks with 4-weekly screening US and start/end CT chest Patients starting chemotherapy Risk score ≥3 R Observe x 12 weeks with 4-weekly screening US and start/end CT chest Sites: Duke, Duke Oncology Network, Univ of Rochester R01 HL095109-01 A prospective, randomized trial of chemotherapy with or without the low molecular weight heparin enoxaparin in patients with advanced pancreatic cancer: Results of the CONKO 004 trial H. Riess, U. Pelzer, G. Deutschinoff, B. Opitz, M. Stauch, P. Reitzig, S. Hahnfeld, A. Hilbig, J. Stieler, H. Oettle Randomization Chemotherapy Chemotherapy + Enoxaparin Treatment for 3 months: VTE, Bleeding, RR, PFS, OS Chemotherapy Chemotherapy + Enoxaparin E 1 mg/kg/d Primary endpoint E 40 mg/kg/d until PD Response evaluation at least every 12 weeks: VTE, Bleeding, RR, PFS, OS A prospective, randomized trial of chemotherapy with or without the low molecular weight heparin enoxaparin in patients with advanced pancreatic cancer: Results of the CONKO 004 trial H. Riess, U. Pelzer, G. Deutschinoff, B. Opitz, M. Stauch, P. Reitzig, S. Hahnfeld, A. Hilbig, J. Stieler, H. Oettle Randomization Chemotherapy Chemotherapy + Enoxaparin Treatment for 3 months: Chemotherapy VTE , Bleeding, RR, PFS, OS Chemotherapy + Enoxaparin E 1 mg/kg/d Primary endpoint E 40 mg/kg/d until PD Response evaluation at least every 12 weeks: VTE, Bleeding, RR, PFS, OS CONKO-004: Chemotherapy Favorable results in randomized phase II/III in patients with good PS: with Gem/CDDP or Gem/FA/5-FU and Gem/Cap Gem/CDDP/5-FU and Gem/FA/5-FU/CDDP with remarkable RR and 1year OS Patient allocation according to Karnofsky-PS (KPS) and plasma creatinine level KPS ≥ 80% + creatinine ≤ ULN KPS 60-70% or creatinine > ULN Gemcitabine (1000 mg/m2) Gemcitabine (1000 mg/m2) Folinic acid (100 mg/m2) d1, 8, 15; 29 5-FU (750 mg/m2 24 h CI) CDDP (30 mg/m2) d1, 8; 22 Results: VTE and Major Bleeding Observation Enoxaparin Patients (N) 152 160 VTE (at 3 months)* Major Bleeding (at 3 months) 9.9% 2.6% 1.2% 3.8% VTE (at 30.4 months)** 15.5% 5% Major Bleeding (at 30.4 months) 9.9% 6.3% 29 weeks 31 weeks Median survival *p<0.01; **p<0.05 Results: VTE and Major Bleeding Observation Enoxaparin Patients (N) 152 160 VTE (at 3 months)* Major Bleeding (at 3 months) 9.9% 2.6% 1.2% 3.8% VTE (at 30.4 months)** 15.5% 5% Major Bleeding (at 30.4 months) 9.9% 6.3% 29 weeks 31 weeks Median survival *p<0.01; **p<0.05 Results: VTE at 3 Months Venous thromboembolic events Observation N= 162 Enoxaparin N= 150 All Pulmonary embolism 2 0 2 Proximal leg DVT 9 2 11 Distal leg DVT only 2 0 2 Upper extremity DVT 3 0 3 All (VTE) 16 2 18 All (Patients)* 15 2 17 Event Results: Relative VTE rates ■ Gem ■ GFFC 16 n=5 Percent (%) 14 Δ=12.4%;RRR=79%;P=.300 12 10 8 n=10 6 4 n=1 2 n=1 0 Observation Enoxaparin Δ=6.6%;RRR=90%;P=.025 CONKO-004: Summary • • • • • • Major Limitations Unusual study design Non-standard chemotherapy Chemo allocated by PS/creat. Small study: trial stopped early Paradoxical major bleeding results No information on catheters • • • • • Conclusions Enoxaparin (1mg/kg/day) significantly reduces VTE No OS improvement High overall major bleeding Unusual study design Clinical relevance of data? – Reducing non-PE VTE – Setting of high major bleeding • ? Long-term complications: – Osteoporosis – HIT