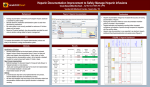
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
PACKAGE INSERT 1. PROPRIETARY NAME (AND DOSAGE FORM) Heparin Sodium-Fresenius 5,000 IU/1 ml (Injection) 2. COMPOSITION 5 ml vial containing 5,000 IU /1 ml Heparin Mucosal Preservative: Chlorocresol 0.1% m/v Water for injection to 1 ml Heparin is obtained from porcine intestinal mucosa. 3. PHARMACOLOGICAL CLASSIFICATION A 8.2 Anticoagulants. 4. PHARMACOLOGICAL ACTION Heparin inhibits the clotting of blood both in vitro and in vivo. Whole blood clotting time, thrombin time and one-stage prothrombin time are prolonged, and thromboplastin generation is abnormal. Clotting time is proportional to the concentration of the medicine in the blood. However, with therapeutic doses bleeding time is usually unaffected and a patient can carry on normal activities, such as shaving, without danger of bleeding. The anticoagulant action of heparin requires the presence of a plasma a-globulin, referred to as “heparin cofactor”, a substance that appears to be identical with normal plasma antithrombin (antithrombin III). Heparin does not block prothrombin synthesis in the liver as do the oral anticoagulants but it does inhibit factors involved in the conversion of prothrombin to thrombin. This action is probably exerted by the facilitation of the formation of complexes of the heparin cofactor (antithrombin) with each of the four activated proteases of the coagulation cascade (activated factors IX, X, XI and XII). A similar heparin-stimulated reaction also occurs between antithrombin and thrombin. The detailed mechanism of this phenomenon may involve a heparin-induced conformational change of the inhibitor. It requires 30 to 40 times more heparin to inhibit the action of formed thrombin than it does to prevent thrombin formation. Therefore the prevention of thrombin formation is probably its primary effect. Heparin is not effective after oral or sublingual administration, but it is well absorbed after subcutaneous injection. In the blood it is evenly distributed between white cells and plasma. Heparin disappears exponentially from the circulation at a rate dependent upon the dose. The half-lives of 100, 200 and 400 units/kg, injected intravenously, are 56, 96 and 152 minutes respectively. Heparin is metabolized by the liver and a partially degraded, weakly active form of heparin (uroheparin) is excreted in the urine; after very large intravenous doses, up to 50% of nonmetabolized heparin may appear in the urine. The exact mechanism of renal elimination is unknown. 5. INDICATIONS Heparin is used as an anticoagulant in the treatment of arterial and venous thrombosis and prevention of thromboembolic complications after surgery. 6. CONTRAINDICATIONS Heparin sodium should not be used in patients with severe thrombocytopenia, in whom suitable blood coagulation tests e.g. the whole blood clotting time, partial thromboplastin time, etc. could not be performed at appropriate intervals (this contraindication refers to full-dose heparin; there is usually no need to monitor coagulation parameters in patients receiving low-dose heparin). Heparin sodium should not be used in patients with an uncontrollable active bleeding state, except when this is due to disseminated intravascular coagulation. Conditions where hemorrhage is a particular risk: • Aneurysm, cerebral or aortic • Risk of abortion • Recent childbirth • Pericarditis • Severe vasculitis • Active cavitating tuberculosis • Visceral carcinoma if there is a possibility of intracranial metastasis • Peptic ulceration • During or after eye, brain or spinal cord surgery or trauma • Prior to lumbar puncture or regional anesthetic block • Surgical or traumatic wounds resulting in large open surfaces • Severe renal function impairment • Severe hepatic function impairment • Esophageal varices • Subacute bacterial endocarditis 7. Hypersensitivity: Avoid use in hypersensitive patients unless benefits outweigh risks. WARNINGS Heparin should not be used for intramuscular injection. Due to the danger of physical/chemical incompatibilities, heparin may not be administered drawn up with other medication in a hypodermic syringe or an infusion. Hemorrhage: Hemorrhage can occur at any site in patients receiving heparin. In the event of an unexplained fall in hematocrit or blood pressure or any other unexplained symptom, consideration must be given to possible hemorrhage. Heparin must be used cautiously in patients suffering from diseases with a hemorrhage risk for example: • Cardiovascular: severe/uncontrolled hypertension • Surgical: during and immediately following spinal tap, spinal anesthesia or major surgery involving the brain, spinal cord or eye • Hematologic: conditions associated with increased bleeding tendencies such as hemophilia, thrombocytopenia or vascular purpuras • Gastrointestinal: ulcerative lesions and continuous tube drainage of stomach or small intestine • Other: menstruation, liver disease with impaired hemostasis Coagulation testing: Frequent blood coagulation tests must be performed on patients receiving heparin and the product discontinued if necessary. Thrombocytopenia: Thrombocytopenia has been reported to occur in patients receiving heparin with a reported incidence of 0 to 30%. Platelet counts should be obtained at baseline and periodically during heparin administration. Mild thrombocytopenia (count greater than 100,000/mm3) may remain stable or reverse even if heparin is continued. If the count falls below 100,000/mm3 or if recurrent thrombosis develops (see Heparin-induced Thrombocytopenia and Heparin-induced Thrombocytopenia and Thrombosis), the heparin product should be discontinued and, if necessary, an alternative anticoagulant administered. Heparin-induced Thrombocytopenia (HIT) and Heparin-induced Thrombocytopenia and Thrombosis (HITT): HIT is a serious antibodymediated reaction resulting from irreversible aggregation of platelets. HIT may progress to the development of venous and arterial thromboses, a condition referred to as HITT. Thrombotic events may also be the initial presentation for HITT. These serious thromboembolic events include deep vein thrombosis, pulmonary embolism, cerebral vein thrombosis, limb ischemia, stroke, myocardial infarction, mesenteric thrombosis, renal arterial thrombosis, skin necrosis, gangrene of the extremities that may lead to amputation and possibly death. Delayed onset of HIT and HITT: HIT and HITT can occur up to several weeks after discontinuation of heparin therapy. Patients presenting with thrombocytopenia or thrombosis after discontinuation of heparin treatment should be evaluated for HIT and HITT. 8. INTERACTIONS Other platelet aggregation inhibitors: Aspirin, sulfinpyrazone: inhibition of platelet function by these agents may lead to hemorrhage because it impairs a homeostatic mechanism on which heparin treated patients depend to prevent bleeding, hypoprothrombinemia induced by large [antirheumatic] doses of aspirin, and the potential occurrence of gastrointestinal ulceration or hemorrhage during therapy with NSAIDs, aspirin, sulfinpyrazone, ticlopidine or clopidogrel may also cause increased risk of bleeding in patients receiving heparin therapy. Cefamandole or cefoperazone or cefotetan or plicamycin or valproic acid: these medications may cause hypoprothrombinemia, in addition, plicamycin or valproic acid may inhibit platelet aggregation; concurrent use with heparin may increase the risk of hemorrhage and is not recommended. Methimazole or propylthiouracil: these medications may cause hypoprothrombinemia (which may enhance the anticoagulant effect of heparin and increase the risk of bleeding). Probenecid: probenecid may increase and prolong the anticoagulant effect of heparin. Thrombolytic agents: Alteplase: (tissue-type plasminogen activator, recombinant), antistreptase (anisoylated plasminogen-streptokinase activator complex; APSAC), streptokinase, urokinase: concurrent or sequential use with heparin increases the risk of bleeding complications; although heparin is sometimes given before, and is usually given to decrease the risk of re-occlusion following thrombolytic therapy, caution and especially careful monitoring of the patient is recommended. 12-1338/01-13 Nitroglycerine: intravenous infusion of nitroglycerine might cause a reduction of the effectiveness of heparin, therefore close controls of partial thromboplastin time (PTT) together with heparin dosage adjustment are required. When alkaline medications such as tricyclic psychotropics, antihistamines and quinine are concomitantly administered, salt formation with heparin can cause loss of efficacy of both drugs. Heparin shows numerous interactions with other preparations, whose clinical significance is being evaluated differently. 9. PREGNANCY AND LACTATION Heparin does not cross the placenta and therefore adverse effects to the fetus would not be expected. Heparin is considered safer to the fetus than warfarin when used during pregnancy. Heparin has not been shown to cause birth defects or bleeding problems in the baby. However, use during the last three months of pregnancy or during the month following the baby’s delivery may cause bleeding problems in the mother, and therefore monitoring is required. The use of epidural anesthesia during labor, for women being medically treated for anticoagulation, is absolutely contraindicated. Heparin does not pass into breast milk. 10. DOSAGE AND DIRECTIONS FOR USE Heparin Sodium-Fresenius is given intravenously, preferably by continuous infusion, or by deep subcutaneous injection. The usual practice is to give an initial intravenous injection of 12,500 units of heparin, followed by doses of 10,000 units every 4 hours to maintain the clotting time, tested not less than 3 hours after the last injection, at about 3 times the pretreatment figure. The dose for this purpose usually ranges from 6,000 to 12,000 units. For continuous infusion 10,000 to 20,000 units of heparin is added to 1 liter of Dextrose injection or Sodium chloride injection and started at about 20 drops per minute. A suggested initial dose for children is 50 units per kg body mass by intravenous infusion in Dextrose injection 5% increased to 100 units per kg every 4 hours to keep the clotting time at 20 to 30 minutes. It is advisable to only use high grade needles with a gauge of 22 to 25, when extracting from the vial. DO NOT USE PREVIOUSLY USED NEEDLES. Pain at the site of injection may be minimized by the addition of 2% solution of procaine hydrochloride. If blood transfusions are required during anticoagulant therapy, 3 units of heparin per ml may be added to the transfused blood in addition to the dose already being administered. Bleeding from the site of operation is unlikely if heparin is started after the fourth postoperative day. For treatment of venous thromboembolism: an intravenous loading dose of 5,000 units (10,000 may be required in severe pulmonary embolism) is followed by continuous intravenous infusion of 1,000 to 2,000 units/hour or subcutaneous injection of 15,000 units every 12 hours. Alternatively, intermittent intravenous dose of 5,000 to 10,000 units every 4 to 6 hours undiluted or diluted in 50 to 100 ml of Dextrose 5% in water or Sodium Chloride 0.9% is suggested. Children and adolescents are given a lower intravenous dose followed by maintenance with continuous infusion of 15-25 units/kg/hour or subcutaneous injection of 250 units/kg every 12 hours. For prophylaxis of postoperative venous thrombo-embolism: subcutaneous doses used are 5,000 units 2 hours before surgery then 8-12 hours for 7 days or until the patient is ambulant. Similar doses are used to prevent thromboembolism during pregnancy in women with a history of deep-vein thrombosis or pulmonary embolism; the dose may need to be increased to 10,000 units every 12 hours during the third trimester. 11. SIDE EFFECTS AND SPECIAL PRECAUTIONS Side-effects: Heparin can give rise to hemorrhage as a consequence of its action. It can also cause thrombocytopenia, either through a direct effect or through an immune effect producing a platelet-aggregating antibody. Consequent platelet aggregation and thrombosis may therefore exacerbate the condition being treated. Heparin-induced Thrombocytopenia (HIT) and Heparin-induced Thrombocytopenia and Thrombosis (HITT) and delayed onset of HIT and HITT may occur. Discontinuation of heparin therapy with immediate corrective treatment action is required if this happens. The patient must be informed that he must not be treated with drugs containing heparin in the future. Adrenal hemorrhage with subsequent acute adrenal insufficiency, can occur. Discontinuation of heparin therapy with immediate corrective treatment action is required if this happens. Ovarian hemorrhage has occurred in women of reproductive age receiving short to long-term therapy. This can be fatal if not recognized and treated. Retroperitoneal hemorrhage can occur even if clotting time is not prolonged. Hypersensitivity reactions may occur, as may local irritant effects, and skin necrosis. General hypersensitivity reactions may manifest as chills, fever, urticaria, asthma, rhinitis, lacrimation, headache, nausea, vomiting, articular pains, pruritus, dyspnea, bronchospasm, decrease of blood pressure, anaphylactoid reactions including shock. Itching and burning, especially on plantar side of feet, may occur. Alopecia and osteoporosis resulting in spontaneous fractures have occurred after prolonged use of heparin. Increased liver transaminases level may occur. Special precautions: Since heparin has caused thrombocytopenia with severe thromboembolic complications, platelet counts should be monitored in patients receiving heparin for more than a few days. A test dose has been recommended for patients with a history of allergy. Heparin inhibits the secretion of aldosterone which may cause hyperkalemia. Plasma potassium levels should be monitored in those patients who are susceptible to hyperkalemia (for example: patients who are concomitantly treated with drugs that increase serum potassium level, diabetes mellitus, etc.), especially when receiving heparin for more than 7 days. The problem is normally resolved with the discontinuation of heparin. Priapism has been associated with heparin administration. Dosage of heparin may need to be reduced in old people; elderly women appear to be especially susceptible to hemorrhage after heparin administration. Heparin resistance: Increased resistance to heparin is frequently encountered in fever, thrombosis, thrombophlebitis, infections with thrombosing tendencies, myocardial infarction, cancer and in post-surgical patients. 12. KNOWN SYMPTOMS OF OVERDOSAGE AND PARTICULARS OF ITS TREATMENT The chief side-effect of heparin is hemorrhage. Careful laboratory control is necessary. Bleeding may be encountered from an unsuspected lesion, such as a peptic ulcer. The hemorrhagic complications recorded include hematuria, hemarthrosis, wound hematoma and gastrointestinal bleeding. The hemorrhage may produce a hematoma in the surgical wound, but this is rarely serious if infection is prevented and larger accumulations of blood are aspirated. Mild effects of heparin overdosage usually respond to simple withdrawal of the medicine. When clinical circumstances (bleeding) require reversal of neutralization of heparin effect the use of the specific heparin antagonist, protamine sulphate, by slow infusion is imperative. No more than 50 mg should be administered, very slowly, in any 10 minutes period. 1 mg of protamine sulphate neutralizes approximately 100 IU of heparin. The amount of protamine required decreases over time as heparin is metabolized. Although the metabolism of heparin is complex, it may, for the purpose of choosing a protamine dose, be assumed to have a half life of about half an hour after intravenous injection. Nevertheless, the required protamine sulphate dose varies according to the time of heparin administration and dose administered. It is important to avoid overdosage of protamine sulphate because protamine sulphate itself has anticoagulant properties. For additional information see the labeling of protamine sulphate injection products. 13. IDENTIFICATION A clear colorless or straw-colored liquid in amber glass vials, free from turbidity and from matter which deposits on standing. 14. PRESENTATION 1 ml and 5 ml amber glass vials packed in packs of 10. 15. STORAGE INSTRUCTIONS Store below 25ºC. Do not freeze. Keep out of reach of children. 16. REGISTRATION NUMBERS Heparin Sodium-Fresenius 5,000 IU /1 ml 105.41.28959.00 17. NAME AND BUSINESS ADDRESS OF MANUFACTURER BODENE (PTY) LIMITED trading as Intramed 6 Gibaud Road Port Elizabeth 6001 South Africa 18. IMPORTER Trima Israel Pharmaceutical Products Maabarot Ltd., Maabarot 4023000, Israel For Medic-Trim Healthcare Ltd. The format of this leaflet was determined by the Ministry of Health and its content was checked and approved by it. 12-1338/01-13 9207910 PL 0113D