Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
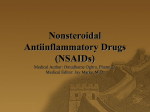
There is an urgent need for national guidelines on the safe use of NSAIDs in patients with a history of IHD, write Caroline O’Connor and Judith Kavanagh 40 FORUM September 2013 Figure 1: Indication for NSAID prescribing 35 31 30 25 22 19 20 15 15 10 10 7 4 5 es s is lln li ra Vi ar at m m fla In M isc or el y la ck ne th ou rit s in pa ed sp Pa in ,n ot te Ba ec rth oa al Os et el sk lo cu ifi rit pa is in 0 us Recent evidence in a large Danish cohort suggests that even short-term (less than one week) use of nonsteroidal anti-inflammatory drugs (NSAIDs) in those with a previous history of myocardial infarction (MI), significantly increases recurrent MI and risk of death from MI.1 This research, as well as a review carried out in October 2012 by the European Medicines Agency, indicates an increase in the risk of cardiovascular adverse effects with diclofenac compared with other non-selective NSAIDs, similar to the risk with COX-2 inhibitors.2 The Danish study showed that diclofenac was associated with a higher risk of death at the beginning of a course of treatment than rofecoxib, which was withdrawn from the market in 2004 due to the increased risk of stroke/ MI. The National Medicines Information Centre (NMIC) and the Irish Medicines Board have highlighted this research in their recent bulletins.3,4 NSAIDs are commonly prescribed in primary care.5 The latest data expands on previous studies of NSAID safety, and raises several important questions for GPs. What are the indications for NSAID prescribing in the primary care setting? For what duration should we prescribe them? Could safer alternatives be considered? And how common is the problem of NSAID prescribing in those with documented ischaemic heart disease (IHD), or with significant risk factors for IHD? Aims We carried out an analysis of the prescribing of NSAIDs in a large Dublin general practice, by examining: • Individual agents favoured • Indication • Duration • The concomitant prescribing of paracetamol. We set out to identify the number of patients who had a history of IHD or a significant risk factor for this, and who were prescribed NSAIDs. We aimed to address whether there is a need for prescribing guidelines on the use of NSAIDs in those with IHD. Methods The clinic’s active patient list (n=10,000) was studied by examining the practice management software to identify patients over 50 years of age who had been prescribed NSAIDs for any duration, over a two-month period in late 2012. Those with documented IHD as well as those with diabetes and/or hypertension were identified. A documented history of IHD was taken to mean previous diagnosis of angina, myocardial infarction, coronary artery stenting or coronary artery bypass grafting (CABG). M Research Forum Caution urged in use of NSAIDs in heart patients All of the prescribed NSAIDs at the clinic were included (diclofenac, ibuprofen, mefenamic acid, naproxen, etoricoxib and celecoxib). A record was kept of the indication for treatment and the duration of prescription, as well as whether the patient was also prescribed paracetamol. Results Demographics, agents prescribed, duration of prescription Of the 108 patients prescribed NSAIDs during the period of the study, 45 were male (42%). Ages ranged from 50-87 years. Diclofenac was the NSAID prescribed in 60/108 (56%) of cases (includes four patients prescribed Arthrotec, a combination of diclofenac and misoprostol), naproxen in 13/108 (12%) of cases (includes 12 patients prescribed Vimovo, a combination of naproxen and esomeprazole), ibuprofen in 11/108 (10%), mefenamic acid 11/108 (10%) and etoricoxib or celecoxib 14/108 (13%). IHD/risk factors for IHD Some 39/108 (36%) patients had established ischaemic heart disease or risk factors for cardiovascular disease at the time they were prescribed NSAIDs. Hypertension was the risk factor in 19/108 cases (18%), diabetes in 6/108 (5.5%), hypertension and diabetes in 6/108 (5.5%), IHD in 4/108(4%), previous MI in 2/108 (2%) and previous coronary artery bypass grafting in 1/108 (<1%). The mean duration of treatment in the 39 patients with IHD was 265 days and 22/39 (56%) were prescribed NSAIDs for longer than one month; 6/39 (15%) were prescribed NSAIDs for a year or longer. Indications for NSAID prescribing, and prevalence of concomitant paracetamol prescription Figure 1 displays the indications for the NSAIDs prescribed in the 108 patients. Some 29 of the 108 patients (27%) were concomitantly prescribed paracetamol. For those prescribed NSAIDs for longer than one month, 17/59 (29%) were also prescribed paracetamol. Discussion The safety of prescribing NSAIDs even for short duration (<1 week) has been challenged.1 It is likely that our study underestimates those with, or at risk of, IHD. The analysis is reliant on correct coding of risk factors. In addition, we have not identified those with hyperlipidaemia or those who smoke. Indeed, advancing age and sex in themselves can each independently be considered inherent risk factors. Bearing these factors in mind, it is likely that the number of patients at higher risk of cardiovascular events is underestimated in our study. It is disconcerting that diclofenac is the most commonly prescribed NSAID in this study. When diclofenac was specifically investigated in the Danish study, it was noted that the increased risk of death and MI became apparent immediately after patients start to take it, and the risk persisted throughout the course of treatment. It was shown that naproxen and ibuprofen were not as high risk as diclofenac. Diclofenac was prescribed as the preferred agent in 53.9% of (NSAID) prescriptions filled in Ireland in 2010, making it by far the most commonly prescribed NSAID.6 This is clearly represented in the data gathered in this study, where it can be seen that 56% of NSAID prescriptions were for diclofenac. Many indications for NSAIDs in this study do not have an underlying inflammatory component. Nearly all patients Forum Research would likely benefit from either replacing the NSAID with paracetamol, or the addition of paracetamol to their NSAID prescription with a view to limiting the cumulative dose of the latter. Although NSAIDs have been shown to be superior to paracetamol in their analgesic effect, this difference is small.7 As an example, recent recommendations in treating osteoarthritis do not advocate NSAIDs over paracetamol.8 Conclusion In light of the growing evidence implicating NSAIDs in cardiovascular risk, and the prevalence of NSAID prescribing in the ‘at-risk’ group, there is a need for alternatives to NSAIDs. Many current recommendations, including very reputable sources, appear out of date; for example, the NHS Evidence Clinical Knowledge Summary9 dates from 2008, although an update is imminent. We contend that many patients could safely be prescribed paracetamol, as a trial, instead of or in addition to their NSAID. If NSAIDs cannot be avoided, alternatives to diclofenac, such as ibuprofen or naproxen should be considered. On the basis of this study, a strong case can be made that urgent national guidelines should be introduced to assist physicians in the safer prescribing of these medications. Caroline O’Connor is a GP registrar and Judith Kavanagh is in general practice at Mercer’s Medical Centre, Dublin. The authors would like to thank all the staff at Mercer’s Medical Centre, RCSI and the Mercer’s Foundation References on request