Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
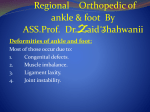
Mr. Zacharia Kimengich Senior Orthopedic Trauma Technician Kenyatta National Hospital Accident & Emergency BONES OF THE FOOT Congenital talipes equino varus (CTEV)for short is commonly known as clubfoot. This is a condition where a child presents with either one or both feet pointing downwards and turns inwards It is most common in male children compared to female children. The clubfoot is a complex deformity that is rapidly apparent at birth and in some cases is diagnosed by prenatal ultrasound. Clubfoot is a major disabler of children around the world, 150,000200,000 babies with clubfoot are born each year worldwide. The bones and joints of the foot deform and child experience complications, due to lack of awareness or knowledge from parents. It is the most common congenital problem leading to locomotor disability. Approximately80% of children born with a clubfoot deformity are born in the developing continents like Africa, and the large Majority of these do not have access to appropriate medical care. In Kenya the prevalence is 50%. Idiopathic Clubfoot Secondary clubfoot Neuropathic clubfoot Syndromic clubfoot Postural clubfoot Metatarsus adductus Not a clubfoot The exact cause of club foot is not known. An abnormality of the tendons and ligaments in the foot causes an abnormal structure and position of the foot. In some children, bones may also be normal in terms of shape, size or position. There may be a link to maternal smoking during pregnancy. If the foot is abnormally positioned in the uterus during pregnancy, it may not grow into a normal shape, but this is not usually considered true club foot Club foot may in rare instance be associated with spinal deformities such spinal bifida or other neuromuscular disease: however, in these cases, the foot is usually more deformed Remained undiagnosed at birth Treatment unavailable locally Lack of awareness of available treatment The treatment given was ineffective Other reasons: cultural beliefs The physical appearance of the clubfoot may also vary. One or both feet may be affected. Feet turning inwards Tightness in the calf muscles For structural: the foot has decreased joint range of the movement. Resting of the foot on its outer border Rigidity and other changes in the movement of the foot “The most common disabling congenital, orthopaedic condition”. Clubfoot Incidence: 1:1000 new born Babies with Clubfeet: 1200 per year Half of those affected both feet A lot of children with neglected clubfoot M>F Rt > Lt in unilateral cases Functional pain-free foot Plantigrade foot, with good mobility No need for modified shoes Most ideal: • Conservative, early treatment • (below 2 years of age-Ponseti Method) Other Options: • Surgery For best outcomes, patients should be identified and treated early. Above knee plaster cast for 5 to 7 days Ligaments loosen Potential Complications • • • • • • • • Pressure ulcers Skin allergy or irritation Swelling Cast slipped Circulation problems Rocker bottom foot Muscle atrophy Other Maintains correction To be worn for 3 months full time (23 hrs/day) To be worn for 2-3 years at night time only Failure to wear appropriately is the most common cause of recurrence - Ministry of Health - AIC CURE International Children’s Hospital - Association for the Physically Disabled of Kenya - Moi Teaching and Referral Hospital - Kenya Orthopaedic Association - Kenya Medical Training College To be continued……..