Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
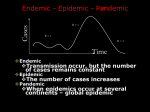
NCDs, alcohol and development: South Africa Clare Herrick Department of Geography King’s College London Outline • • • • NCDs and development NCDs and alcohol NCDs, alcohol and development in SA Concluding thoughts 1. NCDs and development The lack of data showing the interplay of risk factors, NCD burden and poverty has contributed to the neglect of NCDs by policymakers in developing countries (Schneider et al, 2009: 176) Why NCDs? • Social determinants of health agenda • Burden of disease calculations • Socio-spatial complexity of epidemiological transition(s) • Calculations of economic cost of NCDs to low and middle income countries - $7 trillion 2011-2025 • No longer "diseases of comfort" (Choi, 2005), but ones of poverty and “past and cumulative risks” (Beaglehole and Yach, 2003) WHO's Epic Tool - development? Labour Economic Output NCDs Capital Source: Abegunde et al (2006) Institutional momentum • WHO Global Status Report on the burden of NCDs • UN high level meeting September 2011 • NCD Alliance lobbying - Global Health agenda? • Critique of failure to realise MDGs - cannot work without inclusion of NCDs • Targets currently under debate But • NCDs as "market failure" or a "result of defective process of industrialisation that has given priority to economic growth over human welfare" (Frenk et al, 1989: 31) • Role of Geographic “luck“ or fate? (Kearns and Reid-Henry, 2010) • Wellbeing, quality of life and rights - income spent on healthcare is proportionally greatest for poorest. 2. NCDs and alcohol • Four major risk factors for NCDs: salt intake; exercise; smoking; drinking • Alcohol contributing factor to: cancers; CVD; liver disease and T2 Diabetes • Globally, 3rd most significant cause of DALYs lost • But 1st in middle income countries • Significant lack of data - habitual underreporting of drinking. Especially among men, North Africa and Middle East. For a given amount of consumption, poorer populations may experience disproportionately higher levels of alcohol-attributable harm (Blas and Sivasankara Kurup, 2011: 21) • WHO target = reduction of alcohol consumed per capita by 10% by 2020. • Long history of WHO engagement with alcohol, but only recent acknowledgment of NCDs and potential role in undermining developmental aspirations • May require fundamental re-conceptalisation of how and why alcohol is a problem and the potential solutions to this. 3. NCDs, alcohol and development in SA SA and NCDs • Mayosi et al (2009): quadruple burden of infectious, NCDs, perinatal and maternal • Why? Rising life expectancies and effects of urban poverty - poor diets, sedentarism, high salt intake, smoking (ie among coloured), drinking • Cause 40% mortality and 35% burden of disease • Rooted in inequalities in service provision, poverty and poor health literacy South African drinking • Dual economy -formal and informal • One of riskiest patterns of drinking in world heavy episodic as social norm • Liquor production and retailing long been form of state revenue and social control • Focus on formalisation of illegal sector • Significant market and world's second largest industry player Phuza... • Phuzagrain • Phuza-face • Phuza Thursday Many companies are saying to me Monday is our biggest problem. I’m saying I know there’s a fish Friday you know it’s Monday or Wednesday it’s the fish Friday but Monday there’s something that is going on. Go to the townships it’s happening . (Interview, 2011) SA and alcohol policy • • • • • 2003 National Liquor Act Need to update 1989 Provincial Acts 2012 Western Cape Liquor Bill promulgated City of Cape Town municipal by-laws Multi-sectoral team from health, social development, liquor board, SAP, metro police etc. • Still tensions between departmental goals and remits (ie health v dept for trade and industry) WCLB: • Formalisation or closure of shebeens • Land use zoning • Restricted opening hours • Limits on licenses in residential areas • Community involvement in licensing applications • enforcement at metro scale - complaints and tip offs - but conflict with SAPS. • No education component. • Policy driven by: violence, rape, injury, RTAs and drunk driving, crime, absenteeism, drugs. • NCDs have been absent from calls to curb alcohol consumption and abuse, despite burden of CVD, hypertension, T2 diabetes, cancers etc. • SA WHO target = 20% reduction in alcohol consumption by 2020 • Policy focuses on restricting access to deal with acute effects, not chronic consequences. • 'the poor also have a right to choose' 4. Concluding thoughts • Linking NCDs and alcohol necessitates thinking about risk behaviours and behaviour change in a more nuanced way, rather than trying to engineer risk out of environment (eg shebeens in Freedom Park), we need to better understand and acknowledge complexity of demand • Need to understand dynamics of consumption and points of intervention/ settings for this • Expanding role of CSR/ CSI • Need to communicate risks of drinking to change temporality of risk horizons • How to make data more accurate and representative. Success of interventions (i.e. shebeen closures measured through crime numbers not volume of liquor consumed little effect on NCDs) • Funding priorities shaping knowledge • Prevention must be prioritised, not treatment - but is evidence-based always best?