Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
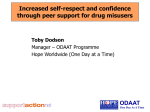
Key Learning Points Chris O’Sullivan Policy and Development Manager [email protected] Key Programmes of Work • Primary Care Mental Health Programme • Peer Support and Long Term Conditions Programme • Mainstreaming Mental Health Programme Primary Care Mental Health Programme Training and capacity building with primary care staff on mental health in long term conditions management, and with staff delivering Keep Well health checks Long Term Conditions Management • Developed as part of ‘Living Better’ programme • SG funded initiative working with 5 CHP and 10 GP practices across Scotland to address mental health and wellbeing in people with long term conditions. • In 4 CHP sites the focus is on diabetes and/or CHD and in 1 CHP site Chronic Obstructive Pulmonary Disease (COPD). • Patient workshops, leading to development of staff training based on discussing MH in LTC management Final report at http://bit.ly/12ktXxK Key Questions (PHQ-2) • During the last month, have you often been bothered by feeling down, depressed or hopeless? • During the last month, have you often been bothered by little interest or pleasure in doing things? Anticipatory Care Training • Keep Well Health checks for 45-65 year olds from deprived areas • Delivered by a range of staff • Covers a range of health risks and screening • Includes mental health, in different ways in different health boards • A challenge, because caseness can be very high • General session of social determinants of mental health, including both formal and informal aspects of MH • Discussion of risk and protective factors in their practice • Bridging from existing skills to mental health • Discussion on suicide and highlight specific trainings • Delivered across Scotland Peer Support for Long Term Conditions Amy Woodhouse, Senior Researcher “It’s a matter of coming to terms with things all the time, finding alternatives and luckily I’ve got interests and hobbies... But it’s something that I’ve had to work out myself, and I don’t think it’s been easy for me...or my partner for that matter.” (Male with CHD) • Evidence of Need (2008-2011) – Living Better Project (2008-2011) – focus groups and survey with 700 people with CHD, Diabetes or COPD. Participants reported: fear of the future, social isolation, low mood, anxiety, lack of confidence, financial concerns. Participants would like access to peer support to help with MH impact of LTC – Peer Support Feasibility Study (2011) found access to peer support was patchy and peer services often lacked ‘credibility’ • Impact and Model of Change (2012) – Networking events, guidance and local development support – Development and delivery of two new training courses – Training participants showed increased levels of knowledge and understanding of peer support and links between mental and physical health Mainstreaming Mental Health Training and capacity building with local authority and health board staff to connect their job roles to mental health and recovery outcomes. “It was really useful to have a day set aside to pull together this stuff. Some of it I knew, but I hadn’t had the chance to sit and connect the dots before” • Evidence of Need – Local Govt obligations under MH Legislation, and policy initiatives. – Originally commissioned by Glasgow City Council. Recommissioned by GCC, then by NHS Ayrshire and Arran and now Highland Council – Focus group research with service users and scoping phase with managers in local government/health to choose areas of focus. • Impact and Model of Change – Work with ‘non-traditional’ departments like environmental health to broaden MH message. – Statistically significant improvements in awareness. – Implementation of action plans. – Discussion of risk and protective factors for suicide, and signposted to local suicide prevention training. Seminar Structure and Content To increase understanding of determinants of mental health and mental ill-health To connect services and activities in the department to mental health and recovery objectives To collect good practice, and identify actions on a departmental and council level Learning Points • Mental Health Awareness – Expectations of mental illness awareness • Trojan Horse – Appreciation of MH role, but some indications for mental illness training (e.g. SMHFA/ ASIST/Something else) • Gatekeepers and Pioneers – Gatekeepers – staff who could assist people with mental health problems/poor MH to access services. – Pioneers – staff who come into contact with people who might not otherwise contact health or council services for help. • Enforcements Roles – Ensuring decisions made and communicated to minimise MH consequences on those affected, and solve problems for communities. • The Third Space – Coined by Glasgow Life, describing council services as the ‘third space’, i.e. not school/work or home, important for decompressing and relaxing • Mentally Healthy Workplace – Though not specifically in the training, most sessions included HR staff, and discussed mental health at work in that department Resilience key throughout the life Later Life course • • • • Young People • Schools and Education • Youth Services • Addressing youth unemployment • Intergenerational Activities • Supporting vulnerable groups Active Ageing Social Care Intergenerational Activities Independent Living Adults of Working Age Early Years • • • • • • Parenting Support Family learning Nursery provision Housing Greenspace Child protection • Public Sector Employee wellbeing • Employability • Complexity and Chaotic Lives • Independent Living • Homelessness • Crisis Support • Family Support • Opportunities for personal development -Housing -Green space -Protection of Vulnerable People -Environmental Health Connecting Role and Outcomes to MH is Key Finding and assessing impact of mental health in the context of challenges faced in job role Protecting and developing individual or community mental health through job related activities youth unemployment anti-social behaviour reduced budgets and service redesign youth work environmental health education housing planning Comparison of participants’ attitudes towards mental health improvement pre and post-workshop (Ayrshire) 95 100 90 98 95 87 90 80 80 70 62 60 45 50 40 30 20 10 0 Mental health promotion is I consider myself aware of I understand the factors that I am confident in my ability relevant to my everyday the importance of mental influence mental health and to develop activities or job*** health to overall health and wellbeing*** services which contribute to well-being*** improving public mental health*** Pre-workshop Post-workshop * p < .05; ** p < .01; *** p < .001 So… Public policy at national and local level has sought to mainstream mental health and inequality messages in Scotland, but these messages still need to be anchored at practice level People who live in areas of deprivation are subject to multiple, overlapping risk factors for poor mental health and suicide. This complexity is a challenge for statutory services and for community organisations alike. Men access community resources in relation to employability, physical ill health and welfare advice more often than they do in relation to emotional concerns or addictions. This can mean that emotional difficulties spring up in other contexts, and first contact is critical Existing suicide prevention training can be difficult to access as the time commitment of two days plus can be hard to arrange cover to attend. In addition these courses do not cover complexity and deprivation, nor on the needs of men as a particular risk group. It can be an easy assumption for those working on mental health that community organisations are more aware of the role mental health in wider health, poverty and complexity than they actually are.